
Abstract

The highly publicised case of the first ever partial facial transplant in 2005 sparked fierce ethical debates, moral arguments and strong opinions, both within the medical community as well as the general public and mass media. As more patients have undergone facial transplantation over the last decade, some of this initial scepticism has given way to a wider acceptance of this significant reconstructive development. However, despite an improved understanding of the perioperative technicalities and postoperative perils, the risks remain significant and the long-term outcomes are still largely unknown. This article examines the major ethical challenges that have accompanied facial allo-transplantation since its inception. We discuss these ethical dilemmas in the context of the patients, donor families, healthcare professionals and society as a whole, while evaluating some of the emerging evidence and outcomes associated with the physical and psycho-emotional risks linked to this procedure.
Lay summary
The highly publicised case of the first ever partial facial transplant in 2005 sparked fierce ethical debates, moral arguments and strong opinions, both within the medical community as well as the general public and mass media. This article debates some of the major ethical predicaments that have accompanied facial transplantation since its inception. We discuss these from the point of view of patients, donor families and healthcare professionals while incorporating some of the emerging evidence associated with the physical and psycho-emotional risks linked to this procedure.
Keywords
Introduction
The human face is often considered to be the focal point of a person’s identity, forming a strong representative of our self-perception, our ancestry and our ethnicity. 1 It is central to both verbal and non-verbal communication, recognition by others, expression of emotion and the conveying of intimacy to loved ones. It is also essential for some of our most vital functional human needs such as speech and articulation, oral intake, breathing and eye-opening.2–5
In an image-driven society where facial attractiveness and symmetry are markers of health, happiness and success, there is great impetus to achieve aesthetic perfection, or in the case of facial disfigurement, to achieve restoration of what is perceived to be normal and socially acceptable.
