
Abstract
The profession of orchestral musician is often linked to musculoskeletal problems, hearing disorders, and struggles with stage fright. However, data on the prevalence of physical problems are very divergent because of different research methods and sampling procedures. It is to be expected that physical problems generally increase with age, but the literature on medical issues that affect musicians contains very few studies on this aspect. In light of this, the data produced by a cross-sectional study of 2,536 musicians from 133 professional symphony orchestras in Germany were analyzed with regard to a number of health aspects. The data from 894 female (36%) and 1,607 male (64%) professional orchestral musicians aged between 20 and 69 (M = 45.5, SD = 9.52) were used to study physical problems, their duration and intensity, and psychological difficulties (such as pressure to perform in the orchestra and stage fright) in conjunction with variables such as age, gender, instrument family, position in the orchestra, and category of orchestra. The various health problems were also examined in relation to health behaviors, including preventative actions taken (nutrition, sleep, etc.). The results showed that more than one in two (55%) of the orchestral musicians who took part in the survey were suffering at the time from physical problems that affected their playing. The prevalence increased significantly with advancing age, and string players and harpists had an above-average frequency of experiencing physical problems. Interestingly, there was no significant correlation between the severity of problems and different health behaviors (including preventative action). Around half (49%) of the orchestral musicians said they felt the pressure to perform was intensifying, something that they partly attributed to an increase in artistic demands. The findings are discussed with reference to existing empirical results, potential methods of prevention and treatment, social aspects, and health-care policies.
Keywords
Theoretical background
With their large-scale cross-sectional study of 2,536 orchestral musicians from 133 professional symphony orchestras in Germany, Gembris and Heye (2012, 2014) examined the effects of the aging process and musicians’ perceptions of aging on their musical performance and other aspects of their profession. They studied age-related changes in musical performance and other aspects such as professional stresses, pressure to perform, and physical problems. Although the main focus of the study was not on the health issues that affect professional musicians, the link between aging and health is of vital importance to the ability to play music and maintain the best possible performance throughout a musician’s professional life. This is why the connection between physical problems and aging was included in the study on participants’ growing older in a symphony orchestra. This article presents the key findings of this study of professional orchestral musicians with regard to the links among age/aging, physical problems, psychological conditions, and their prevention.
Studies in the medical field have highlighted a range of physical and mental problems that are experienced by professional musicians. The most common problems are playing-related musculoskeletal disorders (PRMDs). The oft-quoted study by Fishbein, Middlestadt, Ottati, Straus, and Ellis (1988) involving 2,212 professional orchestral musicians from 47 different orchestras showed that 82% of these musicians suffered from playing-related health problems. Musculoskeletal pain (back, neck, and shoulders) was the most common problem (mentioned by 20–22% of the respondents). A proportion of 76% of musicians said they had at least one health problem that had a negative effect on their playing. In a survey of string players (N = 1,432), Blum (1995) found that the overwhelming majority suffered from musculoskeletal problems (86%). Other studies have confirmed these findings (see literature review by Spahn and Möller, 2011, pp. 7–17). More recent studies have shown that this problem has not improved, and indeed it seems to be worsening. In her review of the literature, Steinmetz (2015a, 2015b) noted that 89% of musicians said they suffered from PRMDs. However, the prevalence of PRMD ranged from 43% to 89% among music students and professional musicians. The wide range of data contained in the various studies on the prevalence of PRMDs has led Steinmetz to the conclusion that there is not one standardized definition of these syndromes and that they can be operationalized in different ways.
A study carried out by Paarup, Baelum, Holm, Manniche, and Wedderkoop (2011) showed that 97% of female orchestral musicians and 83% of male musicians had at some point experienced musculoskeletal pain (N = 441). Woodwind players were less severely affected than string players. A comparison with a representative control sample of the working population showed that musculoskeletal disorders were generally more prevalent and longer lasting in musicians.
It is interesting to note that there was only a weak correlation between perceived problems on the one hand and manifest clinical findings on the other (Paarup, Baelum, Manniche, Holm, & Wedderkopp, 2012). Paarup et al. (2012) believe this was probably due to the fact that the musicians were still working at the time of the survey, so they were probably relatively healthy at that point. The weak correlation could also be put down to the fluctuating nature of musculoskeletal problems and to the basic problem of the often weak covariation between verbal data and clinical findings.
In general, female musicians seem to suffer musculoskeletal problems more frequently than their male colleagues and string players more often than players of other instruments (see also Berque, Grey, & McFadyen, 2016; Kenny & Ackermann, 2013; Leaver, Harris, & Palmer, 2011; Steinmetz 2015a; Wallace, Klinge, & Chesky, 2016). Unlike other studies, in their survey of 377 professional Australian orchestral musicians, Kenny and Ackermann (2013) found no statistically significant differences between the players of various instruments in terms of the prevalence of problems.
The findings on the correlation between age and playing-related pain are somewhat contradictory. In a more recent study by Kenny and Ackermann (2013), musicians between the ages of 41 and 50 said they suffered more frequent and intense pains than both younger and older musicians (18–68 years old). An older study by Fishbein et al. (1988) showed that problems were most likely to arise at the age of 35. Berque et al. (2016) also found that the prevalence of musculoskeletal problems increased with age.
On the basis of detailed data provided by the report Health in Germany (Robert Koch Institut, 2015), in general it seems safe to assume that the prevalence of musculoskeletal disorders increases with age and that women are more severely affected than men. Social status also has a role to play. Across all age-groups, people of lower social rank are more likely to suffer from musculoskeletal problems than the middle and upper classes. For example, 20% of middle-class men and 25% of middle-class women aged between 45 and 64 say they suffer from back pain, but the figures fall to 13% for men and 18% for women who have a higher social status. The frequency of back pain is much lower among the general population than professional musicians, who not only suffer from back pain but also pain in the arms, hands, fingers, and so on.
A number of systematic literature reviews have been carried out to assess the state of current research on physical problems suffered by professional orchestral musicians (see Bragge, Bialocerkowski, & McMeeken, 2006; Baadjou, Roussel, Verbunt, Smeets, & de Bie, 2016; Moraes & Antunes, 2012; Kenny & Ackermann, 2013; Kok, Huisstede, Voorn, Schoones, & Nekissen, 2016; Wu, 2007; Zaza, 1998). These reviews look at risk factors, professional consequences, and various approaches to prevention and treatment with regard to physical problems (Chan & Ackermann, 2014; Chan, Driscoll, & Ackermann, 2013; Kaufman-Cohen & Ratzon, 2011; Molsberger & Molsberger, 2012).
Another health risk for orchestral musicians is noise exposure and the potential for permanent hearing damage (Emmerich, Rudel, & Richter, 2008; Rodrigues, Freitas, Neves, & Silva, 2014). Brass and woodwind players and percussionists are at particular risk of being exposed to sound levels in excess of 85 dB 1 , which can cause permanent hearing damage. Musicians, such as percussionists, may be exposed to levels as high as 135 dB, so they face an objective risk (see Rodrigues et al., 2014). A study of Canadian musicians showed that players of instruments with the highest noise exposure (brass and woodwind players, percussionists) had the highest auditory threshold, but the findings on hearing loss were not clinically relevant in any of the instrument families (Russo, Behar, Chasin, & Mosher, 2013). Kähäri, Axelsson, Hellström, and Zachau (2001a, 2001b) also found that woodwind players and percussionists had slightly lower auditory threshold results than players of other instruments, but overall they found no significant differences between the various instrument families, and they could not prove that hearing loss was attributed to loud music. On the other hand, a study of Swedish musicians showed that 40–57% of respondents had hearing disorders (such as tinnitus, hypersensitivity, and hearing loss). The self-reported hearing problems were associated with a weak psychosocial environment (e.g., friends, acquaintances, family, etc.), psychological problems, and stress. There was also a correlation with increased heart rate variability, which may be an indicator that some found it difficult to switch off and relax (Hasson, Theorell, Liljeholm-Johansson, & Canlon, 2009). Overall, research into music-induced hearing loss in professional musicians remains heterogeneous and unclear (Richter, 2011). As Richter (2011, p. 274) stated, there are many studies describing the risk that over time, the high levels of noise exposure when playing an instrument cause hearing loss. Indeed, there are studies confirming this assumption. On the other hand, other studies do not confirm the assumptions of occupational hearing impairment in musicians. They show that musicians may be surprisingly resilient and have normal hearing, even after years of being subjected to high noise levels. However, these findings must be treated with caution because of the different research methods used and because very few longitudinal studies have been carried out in this respect.
There has been very little research on the correlation between aging and physical problems among musicians. Lederman (1999) describes a number of age-related limitations (such as the slowdown of neuron processing, reduction in muscle mass, and loss of sensory functions) and diseases (such as strokes, dementia and Parkinson’s disease), all of which occur more frequently as people grow older and affect the playing ability of professional musicians. But individuals vary widely in terms of the prevalence and extent of age-related limitations, depending on their particular disposition and personal situation. Berque et al. (2016) examined the prevalence of musculoskeletal problems in professional orchestral musicians and found that musicians who suffered with PRMDs were on average 5 years older than those who did not (50 vs. 45 years old).
Henoch and Chesky (1999) highlight the correlations between advancing age and increasing hearing loss and state that very little is known about how aging affects musicians’ hearing. For example, older epidemiological data from the U.S. National Health Interview Survey carried out in the 1980s show that around 40% of men and 20% of women aged between 50 and 59 suffered from hearing loss, whereas the figure for the 20–29 age-group was below 10%. In contrast, 20% of musicians aged between 20 and 29 already had symptoms of hearing damage. Musicians were more likely to have hearing problems by the time they reached their 40s, but then the situation went into reverse. The incidence of hearing disorders increased more slowly than among the reference population (cf. Henoch & Chesky, 1999, p. 78).
Kenny, Driscoll, and Ackermann (2012) noted that orchestral musicians suffer less from stage fright and social anxiety as they grow older. However, they did not interpret this as an effect of aging, but as a cohort effect that arises because it is the most resilient musicians who stay in the orchestra while those who are more prone to stress are likely to leave.
This article analyses the detailed data provided by the study “Growing Older in a Symphony Orchestra” (Gembris & Heye, 2012, 2014) to investigate the correlation between physical problems, preventative behaviors, and coping strategies on the one hand, and the variables of age, instrument, gender, position in the orchestra, different categories of orchestra, and occupational stress on the other.
Method
The study “Growing Older in a Symphony Orchestra” was carried out in collaboration with the German Orchestra Union (Deutsche Orchestervereinigung, DOV). The DOV is the biggest professional organization and union of orchestral musicians with close to 10,000 members.
For the study, a comprehensive survey was carried out involving all 133 Kulturorchester 2 existing in Germany at the time of data collection. As aging is an ongoing process, it makes little sense to attempt to identify a particular age or age range for studying the topic of growing older in a symphony orchestra. We therefore included orchestral musicians of all ages. This also made it possible to include the experiences and opinions of different generations. A second argument for carrying out a comprehensive survey was that a number of organizational and methodological reasons made it very difficult to set up a suitable sample.
In order to make the questions posed in the survey as relevant as possible to the everyday reality of orchestral musicians, we initially carried out a pilot qualitative study with N = 12 musicians (9 males and 3 females). They played different instruments and belonged to different orchestra sections, were between 48 and 72 years of age, and had between 20 and 40 years’ experience in professional orchestras (for more details, see Gembris & Heye, 2012, pp. 26–38).
On the basis of these interviews and the relevant literature, we developed a comprehensive standard questionnaire. We pretested the questionnaire on a group of 11 professional musicians and then revised it accordingly. The final questionnaire ran to 245 questions/resp. items over 19 pages and was divided into seven sections: general demographic information (age, gender, etc.); current employment (instrument, type of orchestra, position, etc.); the pros and cons of playing in an orchestra (questions about job satisfaction, perceived performance, pressure to perform, stage fright, etc. and how these change over time); health aspects (questions about physical problems, health care, etc.); crises and conflicts (professional difficulties, personal relationships within the orchestra, managing stress, etc.); getting older (perceptions of one’s age, declining performance as a result of aging and how to cope with this, attitudes to age and aging, etc.); and retirement (attitudes towards retirement and part-time work).
Procedures
The survey was carried out between October 2010 and February 2011. A total of 9,922 questionnaires with return envelopes were sent out via the German Orchestra Union to the 133 Kulturorchester. A cover letter explained the purpose of the questionnaire. In general, the completed questionnaires were collected from the orchestras anonymously in sealed envelopes by DOV representatives and sent to the DOV office in Berlin. Here, the questionnaires were collected and sent back to the Institute for Research on Musical Ability (Institut für Begabungsforschung in der Musik, IBFM) at the University of Paderborn, Germany.
In total, N = 2,550 musicians returned questionnaires (a return rate of 26%) and N = 2,536 of these questionnaires were included in the SPSS data analysis.
Analysis
The following procedures were used to analyze the variables for each question or scale: a χ2 test (effect size: Phi and Cramer’s V), a t-test for independent samples (effect size: d and δ), variance analysis (effect size: η 2 ) for multilevel independent variables with the Scheffé test as a post-hoc test, binary logistic regression, and (Pearson) correlation. As we had intended to use a number of items (10) for calculating the construct “health behaviors,” we calculated the internal consistency (Cronbach’s α) of the scale and the corrected selectivity of the items. The factor values of a univariate factor analysis were calculated in order to produce a score summing up the health behavior.
Results
Participants
A number of musicians (N = 2,536) aged from 20 to 69 years (M = 45.8 years, SD = 9.52) were included in the data analyses (36% female, 64% male). Among them were 1,359 string players (54%), 993 wind instrument players (40%), 113 percussionists (5%), and 41 harpists (2%). The majority of them came from Germany (82%), with a smaller number from other countries (e.g., Romania [3%], the U.S., Austria, Poland [2% each], Japan, and Hungary [1% each]). Table A1 shows players in each instrument family broken down by age and gender.
On average, the musicians had 22 years’ experience as professional musicians (M = 21.6, SD = 10.14, range = 0.3–48 years); their experience in the orchestra they were playing with at the time of the survey was on average 19 years (M = 18.5, SD = 10.0, range = 0.1–42 years). More than half (56%) of the participants had 20 or more years’ experience as orchestral musicians.
We also surveyed musicians in orchestra categories A to D. Categories A to D relate to the size and pay scales that apply to Kulturorchester. Opera orchestras with fewer than 56 positions belong to Category D; orchestras with 56–65 positions are Category C; those with 66–98 positions are Category B; and orchestras with 99 or more positions are described as Category A. The groupings can also be interpreted as a performance indicator (see Mertens, 2016). The best, top-level orchestras belong to Category A. Musicians from Category A orchestras (54%) and B (35%) represented the largest part in our sample. This also included 7% of musicians from Category C and 5% from Category D.
A distinction was drawn between soloists (27%, n = 436) and non-soloists (73%, n = 1,173), so that we could assess potential differences between musicians’ positions in the orchestra. The other positions involved 3 were principals (9%, n = 231), assistant principals (10%, n = 232), coprincipals (6%, n = 149), and concertmasters (3%, n = 62), but these were not taken into account when differentiating between positions.
By comparing this sample with official statistics provided by the DOV on age structure, gender distribution, and origin, our study can be considered to be representative.
Professional orchestral musicians and health issues
The questionnaire “Growing Older in a Symphony Orchestra” covers a number of health issues that affect orchestral musicians. The focus of this article is on physical problems that may have an effect on musicians’ playing abilities. It also examines psychological issues. Along with assessing their own physical and mental condition, the musicians were also asked about their health behaviors. They provided information about the specific strategies they use to manage physical and mental problems and the preventative actions they take in order to maintain their health.
Physical problems
At the time the survey was carried out, just over half of orchestral musicians (55%, n = 1,396) had physical problems that affected their playing. There were significant differences in the frequency of physical problems between different age-groups as well as between different instrument families.
Older musicians suffered from physical problems much more frequently than their younger colleagues (χ2 = 132.36, p < .001, Phi = .255; Figure 1). However, 28% of the musicians in the under-30 age-group also said they have physical problems. By the age of 40, the percentage of musicians with physical problems was higher than the percentage without problems (cf. Figure 1). This increased with age to reach 69% of 55–59-year-olds, well above the total average of 55%. The fact that a slightly lower percentage (67%) of musicians in the 60+ age-group reported physical problems was probably due to the fact that musicians with more major problems are likely to have already left the orchestra, while the “healthier” musicians have remained in the older age-group.