The highly publicised case of the first ever partial facial transplant in 2005 6 sparked fierce ethical debates, moral arguments and strong opinions from both the medical community as well as the general public and media: 7 was this the most significant development in facial reconstructive surgery to date or, this time, had medicine gone too far?
Since then, it is estimated that a total of 37 partial and full facial transplants have been undertaken across the globe 8 (Table 1). As the number of cases steadily increases and the scientific community amasses more information regarding the practicalities, risks, health implications and costs of these procedures, the ethical considerations are still a matter of great contention. These have been further highlighted in recent months following the death of the index case which, according to media outlet speculation, resulted from complications related to the patient’s immunosuppressive therapy. 9 Such outcomes further emphasise that the procedure is still in its experimental infancy. 10
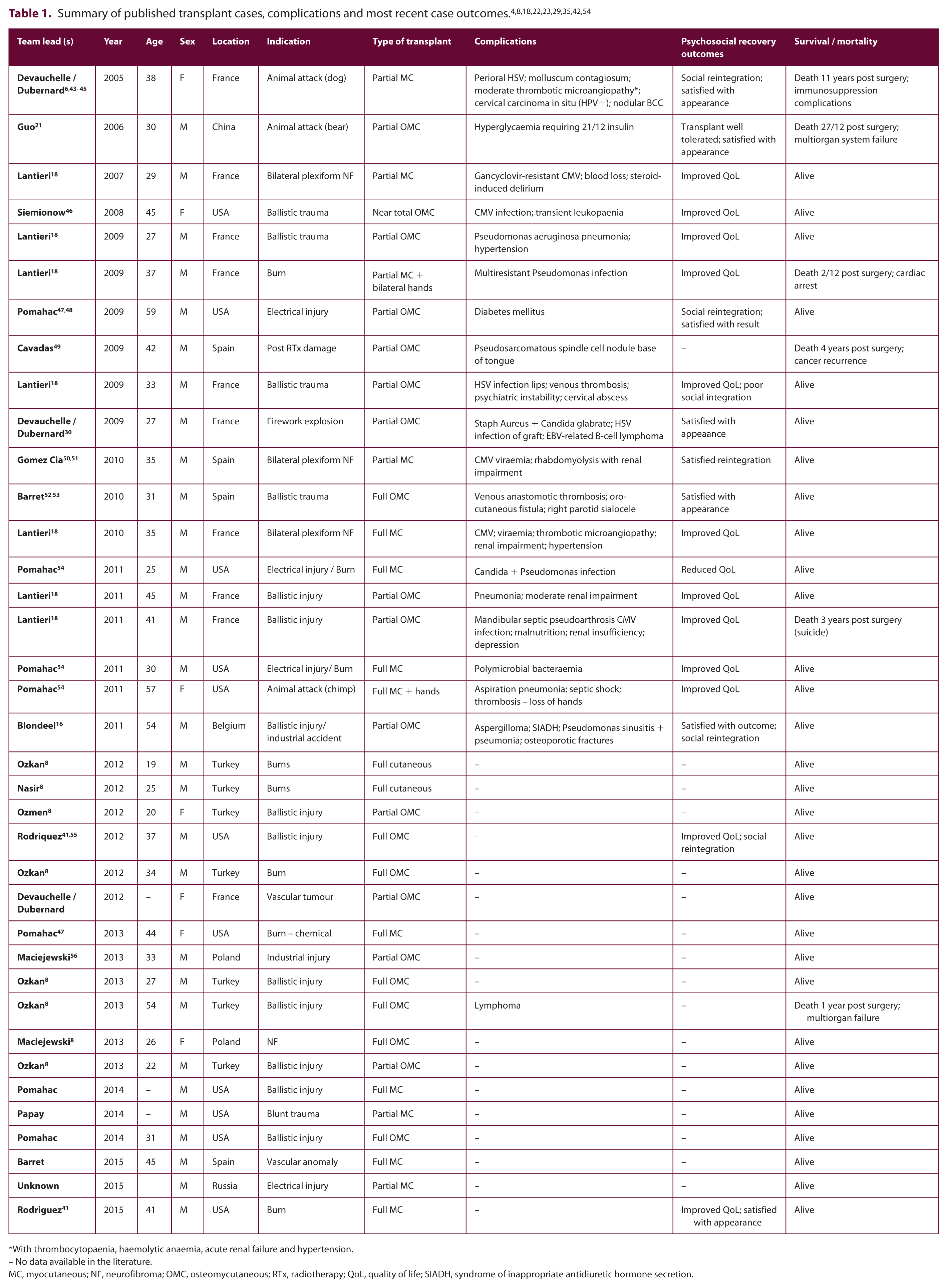
With thrombocytopaenia, haemolytic anaemia, acute renal failure and hypertension.
– No data available in the literature.
MC, myocutaneous; NF, neurofibroma; OMC, osteomycutaneous; RTx, radiotherapy; QoL, quality of life; SIADH, syndrome of inappropriate antidiuretic hormone secretion.
Although the indications for a facial transplant arguably are the same as those posed by other forms of reconstructive surgery or limb and organ transplantations—the restoration of health and function—the ethical considerations associated with facial allo-transplantation have unquestionably been far more challenging.2,11
This report evaluates and debates some of the pertinent ethical dilemmas that have accompanied the advent of facial transplantation since its inception against the backdrop of emerging evidence regarding patient outcomes and longer-term complications.
Discussion
Patient considerations
Loss of identity
Arguably, one of the main concerns posed by those who are opposed to, or sceptical of, facial transplantation has been the question of ‘loss of identity’ through the acquisition of a donor face. In acknowledging the integral role of our face plays in establishing our social, physical and psycho-emotional identity, it is understood why the concept of transferring this vital element of one’s self onto another has been a source of contention.