Frequency of physical problems by age-group.
There were significant differences among string players, wind instrument players, percussionists, and harpists (χ2 = 61.30, p < .001, Phi = .156). String players (62%) and harpists (61%) suffer from physical problems that affected their playing more frequently than wind instrument players (47%) and percussionists (39%). This effect was consistent for both male and female musicians. The kind of instrument played a significant role with regard to physical problems, but the effect size was very small (Phi ≤ .10). No significant differences were noted between different categories of orchestras. This suggests that the physical problems of orchestral musicians are not linked to the size or type of orchestra.
Types of physical problems
The musicians who suffered from physical problems mentioned six different types of physical problems: musculoskeletal (bones, muscles, and joints), hearing, cardiovascular, respiratory (breathing/lungs), visual, and those connected with the nervous system (e.g., pinched nerves such as with carpal tunnel syndrome).
Musculoskeletal problems were the most common, with 83% of respondents saying they suffered from them. Around one third (34%) said they had problems with their hearing. Another section in the questionnaire asked whether the musicians had ever been medically diagnosed with a hearing disorder such as hearing loss or tinnitus. A total of 38% responded that this was the case. The nervous (12%), cardiovascular (10%), visual (6%), and respiratory systems (5%) were mentioned much less frequently (Figure 2).

Frequency of problems in different physical areas.
Some specific physical problems showed significant differences in terms of the variables age, gender, and instrument family.
There were also significant age differences with regard to the frequency of hearing problems (χ2 = 39.99, p < .001, Cramer’s V = .171), cardiovascular problems (χ2 = 31.37, p < .001, Cramer’s V = .151), and nervous system disorders (χ2 = 18.18, p < .001, Cramer’s V = .115). These kinds of problems tended to increase with advancing age (Figure 3).
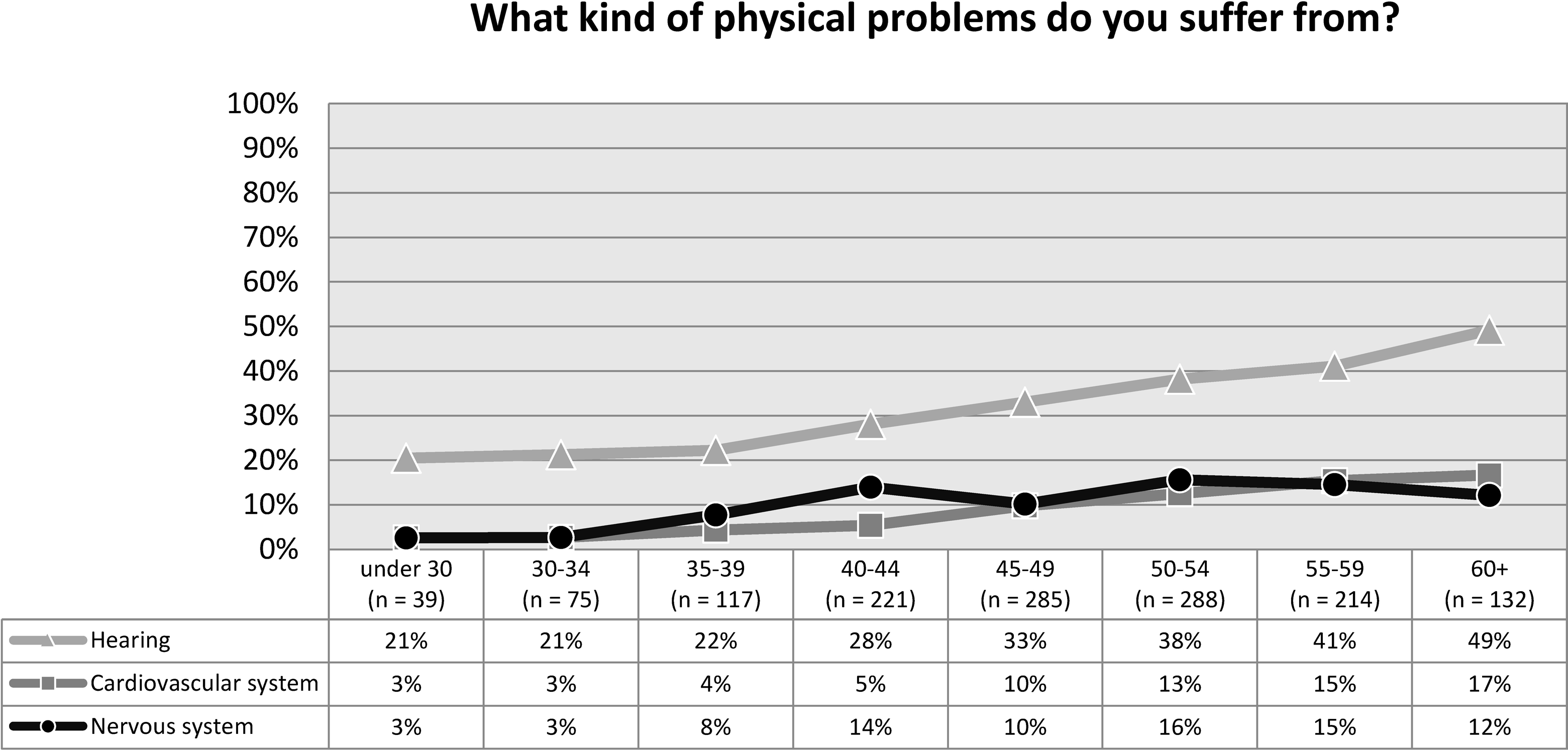
Percentages for different physical problem areas by age-group.
About a fifth (19%) of musicians under the age of 30 said they had already been diagnosed with hearing disorders such as hearing loss and tinnitus. The number of people with hearing problems increased considerably with age, reaching 45–46% in the over-55 age-group (Figure 4).

Diagnosed hearing disorders by age-group.
Data analysis showed that belonging to a particular section of the orchestra, category of orchestra, or being a soloist or non-soloist had no effect on the probability of being diagnosed with a hearing disorder (binary logistic regression; omnibus test not significant, χ2 [7] = 11.383, p > .05).
Female musicians (91%) were significantly more likely to suffer from musculoskeletal problems than their male colleagues (78%; χ2 = 38.60, p < .001, Phi = .168). Overall, it can be concluded that string players (90%) and harpists (92%) had an above-average likelihood of suffering from musculoskeletal problems. Wind instrument players (10%) were twice as likely to suffer from respiratory problems than the average (5%). Percussionists had an above-average frequency of hearing problems, with about one in two (55%) mentioning problems in this area.
Time when initial physical problems arose and duration
In order to identify when the initial physical problems arose, we asked the musicians how many months or years they had had physical problems. The time the problem arose was calculated in conjunction with their current age. This showed that the average age when physical problems arose was 37 for female musicians (M = 37.4, SD = 10.21) and 41 for male musicians (M = 40.7, SD = 9.72). Female orchestral musicians began to suffer physical problems significantly earlier than their male colleagues, t = −5.824, df = 1239, p < .001, d = −0.34. This is shown in the gender-specific distribution of the age range when the initial problems began (Figure 5). More women than men began experiencing physical problems in the first three age-groups (“up to and including 20 years old,” “21–30 years,” and “31–40 years”). Men were overrepresented in the following age-groups: “41–50 years” and “51 years and older” (Figure 5).
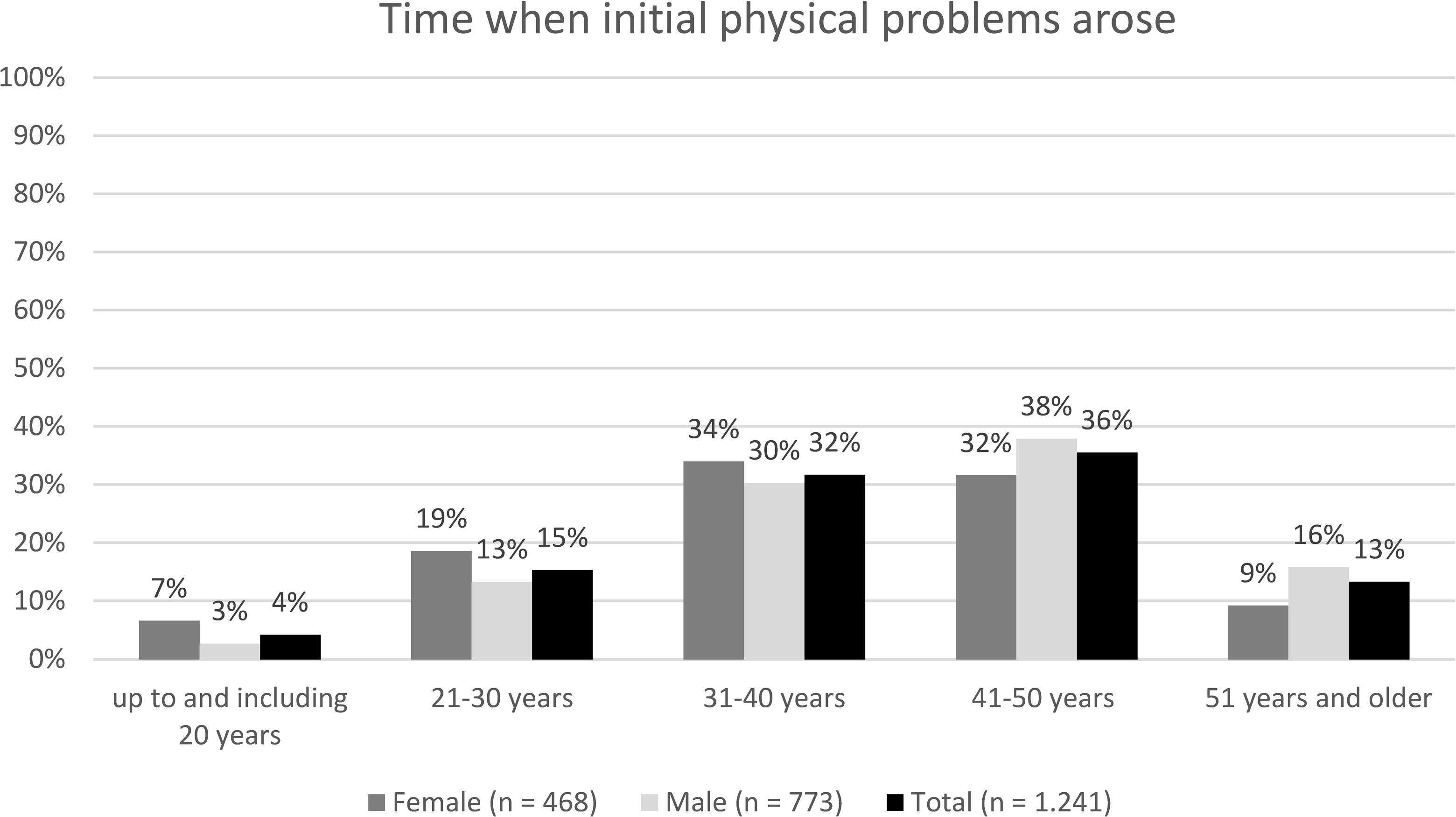
Time when initial physical problems arose.
The duration of the physical problems was, however, almost the same for female (M = 8.8, SD = 7.58) and male (M = 8.6, SD = 7.12) musicians, with an average of around 9 years (M = 8.7, SD = 7.38). The very wide range of responses from 1 month to 51 years meant that the median was calculated as a supplementary situation parameter. This amounted to 6 years (Mdn = 6), meaning that 50% of orchestral musicians said they had been suffering from physical problems for more than 6 years. The remaining 50% had had physical problems for less than 6 years. Figure 6 shows that in the majority (71%) of cases, physical problems lasted between 1 and 10 years. There was also a weak positive correlation between age and duration of problems. The correlation according to Pearson was certainly significant, p < .01, but the correlation coefficient of r = .227 showed that it was weak.
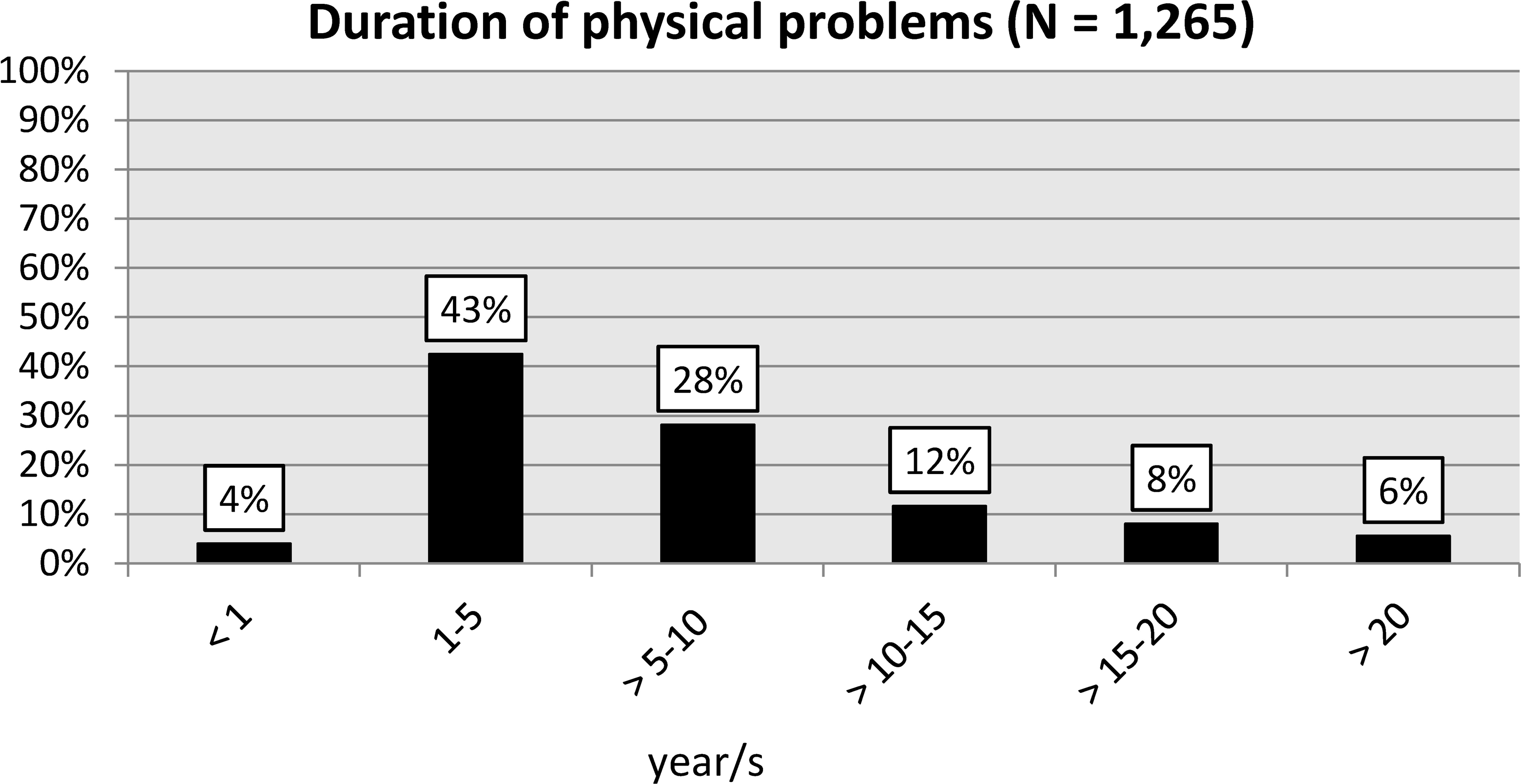
Duration of physical problems.
The duration of physical problems varied significantly between the different instrument families, (F(5, 1240) = 4.861, p < .001, η2 = .019; Table 1). The duration of problems of harpists in particular (M = 15.2, SD = 13.3), but also of woodwind players (M = 9.4, SD = 7.92), was much higher compared to the overall average (M = 8.7, SD = 7.39). The duration of problems among string players and brass players was nearer to the overall average. Percussionists said their problems had lasted around 7 years, a shorter duration than for harpists, who had experienced problems for more than twice as long (cf. Table 1).
Duration of physical problems broken down by instrument family.

It was necessary to take into account the relatively low effect size (η 2 = .019), which to some extent could be explained by the high degree of dispersion. As a result, it was only possible to make very limited generalizations about these differences between groups. There were no significant differences within the variables of gender, position in the orchestra, and category of orchestra.