Interventions that alter the appearance of the face from the pre-morbid norm may potentially alter a patient’s self-worth, their very identity and how they are perceived by society. 12 Certainly, in the case of facial transplant surgery this potential skewing of self-identity is even further amplified, with some supporting that the difficulties patients may encounter in recognising the nuances of their former self and accepting their new external appearance are akin to those experienced when they sustained their original disfigurement. Both healthcare practitioners and patients must be weary that the dramatic change in a patient’s appearance may lead to a feeling of loss that requires a period of adjustment and even mourning for one’s old self. Even following a successful procedure and eventual acceptance of this new appearance, patients may continue to experience ongoing anxiety linked to the fear of transplant rejection. Similarly, there are concerns regarding how a patient may be perceived by their loved ones following such a significant alteration in appearance. Therefore they too require support and counselling throughout this process.2,11,13
As increasing evidence emerges on the cosmetic end-outcomes of facial transplant patients, it has been reported that patients tend to acquire a hybrid appearance incorporating their existing facial features with that of the donor, with the underlying bony skeleton of the recipient contributing far greater to the overall appearance.3,12,14,15 Allowing recipients to visualise what their appearance may resemble following the procedure has been made possible in some centres through the use of technology such as advanced three-dimensional (3D) imaging. Though the outcomes of such tools may not necessarily be perfect, this can provide patients with a greater degree of understanding as to what their postoperative appearance may entail and therefore minimise perioperative anxiety. 16
The candidate profile
A second point to consider is the idiosyncrasies of the patient population who tend to be candidates for facial reconstructive or transplant surgery. These patients may already be perceived as vulnerable or suffering with low self-esteem, often induced by the psycho-emotional trauma surrounding the original injury as well as the stigmatisation they face from society. This vulnerability often means that patients may be more inclined to pursue appearance-altering surgery in an attempt to free themselves of feelings of low self-worth, with little or no consideration for the perioperative risks. This was demonstrated in a study by Barker et al. where patients were shown to be willing to accept more risks for a facial transplant than for any other type of transplant, despite being informed of the risks of immunosuppression and rejection. 17
Although many authorities in the field would consider a pre-existing behavioural or affective disorder to be a contraindication to transplantation, it is interesting to point out that a significant portion of cases reported in the literature were patients with a past medical history of psychiatric illness whose facial deformities were a direct result of violent self-inflicted injuries, further highlighting the vulnerability of this patient cohort.18,19
Additionally, these patients’ expectations may be unrealistic, viewing surgery as the panacea that will rectify all their problems. As is seen throughout medicine, unrealistic expectations tend to go hand-in-hand with disappointment and resentment towards the healthcare team. Hence, it has been argued that the patients for whom the procedure is most indicated, physically and medically, may actually be the ones least suitable to deal with the aftermath emotionally and psychosocially. This paradox has been coined the ‘Catch-22’ of facial transplantation surgery in the literature and can pose a great challenge in the patient selection process.4,12,20 This was highlighted by the case of the second reported transplant patient, a 30-year-old man from China: the patient is believed to have had minimal social support following his surgery and at the behest of a local witch doctor stopped his immunosuppressive regime, eventually succumbing to multiorgan failure and becoming the first patient to die as a direct result of undergoing facial transplantation.21,22,23
Donor implications
A further problem that may arise revolves around the donor and their families: donor anonymity has been difficult to maintain as a result of extensive media coverage and publicity of such cases as well as the need to disclose some details pertaining to the donor’s medical background in published literature. This can greatly impact on the grieving process of the deceased’s family. Additionally, donor relatives may also perceive their loved one as still ‘living on’, preventing them from appropriately addressing and overcoming their grief. In extreme cases, there are concerns that this could even lead to an inappropriate need to contact or harass the recipient or conversely impart a perceived obligation upon the recipient to maintain communication with the donor family.11,24,25
Furthermore, it is essential to ensure that following the harvesting of facial tissues, the integrity of the donor’s facial appearance is restored as much as possible in order to minimise the distress endured by their loved ones. This is not only a moral obligation but in certain countries, also a legal one and requires the input of a skilled prosthetics team who should form part of the multidisciplinary team involved in facial transplantation. 26
Bioethics
Currently, ethical approval for facial transplantation cases falls under the remit of hospital and university ethics and research boards, subject to strict controls and guidelines. 3 Even so, critics and sceptics of facial transplantation argue that some of the most contentious ethical issues raised by this procedure are those of informed consent and non-maleficence. As facial transplantation becomes more widespread there will be an even greater onus for healthcare professionals to adhere to strict ethical conduct and ensure standards are kept meticulous and rigorous.