Severity of physical problems
The respondents assessed the severity of their physical problems on a Likert-type scale of 1–10 (1 = not very severe; 10 = extremely severe). For the sake of clarity, the results were collated in the following categories: not very severe (Scale 1–4), quite severe (Scale 5–6) and very severe (Scale 7–10).
Almost half of the orchestral musicians rated their physical problems as not very severe (48%). Around one quarter assessed their pain level as quite severe (28%) or very severe (23%). There was a weak significant correlation between age and severity of pain (r = .227, p <. 01). Older orchestral musicians tended to assess their pain as more severe than their younger colleagues. There were no significant correlations between (a) the variables of gender, instrument family, position in the orchestra, and orchestra category and (b) the severity of pain.
Perceived causes of physical problems
The musicians were asked to assess whether they felt their physical problems were “work-related” or “age-related.” Although it was not always easy to identify different causes, and the terms “age-related” and “work-related” could not be clearly defined, this question provided an impression of what the musicians subjectively felt was the main reason for their physical problems. Most musicians had a view about whether their problems were work-related or age-related. Only a small proportion of musicians (between 2% and 11%) responded with “don’t know.”
Cardiovascular problems were most commonly considered to be age-related. The majority of respondents (59%) thought that their cardiovascular problems were at least partly due to age (“age-related” or “partly age-related”). More than half (56%) believed their musculoskeletal problems were age-related. Problems with hearing, the respiratory system, and the nervous system were thought of as being age-related by more than 40% of the respondents. The majority felt they were not age-related (Figure 7).

Problems perceived as being age-related.
When assessing the problems as age-related, there were significant differences with regard to the variables of age, gender, position in the orchestra, and orchestra category. The differences in age affected four of the five problem areas. Orchestral musicians up to the age of 49 were less likely than those 50 and older to describe their physical problems as age-related (age-related vs. not age-related; Table 2). The strongest correlation with age could be seen in the cardiovascular system (Phi = .436), followed by musculoskeletal problems (Phi = .333), nervous system disorders (Phi = .298), and hearing disorders (Phi = .245). However, these results should be interpreted with some caution because of the very low numbers of people in some of the individual cells.
Frequency of problems described as age-related in the various age-groups.

*p < .05; **p < .01; ***p < .001.
The significant differences in the assessment (age-related vs. not age-related) between (a) the variables of gender, position in the orchestra, and category of orchestra and (b) musculoskeletal problems are not discussed in more detail here because of their small effect size (Phi < .17).
Our findings were more clear-cut with regard to the assessment that physical problems were work-related. Almost all orchestral musicians (96%) considered their hearing problems to be work-related or partially work-related. Equally, 9 out of 10 musicians thought their musculoskeletal and nervous system problems were at least partially work-related (Figure 8). Most of the musicians affected believed that their cardiovascular problems (73%) and problems related to the respiratory system (61%) were work-related or partially work-related. However, it should be remembered that these are self-assessments and are not backed up by other evidence.

Problems perceived as being work-related.
The different age-groups revealed significant differences when it came to assessing whether the respiratory system and nervous system disorders were work-related. Orchestral musicians over 50 years of age (60%) were more likely than their younger colleagues (11%) to describe their problems related to the respiratory system as work-related. The χ2 test demonstrated a medium to large effect (χ2 = 5.53, p < .001, Phi = .480). In addition, almost all older orchestral musicians (98%), but also a very large proportion of younger musicians (82%), believed their nervous system problems were work-related (χ2 = 6.07, p < .001, Phi = .263).
There were significant differences with regard to musculoskeletal problems and to the variables gender and instrument family (string players vs. wind instrument players). Female musicians (95%) were slightly more likely to assess their musculoskeletal problems as being work-related than male musicians (88%; χ2 = 7.93, p = .005, Phi = .115). String players (94%) were more likely to describe their musculoskeletal problems as work-related than wind instrument players (86%; χ2 = 11.58, p = .001, Phi = .141).
Psychological problems
In the qualitative preliminary study, job satisfaction and pressure to perform in the orchestra were mentioned and specified as potential psychological problems. Based on the qualitative results, the following aspects of job satisfaction were included in the questionnaire: satisfaction with (a) current position in the orchestra, (b) the atmosphere in the particular section, (c) the atmosphere in the orchestra as a whole, (d) career prospects within the orchestra, (e) the principal conductor, and (f) the musical performance of the orchestra as a whole. These aspects were evaluated on the following scale: 1 = very good to 5 = poor, and we gathered these into three categories: very satisfied (scores 1 and 2), fairly satisfied (3), and not very satisfied (4 and 5: Figure 9).

Percentages showing levels of satisfaction with current orchestra.
Overall, the majority of musicians were happy with their position in the orchestra, which was rated as very good or good by 86% of respondents. More than 60% of musicians were also very happy with the atmosphere in their section (69%), the orchestra’s musical performance (61%) and the atmosphere in the orchestra as a whole (60%). By comparison, between 10% and 13% of musicians rated these aspects as inadequate or poor.
The questions about how satisfied musicians were with their career prospects within the orchestra and with the principal conductor produced a range of responses. More than half of orchestral musicians (56%) said they were very happy with their career prospects, while the others were “fairly” (22%) or “not very satisfied” (23%).
The principal conductor was the most polarizing factor: half of the musicians (50%) said they were very satisfied in this respect, while 22% responded said they were “fairly satisfied,” and 28% were “not very satisfied.” There were no statistically significant correlations between (a) satisfaction/dissatisfaction with the principal conductor and (b) the variables of age, gender, position in the orchestra, instrument family, or category of orchestra.
On the other hand, there were statistically significant differences between some aspects of satisfaction and the variables of age, gender, position in the orchestra, instrument family, and category of orchestra. The main difference related to the musicians’ position in the orchestra. A total of 74% of soloists, but only 38% of non-soloists, said they were very happy with their position (χ2 = 170.43, p < .001, Cramer’s V = .326). A similar picture emerged with regard to career prospects, which were viewed more positively by soloists than non-soloists, though the effect size was much smaller (χ2 = 27.78, p < .001, Cramer’s V = .135). Around 63% of soloists and 52% of non-soloists rated their career perspectives in the orchestra as very good or good.
The trend was similar concerning musicians’ levels of satisfaction with the atmosphere in their orchestra section. Overall, more soloists (77%) than non-soloists (66%) rated the atmosphere in their orchestra section as positive (χ2 = 34.14, p < .001, Cramer’s V = .147). By contrast, there was no significant difference in assessments of the atmosphere in the orchestra as a whole and no significant effects of gender, instrument family, position in the orchestra, and orchestra category.
When it came to job satisfaction, there were significant differences between age-groups and orchestra categories. Older members of the orchestra (50 and above) tended to be more satisfied with the orchestra’s musical performance than their younger colleagues (below 50; χ2 = 65.37, p < .001, Cramer’s V = .162). Musicians in the 50+ age-group were more likely to rate their satisfaction with the performance of the orchestra as very good (17%) or good (53%) compared to younger musicians (very good = 10% or good = 46%).
With regard to the differences between orchestra categories, members of Category A orchestras tended to express the highest levels of satisfaction (69% gave a rating of good or very good). In comparison, the percentage of top ratings in orchestra categories B (52%), C (37%), and D (42%) was lower (χ2 = 113.11, p < .001, Cramer’s V = .166). There was no clear evidence that levels of satisfaction had a positive correlation with an orchestra’s performance and size, as members of D-class orchestras expressed higher levels of satisfaction than those in C-class orchestras.
Pressure to perform in the orchestra
The musicians’ responses showed that the pressure they felt to perform had increased since joining their current orchestra. Around half of orchestral musicians (49%) stated that pressure to perform had increased. A further 36% had not noticed any change in this respect, and the remaining 15% thought there was less pressure at the time of the survey. There were significant differences between age-groups in their assessment of whether pressure to perform had increased (χ2 = 263.31, p < .001, Cramer’s V = .231). As the musicians grew older, they tended to feel under growing pressure to perform (Figure 10), with the percentage increasing from 20% in the youngest age-group to 70% in the oldest. The fact that the under-35 age-group in particular felt no increase in pressure to perform is probably linked to the short time they had been members of an orchestra at the time. Perceived pressure to perform was slightly higher in the under-30 age-group than in the 30–34 group. This may be due to the fact that musicians under the age of 30 are still in their stressful probation period, while the 30–34 age-group has generally completed this.

Change in pressure to perform since joining the orchestra by age-group.
The musicians’ perception that pressure to perform increases over time has a number of reasons, such as growing artistic demands, difficult relationships with the conductor, or an ever-increasing workload (see Gembris & Heye, 2012, p. 113).
Health behaviors
The health behaviors of orchestral musicians were studied with the help of 10 items relating to the avoidance of behaviors that damage health (prevention) and the exercise of behaviors that promote health (Table 3 for list of items). The response format was a four-point Likert-type scale (0 = definitely not the case, 1 = generally not the case, 2 = generally the case, and 3 = definitely the case).
Characteristic values of items relating to health behaviors.

These 10 items were gathered together under the heading “health behaviors” (N = 2,316).
Internal consistency was α = .68. The corrected selectivities ranged from rIT = .20 to rIT = .60. The characteristic values of the individual items are shown in Table 3.
All the items were used to calculate a score, as eliminating certain items would not clearly improve reliability, and such an elimination would compromise the content of this construct. In order to calculate the health behaviors variable, a factor score with standard normal distribution was calculated using univariate factor analysis.
Impact on health behaviors
There was a significant positive correlation between age and health behaviors, but it was so small that it can be ignored, r = .041, p < .05.
However, gender had a significant effect, t(2283) = 13.27, p < .001, δ = 0.58. Female musicians were significantly more health conscious in their behavior than their male colleagues (Table 4). Cohen’s δ showed an average effect.
Descriptive statistics: heath behaviors by gender.

There were significant differences in mean value between instrument families, F(5, 2281) = 6.416, p < .001, η 2 = 0.14. The post-hoc test showed that violinists and woodwind players were significantly more likely to exhibit health conscious behaviors than musicians in other instrument families (low strings, brass, percussion) (Table 5). Harpists were most health conscious in their behavior and percussionists were the least in this respect (but there were no significant group differences). However, the overall effect size was very small. This effect was also not significant when gender was controlled for, F(1, 2257) = .322, p > .05, η 2 = 0,00.
Descriptive statistics: health behaviors by instrument family.

Soloists exhibited significantly more health conscious behavior than non-soloists, t(1472) = −0.31, p < .01, δ = 0.181. However, the effect size was relatively small.
Correlations between the severity of physical problems and different health behaviors
The musicians assessed the severity of their physical problems on a Likert-type scale of 1 to 10 in response to the question “How severe are your problems overall”? (1 = not very severe; 10 = extremely severe). Bivariate (Pearson) correlations were calculated between the severity of health problems and different health behaviors, so that we could find out whether there was a correlation between the severity of the problems and the preventative actions taken. No significant correlation was identified between the severity of problems and particular health behaviors, r = .041, p >.05. However, there was a weak, significant correlation with age, r = .226, p < .001. In general, people tend to suffer more physical problems as they grow older.
There was no significant difference between male and female orchestral musicians with regard to the severity of their problems, t(1358) = 0.046, p > .05.
There were also no significant differences between the different instrument families in terms of the severity of health problems, F(5, 1354) = 0.759, p > .05.
There were also no significant differences in mean value with regard to the severity of physical problems among soloists and non-soloists, t(882) = −1.576, p > .05.
However, the degree of stage fright (1 = not at all to 10 = a great deal) had a significant positive correlation with the severity of problems: the more stage fright experienced by a musician, the more severe their health problems, r = .269, p < .001. But this correlation was still relatively weak. No significant correlation was noted between stage fright and health behaviors, r = −.009, p > .05.
It is interesting to note that there was practically no correlation between health behaviors and the severity of physical problems that affected the musicians’ ability to play, rpbis = .074, p < .001. This means that musicians who had problems that affected their playing seemed not to pay more or less attention to their health than musicians who had no problems.
In terms of how they deal with mental and physical problems, the orchestral musicians were asked what gave them the strength and energy to carry on when they were under particular stress at work. The responses showed that most of the musicians found that music was their greatest resource for combating stress at work. Two thirds of the respondents (67%) said that music gave them a great deal of strength and energy. In second place came their partners (66%), followed by family (57%), hobbies (48%), friends (44%), and sport/fitness (41%). In contrast, interventions such as physical techniques, psychotherapy, and medical treatments and medication were considered to be less helpful (Figure 11).

Importance of different ways of managing professional stress.
Discussion
These results are based on data collected from a full survey of all 133 Kulturorchester in Germany, involving almost 10,000 orchestral musicians. Of the 9,922 musicians who were sent questionnaires, 2,536 (26%) took part in the survey. This is the most comprehensive study of professional orchestral musicians to date. According to the official figures and statistics of the German Orchestra Union (DOV), its parameters such as age, gender, and nationality reflected the actual composition of German Kulturorchester at the time of the survey, so we can assume the sample was representative, at least with regard to these variables.
Our findings show that at the time of the survey, half of all orchestral musicians had physical problems that affected their ability to play.
In principle, this confirms the findings of other studies that have suggested large numbers of professional musicians suffer from physical problems that affect their playing (for a literature review, see Spahn & Möller, 2011). However, our results clearly deviate from previous studies with regard to prevalence. In their review of international studies, Ackermann, Driscoll, and Kenny (2012) found that 70–80% of musicians typically suffer from work-related disorders. In their own survey of 377 orchestral musicians in Australia, they had found that 84% of their sample had experienced pain or injuries interfering with playing at some time during their career, but only “Fifty percent of musicians reported having such pain or injury at the time of the survey” (p. 183). Steinmetz (2015a, 2015b) noted in her literature review that 89% of musicians claimed to suffer from PRMDs. The oft-cited study by Fishbein et al. (1988) examined a similar number of test subjects (2,212) and reported that 82% of musicians had a general medical problem and 76% a medical problem that affected their musical performance. The discrepancy with our results, which show that “only” 55% of respondents had problems that affected their performance, is probably due to the fact that we explicitly asked about physical problems that were currently affecting their ability to play at the time of the study. Other studies, however, have included general problems, including psychological issues such as stage fright (stage fright was dealt with separately in our study).
Our results show that the prevalence of physical problems that affect playing is clearly linked to aging, so it provides more detail on previous findings. The frequency of physical problems increased steadily, from 28% in the under-30 age-group to almost 70% among the over 55s. In relative terms, the sharpest increase in physical problems occurred between the ages of 40 and 50. To some extent, our findings on age-related problems that affect playing correspond with those of Berque et al. (2016), who found that the emergence of PRMDs among professional orchestral musicians is age-related in that musicians with PRMDs were on average 5 years older than musicians without problems (M = 49.6, SD = 8.83 vs. M = 45.0, SD = 10.83; p. 81). The high standard deviation suggests that a considerable number of younger musicians are afflicted by PRMDs, but also that there are many older musicians who have no problems. However, the sample of N = 101 is too small to be able to paint a more accurate picture. Nevertheless, our results and those of Berque et al. (2016) contradict other studies that suggest being a professional musician has a protective effect in the long run, and that therefore musicians who have been playing for fewer years are more likely to suffer from PRMDs than musicians who have been playing for longer (see, e.g., Davies & Mangion, 2002).
In general, it is hardly surprising that the frequency of physical problems and disorders increases with age. But it is surprising that almost 30% of the youngest group of musicians in our study already had physical problems that affected their playing. And by the time they reached their 50th birthday, at least two thirds of musicians felt their musical performance was affected by physical problems. This should prompt orchestras to pay more attention to the health of their members in general, and particularly their older musicians, if they want to maintain the musical standards of the orchestra. Our study shows that performance decreases parallel with age-related increases in physical problems (Gembris & Heye, 2014). The musicians who took part in our survey also felt that musical capabilities are generally highest before the age of 40 and then decline sharply. They also believed their own musical performance had gradually declined after the age of 30 (cf. Gembris & Heye, 2014) and were finding it increasingly difficult to meet their own expectations in this respect as they grew older. Although declining performance as a result of aging, such as the slowdown of cognitive and sensorimotor processing, is confounded with health-related declines in performance due to physical problems, making them difficult to distinguish, it can be assumed that avoiding physical problems by taking appropriate preventative action would help musicians to maintain their performance for a longer period.