Is consent truly informed?
It can be argued that while the full implications, risks and chronic sequelae of a procedure have not yet been fully quantified, can patient consent be truly informed? In the strictest sense, proposing and undertaking such a procedure could be perceived to be a breach of patient autonomy and dignity because at this stage it is still impossible for healthcare professionals to offer a full and transparent explanation of what the procedure entails in the long term, simply because this still remains unknown.3,22 However, this is the case with all experimental procedures in their infancy and patients that are selected to undergo facial allo-transplantation and who agree to proceed do so after extensive counselling and an understanding of the uncertainty of long-term outcomes and peri-procedural risks.
With highly experimental treatment in patients where all other options have failed, however, it is important to consider whether the patient is being driven to accept a facial transplant in a desperate means of ridding themselves of disfigurement and conversely, whether the teams of experts in the field, influenced by their enthusiasm for this novel procedure may be inadvertently, subtly or unknowingly influencing the patient’s choice.3,11
The role of the healthcare team: Are we doing ‘no harm’?
The ethical ramifications also lie within the healthcare team and operating surgeons. It is unquestionable that a patient living with facial disfigurement may be dealing with an immense amount of suffering and prejudice, but opponents of facial transplantation argue that this is not a strong enough indication to undergo radical surgical treatment which may have no actual medical or therapeutic indications and which may lead to greater psycho-physical problems postoperatively. Is an operation with potentially severe repercussions appropriate when there are no life-saving or health-preserving justifications? And in offering such treatment to patients are we breaching the values of ‘non-maleficence’? Critics have voiced that they do not consider it acting in the patient’s best interest to subject them to a procedure that takes them from being disfigured but physically ‘healthy’ to having a more ‘normalised’ appearance at the expense of their physical health. 7 Arguably, thousands of facial aesthetic surgeons perform appearance-altering, non-therapeutic operations on a daily basis; however, undergoing a procedure that rejuvenates or rectifies a localised grievance, such as a deviated nose, does not carry the same implications as a facial transplant.
Additionally, the public’s perception of the medical professsion can easily be tainted by controversial procedures such as these, branding them as being above ‘natural laws’, above religious beliefs and above what was previously considered scientifically possible. This can subsequently lead to an attitide of mistrust and hostility towards the medical field.
Nevertheless, it cannot be denied that, although facial transplantation may not constitute a life-saving treatment, it can certainly improve or restore the quality of the recipient’s life, which has been a vital driving force for a wide array of surgical interventions, despite their recognised risks. As per the World Health Organization definition of health, it is ‘a state of complete physical, mental and social well-being and not merely the absence of disease of infirmity’ and this must always be kept in mind when evaluating patients with facial disfigurement. Additionally, proponents of facial transplantation also point out that if the transplant is successful then the patient will be saved from potential multiple reconstructive procedures which are known to have sub-optimal functional and aesthetic results and which can further contribute to patient distress and prolong their suffering.3,20 In this sense, if a medical professional offers a facial transplant to a carefully selected, scrupulously counselled patient who would benefit physically and psychosocially then arguably they are acting in the patient’s best interest and within the scope of ‘beneficence’. 3 This is supported in the Declaration of Helsinki and is often accepted in the context of novel, experimental procedures where risks are not yet fully understood but where there is felt there could be a benefit to patients’ health. 27
Immunosuppression
One of the most important recognised risks associated with the procedure is that for long-term immunosuppressive therapy which will predispose patients to a whole gamut of other health problems: the incidence of malignancy, infection and metabolic disorders in patients undergoing facial transplantation is well-recognised (Table 1).10,28 Furthermore, treatment requires long-term patient compliance and health awareness. This is especially true when considering the high antigenicity of facial tissue and the subsequent high risks of tissue rejection.3,11 All reported cases showed evidence of acute rejection in the first year post transplant and this neccessitated an increase in the immunosuppressive regimen, which further augmented the risks.8,29 Recent reports have also now described a case of chronic rejection occuring in a 27-year-old male patient operated on by the Amiens group in France. This further underlies that we are still lacking long-term data that would enable a robust understanding of the likely associated risks and their chronicty.8,30