The problems that were most frequently mentioned (83%) were musculoskeletal disorders. This finding corresponds to the generally very strong prevalence of musculoskeletal disorders that has been noted in other studies (e.g., Andersen, Roessler, & Eichberg, 2013; Ackermann et al., 2012; Berque et al., 2016; Kenny & Ackermann, 2013; Kim, Kim, Min, Cho, and Choi, 2012; Leaver et al., 2011; Paarup et al., 2011; Papandreou & Vervainioti, 2010; Sandell, Frykman, Chesky, & Fjellman-Wiklund, 2009; Steinmetz, 2015a, 2015b; Wallace et al., 2016). Blum (1995) noted a very similar percentage of respondents with musculoskeletal problems (86%) in a study involving a large sample of string players (N = 1,432) in German orchestras.
Other studies have shown a higher prevalence of physical problems among women (Berque et al., 2016; Kenny & Ackermann, 2013; Leaver et al., 2011; Steinmetz, 2015a; Paarup et al., 2011; Wallace et al., 2016). Our results confirm these findings and shed more light on them.
Paarup et al. (2011) showed that 97% of female orchestral musicians and 83% of male musicians had at some point experienced musculoskeletal pain. We identified similar gender-related differences (91% of women and 78% of men). We also noted that physical problems that affect playing tend to start at an earlier age (late 30s) among women than men. Men catch up a few years later, once they enter their 40s. Some of the standard deviations in the two groups were high, suggesting there are more pronounced differences within the groups.
We compared string players (90%) to players of other instruments and found they have an above-average likelihood of suffering from physical problems. This reflects the findings of other studies, which also show that violinists are more susceptible to developing physical problems (e.g., Kenny & Ackermann, 2013; Paarup et al., 2011; Steinmetz, Scheffer, Esmer, Delan, & Peroz, 2015). We were unable to attribute the increased prevalence of PRMDs among string players compared to players of other instruments to the slightly higher proportion of women (53%). Steinmetz et al. (2015) believe violinists are more likely to suffer physical problems because it is usual to begin playing this instrument much earlier than other instruments, traditional orchestra repertoires require them to play for longer than other instruments, and they have to hold an asymmetrical playing position for a sustained period. It seems plausible that this combination of factors could lead to increased susceptibility.
However, this does not explain the increased prevalence of musculoskeletal problems among harpists (92%) compared to players of other instruments (n = 40). Apart from one player, all the harpists in our study were women. Harpists generally take up their instrument at a later stage than violinists, and they only play rarely in the orchestra, so there must be other and/or additional factors involved.
A number of potential treatments for relieving pain, such as physiotherapy and acupuncture, have been discussed as ways of countering the effects of musculoskeletal problems on professional musicians (Chan & Ackerman, 2014; Chan et al., 2013; Molsberger & Molsberger, 2012). In our study, only 18% of musicians stated that their orchestras offered preventative treatments such as physiotherapy. When they were available, they tended to be one-off, irregular, or only offered by larger orchestras, so they do not meet the needs of musicians in this respect. On the other hand, only 27% of musicians said they would take part in a health program in their free time if such a program existed. Perhaps their lack of enthusiasm for health programs is because they are only suffering low levels of pain. A recent study by Chimenti et al. (2013) seems to confirm this suspicion, finding that musicians tend to understate the severity of symptoms that affect their playing and make out they are less serious than is actually the case. Another strategy is to ignore pain (Andersen et al., 2013). In this respect, Altenmüller (2013) argued that the instruments used to measure pain experienced by orchestral musicians are too sensitive and that the only responses often come from musicians with problems, leading to a whole profession becoming pathologized (p. 67).
There has been little systematic research on how health risks vary between different categories of musicians. Voltmer et al. (2012) examined the physical and mental health of professional musicians using a standard measurement instrument (a short form of the SF-36 health survey (SF-12) for the evaluation of physical and mental health; Voltmer et al., 2012, p. 10) and compared the results with the health status of doctors, aircraft mechanics, and a reference group (for more details on this, see Gembris & Heye, 2012, pp. 142–144). Previous studies had revealed that 50–70% of professional musicians suffered from physical problems, but the study carried out by Voltmer et al. (2012) showed that musicians enjoyed significantly better physical health than the other groups surveyed. Their mental health was significantly worse than the reference group but similar to that of doctors and aircraft mechanics. Age played a significant role in health status, with the health of all groups worsening as they grew older. However, it is interesting to note that musicians in every age-group experienced less deterioration in their general health than aircraft mechanics and the general population.
The authors questioned whether this surprising result, compared to previous studies, actually reflected better physical health on the part of orchestral musicians or whether musicians simply have a different perception of health (p. 12). It may be that musicians consider playing-related symptoms to be “normal” or that they view the musculoskeletal problems that are so frequently reported as somehow separate from their general state of health.
The health report Gesundheit in Deutschland [Health in Germany, translated by the authors], published by the Robert Koch Institut (2015), shows that musculoskeletal problems are behind the majority of sick days and the second-highest reason for taking early retirement on health grounds (p. 69). Around one fifth of sick days are due to musculoskeletal problems (Rebscher, 2016, p. 18). The number of absences ranges from 31 days a year in jobs involving supply and disposal and 4 days a year among university lecturers and researchers (Badura, Ducki, Schröder, Klose, & Meyer, 2015). However, the statistics do not include professions in the artistic/cultural field that could be used for the purposes of comparison. The authors of the health report Gesundheit in Deutschland (Robert Koch Institut, 2015) also noted that there is a lack of evidence-based data on the prevention, diagnosis, and rehabilitation of musculoskeletal disorders (p. 76).
Our study was not able to measure hearing disorders, but these were included on the basis of diagnosed hearing problems reported by the musicians surveyed. Therefore, our results cannot be directly compared with studies that measure other parameters such as sound pressure levels, hearing and auditory thresholds and that draw conclusions on hearing problems (e.g., Kähäri et al., 2001a, 2001b; Rodrigues et al., 2014; Russo et al., 2013). A portion of 38% of the orchestral musicians in our study said they had been medically diagnosed with a hearing problem at some point in the past. While Blum noted that 24% of musicians had hearing problems, in a comparative study of British and German orchestral musicians, Harper (2002, p. 91) found that 38% of British and 37% of German musicians had been diagnosed with hearing problems, which corresponds quite closely to our findings. Hasson et al. (2009) also found that 40–57% of musicians suffered from hearing loss. The likelihood of suffering from a hearing disorder (such as hearing loss or tinnitus) increases with age. However, even objective measurements are unable to show whether these are age-related changes or due to work-related stress that intensifies with age.
Health problems can also be caused by psychological stress. Increasing pressure to perform in the orchestra may play a major role in this respect. Older orchestral musicians feel this pressure to perform more acutely than their younger colleagues, and the respondents generally felt this trend was due to increased artistic demands. Expanding workloads and difficulties with the conductor also play a role. The correlation between psychological factors such as stress and job satisfaction has been empirically proven (cf. Abeles & Hafeli, 2014; Felger, 2014; Holst, Paarup, & Baelum, 2012; Jäncke, 2011). It has also been shown that professional stress is linked to physical symptoms (Kaufman-Cohen & Ratzon, 2011).
Preventative health behaviors correlated with instrument family, position in the orchestra, and age. Harpists, woodwind players, and violinists tended to be more health conscious than other musicians in the orchestra. Soloists exhibited more health conscious behaviors than non-soloists and older musicians more than their younger colleagues.
It is interesting to note that when asked how they coped with stress, most musicians mentioned music ahead of their partners, family, children, and hobbies. This is surprising because playing music professionally is often linked to stress and can be detrimental to health, whereas music is also a source of recreation. However, a number of studies have shown that music is an important source of well-being and health for nonprofessional players and involves fewer risk factors than those faced by professional musicians (Brodsky, 2006; Gembris, 2012). The polyvalence of music is clearly connected to the way it is used. It would be interesting to examine how professional orchestral musicians use music as a way of dealing with stress. Many orchestral musicians find it stressful that they are typically trained to be soloists but then are subordinated to the conductor with little or no scope for developing their own artistic vision. At least to some extent, it is possible to compensate for this sense of musical heteronomy by pursuing their own musical projects that allow them to develop their artistic vision outside the orchestra, and this can contribute to their happiness and psychosocial well-being. The same applies to musicians who have retired from the orchestra (Dick, 2017).
With regard to staying healthy, it is interesting to note that the musicians surveyed frequently said that appreciation from their colleagues (40% = “very important,” 50% = “quite important”) and recognition from the principal conductor (27% = “very important,” 47% = “quite important”) were an important resource for coping with professional stress. It is up to the orchestras to create a culture of mutual appreciation and recognition that, at the end of the day, benefits everyone. Generally, there is a growing interest in research on health promotion for musicians (Norton, 2016). Norton, Ginsborg, Greasley, and McEwan (2015a, 2015b) claim that health and well-being issues should be included in music education programs to prevent and mitigate performing-related health problems.
Limitations of the study
Our study was not primarily designed to look at medical issues affecting musicians, but its main focus was the topic of growing older in an orchestra. It only addressed certain aspects of physical and mental health problems in a general way in so far as they are linked to aging and the effect that this has on the work of orchestral musicians. We devised our own questions to examine musculoskeletal and other physical problems, but in principle it would have also been useful to make use of standardized instruments such as the Musculoskeletal Pain Intensity and Inference Questionnaire for Musicians (MPIIQM) produced by Berque et al. (2016). This would also have made it possible to compare the results of different studies. But it was difficult to include existing measuring instruments in our study because this would have resulted in our already detailed questionnaire being even longer. The same applies to the measurement of hearing problems, degrees of stage fright, and other psychological issues. Apart from this, the MPIIQM was actually published after our survey was carried out.
This study is a cross-sectional survey, so it does not provide information on individual progression. It is possible that the age-related differences in physical problems, health behaviors, and other variables are confounded with differences between generations, something that cannot be assessed here. Some of the statistical correlations are relatively weak, which could be put down to a relatively high interindividual variance and hence point to corresponding interindividual differences. Longitudinal studies are needed in order to find the answers to these questions. When interpreting our data and findings, it should also be borne in mind that these are self-assessments, so they reflect the subjective perceptions of professional orchestral musicians. Their perceptions of things like musical performance and physical problems may deviate from the perceptions of others and objective findings. On the other hand, these self-assessments show the image and concept that musicians have of themselves, which forms part of the subjective identity.
The return rate of 26% was below our expectations. We expected it to be higher because appropriate numbers of questionnaires were sent to every orchestra via the DOV, and the DOV specifically recommended that musicians should complete them. However, we discovered that some of the orchestras were away on tour during the time of the survey, so their members were unable to take part. We were also told that some of the orchestras receive frequent requests to take part in surveys, so some musicians are suffering from questionnaire fatigue. It may also be that there are musicians who are not interested in dealing with the topic of growing older in a symphony orchestra or that non-German speakers would have found it hard to complete the questionnaire.
Outlook and future research
Mertens (2016) has identified two key trends in Germany’s orchestras. A fundamental overhaul has led to some orchestras being merged or even dissolved. Since carrying out our survey, the number of orchestras in Germany has fallen from 133 to 130 (2016) and will drop to 128 in 2017. This has had an impact on musicians’ contracted positions, which have fallen from 12,159 in 1992 to 9,816 today, a decline of 19% (p. 6), yet the number of music school graduates continues to rise (Gembris & Menze, 2017, in print).
Competition in the job market and the demands made on orchestral musicians will only intensify in the years to come. Artistic demands are increasing, along with pressure to find ways of countering dwindling audience figures. To this end, orchestras are working to increase musical appreciation (see Mertens, 2016), for example through school concerts, workshops in mainstream schools, and involvement in music schools (e.g., student, youth, and regional youth orchestras, and church music). So orchestral musicians are now finding themselves acting as instrument teachers, mentors, and soloists in nonprofessional orchestras. Their work is expanding and dealing with these changes, while maintaining their performance and health means that it is more important than ever for them to be provided with and to use preventative health programs.
Equally, research on the links between health and physical and mental problems on the one hand and growing older as an orchestral musician on the other is gaining in importance against the backdrop of our aging society and longer working lives. More studies are also required on the protective effect of musical activities. Research into these correlations should not be limited to orchestral musicians, but should also include freelance musicians and musicians in other musical genres such as pop and jazz. This opens up many possibilities for further research that has a very practical relevance.
Footnotes
Contributorship
HG and AH researched literature and conceived the study (including study design, participant recruitment and data collection). AH and HG did the first data analysis. AS was involved in further data analysis. All authors wrote the first draft of the manuscript, reviewed and edited the manuscript. HG and AH approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This research was conducted in accordance with the “Guidelines for Safeguarding Good Research Practice”, published by the Deutsche Forschungsgemeinschaft (DFG).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research on which this article is based on was funded by the Deutsche Orchestervereinigung (DOV).
Notes
Peer review
Eckart Altenmüller, University of Music, Drama, and Media Hannover, Institute of Music Physiology and Musicians Medicine. Jane Ginsborg, Royal Northern College of Music.
Appendix A
Standard instruments within the instrument families, grouped according to gender and age.

| Instrument familiesa | Number and percentage of total sampleb | Femalec | Male | Age | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Contracted instruments | n | % | n | % | n | % | M | SD | Min. | Max. | |
| High strings | Violin |
13 | 0.5 | 6 | 54.5 | 5 | 45.5 | 46.82 | 10.62 | 31 | 63 |
| 1. Violin | 359 | 14.2 | 189 | 54.0 | 161 | 46.0 | 46.64 | 9.50 | 23 | 69 | |
| 2. Violin | 342 | 13.5 | 200 | 58.8 | 140 | 41.2 | 46.70 | 9.50 | 24 | 64 | |
| Viola | 276 | 10.9 | 120 | 44.1 | 152 | 55.9 | 47.27 | 9.12 | 25 | 64 | |
| Total | 990 | 39.2 | 515 | 52.9 | 458 | 47.1 | 46.84 | 9.40 | 23 | 69 | |
| Low strings | Violoncello | 213 | 8.4 | 73 | 34.6 | 138 | 65.4 | 46.17 | 9.41 | 23 | 65 |
| Double bass | 156 | 6.2 | 18 | 11.5 | 138 | 88.5 | 46.21 | 9.41 | 26 | 64 | |
| Total | 369 | 14.6 | 91 | 24.8 | 276 | 75.2 | 46.19 | 9.40 | 23 | 65 | |
| Woodwind | Clarinet | 136 | 5.4 | 26 | 19.4 | 108 | 80.6 | 45.69 | 8.97 | 24 | 63 |
| Oboe/Cor Anglais | 124 | 4.9 | 48 | 39.3 | 74 | 60.7 | 46.39 | 8.94 | 24 | 63 | |
| Bassoon | 119 | 4.7 | 30 | 25.4 | 88 | 74.6 | 44.13 | 9.43 | 22 | 63 | |
| Flute/Piccolo | 152 | 6.0 | 92 | 61.3 | 58 | 38.7 | 46.58 | 9.41 | 23 | 65 | |
| Total | 531 | 21.0 | 196 | 37.4 | 328 | 62.6 | 45.75 | 9.22 | 22 | 65 | |
| Brass | Trumpet | 126 | 5.0 | 4 | 3.2 | 121 | 96.8 | 45.13 | 9.71 | 22 | 63 |
| Trombone | 117 | 4.6 | 3 | 2.6 | 113 | 97.4 | 43.86 | 9.47 | 20 | 63 | |
| French horn | 193 | 7.6 | 39 | 20.3 | 153 | 79.7 | 43.31 | 10.08 | 21 | 62 | |
| Tuba | 26 | 1.0 | 0 | 0.0 | 26 | 100.0 | 40.58 | 7.89 | 25 | 54 | |
| Total | 462 | 18.3 | 46 | 10.0 | 413 | 90.0 | 43.79 | 9.74 | 20 | 63 | |
| Percussion | Kettledrum/drum | 113 | 4.5 | 1 | 0.9 | 111 | 99.1 | 45.20 | 9.81 | 23 | 64 |
| Plucked strings | Harp | 41 | 1.6 | 40 | 97.6 | 1 | 2.4 | 43.83 | 10.24 | 27 | 60 |
a N = 2,525 (missing = 11). The “Other Instrument” category is not included (n = 19; 0.8%).
b N = 2,506.
cBecause of the large number of missing in the gender-specific analysis, the number of female and male musicians within the instrument groups may differ from the total figure.
dA total of 13 orchestral musicians failed to state their position (first or second violin), so it was not possible to allocate them to one of the two categories.