Financial implications
As facial transplantation starts to be used more widely, the issue of financial burden will begin to surface. This is an extremely contentious subject in a time when healthcare provision is being rationed by the state and resources and personnel are already stretched to their limits. Thus far the procedures have been carried out under the remit of research and healthcare institutions, military establishments and other sources of private and public funding. In addition to the costs of the index procedure itself, facial transplantation also continues to incur costs in the long term due to lifelong immunosuppression, the treatment of emerging complications and follow-up surgical interventions. Although the cost of a single face transplant has been demonstrated to be similar to that incurred by the multiple conventional reconstructions the patients undergo pre-transplant, it is the ongoing demand for interventions and resources postoperatively that exponentially drives up the cost.22,25,31,32 Although one could argue that giving patients the best treatment option necessary to restore their quality of life is worth the expenses incurred, the reality is that in our current healthcare system, funding is limited and invariably one questions whether the vast sums used to carry out and support a single facial transplant would therefore be unavailable for other treatments which may be life-saving. With the attenuation of financial resources for the upkeep of such costly procedures, it is not unlikely that facial transplantation may eventually only be offered those able to afford it, further propagating health inequality and breaching the ethical pillar of ‘justice’. This allocation of resources will no doubt pose a great challenge health policy-makers in coming years.
The need for scrupulous patient selection
With increasing publicity, social acceptance and more centres offering this procedure, an increasing number of patients may start to request facial transplants at a greater rate than there is an availability of donors, and this is associated with the increased and well-recognised anxiety of being on a transplant waiting list. And to what extent will patients and their families be given a choice in which donor they would accept a facial transplant from? Would it be appropriate for patients to reject a face depending on their perception of attractiveness? 2 And who will be entitled to a transplant as this procedure becomes more commonplace and easily accessible? A severely disfigured burns survivor, an attack victim? Or will this extend to a dysmophophobic patient, a person with adequate disposable income looking to alter themselves or even a criminal who wants to change their appearance? Could this lead to further transplant-associated crime, akin to that seen with black-market organ donation?
Nevertheless, despite these potential extreme scenarios of a post-humanist existence, the reality remains that currently, this procedure is offered to severely disfigured patients in whom other reconstructive options have failed. The process is conducted under strict conditions of patient selection and cautious considerations throughout by teams of highly qualified healthcare professionals in respected reconstructive centres and within the safety net of carefully regulated clinical research initiatives.4,33 Despite this, as mentioned before, several of the patients receiving transplants had pre-existing psycho-emotional disturbance, including alcohol dependency, and this translated into poor compliance, poor social re-integration and lower objective measures of quality of life. 18
It is essential that patients undergo rigorous evaluation on the basis of stringent criteria, give their consent in an informed manner, have a robust social and family network, be physically and emotionally suitable to receive the transplant and be fully aware of the postoperative ramifications.34–36 Planning for the procedure has been known to take years, which is the level of meticulousness demanded by an operation riddled with such technical and ethical considerations. What has been highlighted by the heterogenous nature of the patient cohort that has undergone facial transplantation thus far, is that the implementation of strict guidelines and selection criteria may be challenging. 16
With the risks and benefits not fully known yet in view of the early stages of the procedure’s development, the need for extensive scrutiny from an ethical point of view and the need to be guided by strict recommendations and guidelines is even more essential; after all, the procedure is still considered to be experimental by even the utmost experts in the field.10,37,38 The procedure must only be offered in selected qualified centres with full multidisciplinary representation including that of psycho-social support where the needs of patients and donor families can be addressed before, during and after the process.3,11,38–41 Cultural implications must also be taken into consideration as evidence has shown that the willingness to receive and/or donate a facial transplant is strongly linked to cultural, religious and societal idiosyncrasies. 24 It is therefore paramount that advancing technologies such as this are addressed sensitively, professionally and with ongoing participation from interested stakeholders and the public.
A gradual shift in attitudes?
The scientific community is very gradually starting to gain a better understanding of the risks and longer-term outcomes and the procedure is now being more frequently considered as a reconstructive option for severely disfigured patients.7,14,15 The small group of experts in the field will often quote the fears expressed by the public and media as sensationalistic and argue that based on their own, albeit limited, experiences with facial transplantation the procedure is not only indicated medically, but also justified ethically. 20 As more information emerges with time, it appears that, yes the risks are high and unquestionable but the benefits too have been immense, with patients reporting increased satisfaction with their appearance, positive reintegration into society and improvement in their quality of life. There have been no reports to date regarding problems with self-identity and perception. 10 Additionally, results pertaining to functional outcome have been promising which has helped to further promote facial transplantation as a feasible reconstructive option.4,29
Yet the question remains: with the vast majority of the psycho-emotional suffering experienced by a disfigured individual being a direct result of societal perception, is it not important to also target ignorance, promote acceptance and educate adults as well as children at a young age to show kindness and compassion to those who are different rather than propose that the solution lies in patients undergoing surgery? Are we accepting that if your own appearance doesn’t make you worthy of acceptance by society because it is deformed, then conforming to a predetermined notion of normality will? Mild alteration in the wording of this paragraph: “The growing role of charity organisations such as ‘Changing Faces’ in the United Kingdom has been integral in addressing these very issues by not only helping individuals with facial deformities accept themselves, develop their self-esteem and achieve a fulfilled quality of life, but also by educating the public and altering long-engrained discrimination and fear and campaigning for equality and equal opportunities.”
The medical reality
Despite the gradual attenuation of the initial scepticism, critics of the procedure continue to argue that facial transplantation carries a host of risks that outweigh the benefits. The procedure is still associated with significant morbidity and mortality and as the recent death of the index case has highlighted, patients are still susceptible to transplant-associated risks, even years following the initial operation. 34 Six deaths have been reported to date with an estimated 37 patients having undergone the procedure. Causation of death has been attributed to both iatrogenic complications in the immediate and long-term period, as well as psycho-emotional demise leading to suicide.23,42 Furthermore, as is demonstrated in Table 1, every case formally reported in peer-reviewed literature experienced a range of postoperative complications ranging from acute rejection, opportunistic infections of varying severity, prolonged hospitalisation and malignancy.
Another issue which has become apparent is the significant under-reporting of a large number of cases in the medical literature, especially in recent years. Often, information is only available through media outlets with no official data from the operating teams, in stark contrast to the flurry of debate and communication witnessed initially within the scientific community. When dealing with a novel procedure with so many unknowns, it is essential that medical reporting is kept up-to-date and that information is pooled and shared as a means of propagating knowledge, avoiding pitfalls and improving outcomes. 8 This also translates to transparency and accountability by the healthcare teams meaning that standards and regulations remain high.
Conclusion
The ethical ramifications associated with facial transplantation have been well recognised and extensively debated over the last decade. With steadily growing numbers of patients undergoing this novel and controversial procedure, the medical community is increasingly becoming better equipped at addressing the associated moral quandaries. Ongoing education and exchange of ideas and experiences within the international medical community will be vital in enabling the propagation of knowledge and the development of expertise which will allow the risks of such technically and ethically challenging surgery to be understood and further developed allowing facial transplant patients to have access to the best care, optimal outcomes and quality of life.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.