
Abstract
Introduction
Up to now, there were few studies on extreme lateral interbody fusion (XLIF) surgery for lumbar spondylodiscitis. This study was aimed to evaluate clinical effectiveness and provide more information for XLIF in the treatment of lumbar spondylodiscitis.
Methods
We retrospectively collected cases of XLIF for the treatment of lumbar spondylodiscitis from September 2017 to February 2020. There were 8 cases of non-specific infection of lumbar spine, 4 cases of lumbar tuberculosis, and 1 case of lumbar brucellosis. Basic information, antibiotic application, and inflammatory index were collected before and after surgery. Clinical effectiveness was evaluated at baseline and in 3, 6, and 12 months after the surgery with visual analog scale (VAS) and Oswestry disability index (ODI). The comparison of the indicators before and after the operation was performed by repeated measures analysis of variance.
Results
The average intraoperative blood loss and operation time was 70mL and 99.23 min, respectively. The study consisted of 13 cases with single segment operation. The average follow-up time was 16.54 months. No sign of recurrence of spondylodiscitis occurred at last follow-up. Postoperative VAS and ODI were significantly decreased after the operation. No major blood vessels, nerves, or organ damage occurred during the perioperative period.
Conclusion
XLIF has shown good clinical effectiveness in the treatment of lumbar spondylodiscitis with advantages of less bleeding and less tissue damage in the present study. More multi-center prospective comparative studies are needed to further verify the clinical effectiveness of this procedure in lumbar spondylodiscitis.
Introduction
Spondylodiscitis was a type of disease in which pathogenic bacteria damaged the lumbar intervertebral disc or vertebral body, leading to inflammation, abscess formation, spinal deformity, and even nerve damage. Spondylodiscitis was roughly classified into specific infections and non-specific infections depending on the pathogen. Lumbar spinal tuberculosis and brucellosis were the most common specific infections.1,2 Non-specific infections were mostly bacterial infections, especially the genus staphylococcus, which can be caused by local spreading or bloody dissemination. 3 Thoracic and lumbar vertebrae infections were the most common in spinal infections. The main clinical manifestations of lumbar spondylodiscitis were severe low back pain and fever. When nerve compression occurred, the clinical manifestations were accompanied by pain, numbness, or weakness of the lower limbs or even excretory dysfunction. 4
Conservative treatment can be used in patients with mild spondylodiscitis. Previous studies also confirmed intravenous antibiotics and subsequent oral antibiotics for the treatment of mild spinal infections. 5 However, surgical treatment was needed for abscess formation, nerve compression, spinal instability, or even deformity when conservative treatment was ineffective. Operations included anterior, posterior, and combined anterior and posterior approaches. The purpose of the operation was to completely remove the lesions and restore local stability. In the past few decades, the traditional open anterior lateral lumbar spine surgery could completely remove the lumbar intervertebral and paravertebral lesions and restore local stability with lateral bone graft fusion.6-8 However, open anterior approach had some disadvantages, such as wide exposure area, large trauma, and high risk of vascular and nerve injury, which had always been a concern of scholars.9,10 Posterior lumbar debridement for the treatment of spondylodiscitis avoided complications of the anterior approach, but the effect of clearing up the anterior lateral abscess was poor. In addition, the posterior approach damaged the spinal canal structure, which had the potential risk of central infection. 11 In 2006, Ozgur B 12 proposed extreme lateral interbody fusion (XLIF), which was popularized by spine surgeons and quickly promoted. XLIF was approached to intervertebral disc and lateral vertebral body through retroperitoneal space and psoas major muscle. XLIF completed the discectomy and interbody fusion in a minimally invasive channel and showed good clinical effect in treatment of lumbar degenerative disease.13,14 However, there were few studies on XLIF surgery for lumbar spondylodiscitis.15-19 Moreover, there was a lack of evaluation on the clinical effect of this application. This study retrospectively collected our center’s application of XLIF in the treatment of lumbar spondylodiscitis to evaluate clinical effectiveness and provide more information for XLIF in the treatment of lumbar spondylodiscitis.
Materials and methods
This was a retrospective case series study. This study was approved by the ethics committee of the Third Hospital of Hebei Medical University (2021-009-1). All patients' data collection was informed in advance. The inclusion criteria are as follows: lumbar discitis or vertebral osteomyelitis with clinical manifestations of stubborn low back pain or lower limb pain and conservative treatment is ineffective; abscess formation; nerve compression; and deformity aggravation. The exclusion criteria are as follows: (1) XLIF for treatment of lumbar degenerative diseases; (2) spinal nerve compression and intracanal epidural abscess which required posterior decompression surgery; (3) incomplete follow-up data; and (4) the follow-up time is less than 12 months. We retrospectively collected cases of XLIF for the treatment of lumbar spondylodiscitis from September 2017 to February 2020. Due to the small sample size of such cases, we included all cases according to the inclusion and exclusion criteria without calculating sample size. There were 8 cases of non-specific infection of lumbar spine, 4 cases of lumbar tuberculosis, and 1 case of lumbar brucellosis.
Surgical procedure (Figure 1): The patient was in right lateral decubitus position with general anesthesia and intraoperative neurophysiological monitoring. During the operation, the c-arm lateral position fluoroscopy was used to locate the center point of the diseased intervertebral space. The incision was located at the center of the diseased intervertebral space, and the length was about 3 cm. We bluntly separated the muscle layer to the retroperitoneal space. The surgeon touched the lateral side of the intervertebral disc and inserted the guide needle. Lateral fluoroscopy confirmed that the needle was located in the one-third of the intervertebral disc. The dilatation tube was inserted step-by-step followed by working channel. We expanded the channel, fully exposed the vertebral body and the lateral side of the intervertebral disc, cut the annulus fibrous, and completely removed the necrotic tissue of the intervertebral space and the ipsilateral psoas abscess. Then, we opened the contralateral annulus fibrous and treated the contralateral psoas abscess with a curette and an aspirator. The diseased tissue was taken for pathological examination and bacterial culture. After the debridement was satisfied, they were soaked with hydrogen peroxide and benzalkonium bromide, respectively, and finally rinsed with a large amount of normal saline. The interbody fusion cage or the autogenous iliac bone mass was selected according to the destruction of the intervertebral space. A suitable polyether ether ketone (PEEK) cage filled with allogeneic bone was implanted into the intervertebral space in patients with simple discitis because the vertebral endplate was relatively intact in these patients. Autologous iliac bone mass was implanted in patients with severe vertebral destruction. Then, we added lateral internal fixation in all patients (Figure 2). After confirming the position of the graft by fluoroscopy and making sufficient hemostasis, one flushing tube and one drainage tube were indwelled and the incision was sutured. Surgical procedure of extreme lateral interbody fusion (XLIF) in the treatment of lumbar spondylodiscitis. (a) The patient was in right lateral decubitus position with general anesthesia. (b and c) We inserted the first dilatation tube and determined the position of the first dilatation tube under X-ray fluoroscopy. (d) Intraoperative neuroelectrophysiological monitoring. (e) We fixed working channel by the free arm. (f) Curettage with a curette. (g) Implantation of intervertebral fusion cage. A typical case was intraoperatively supplemented with lateral fixation. (a and b) Preoperative X-rays in anteroposterior and lateral position. (c and d) Preoperative sagittal T1-weighted and T2-weighted MRI revealed L1/L2 lumbar spondylodiscitis. (e and f) Preoperative coronal and sagittal CT showed destruction of upper and lower endplates of narrow intervertebral space. (g) Location of lateral internal fixation under intraoperative X-ray in anteroposterior position. (h) Coronal CT showed good interbody fusion at 6 months after operation.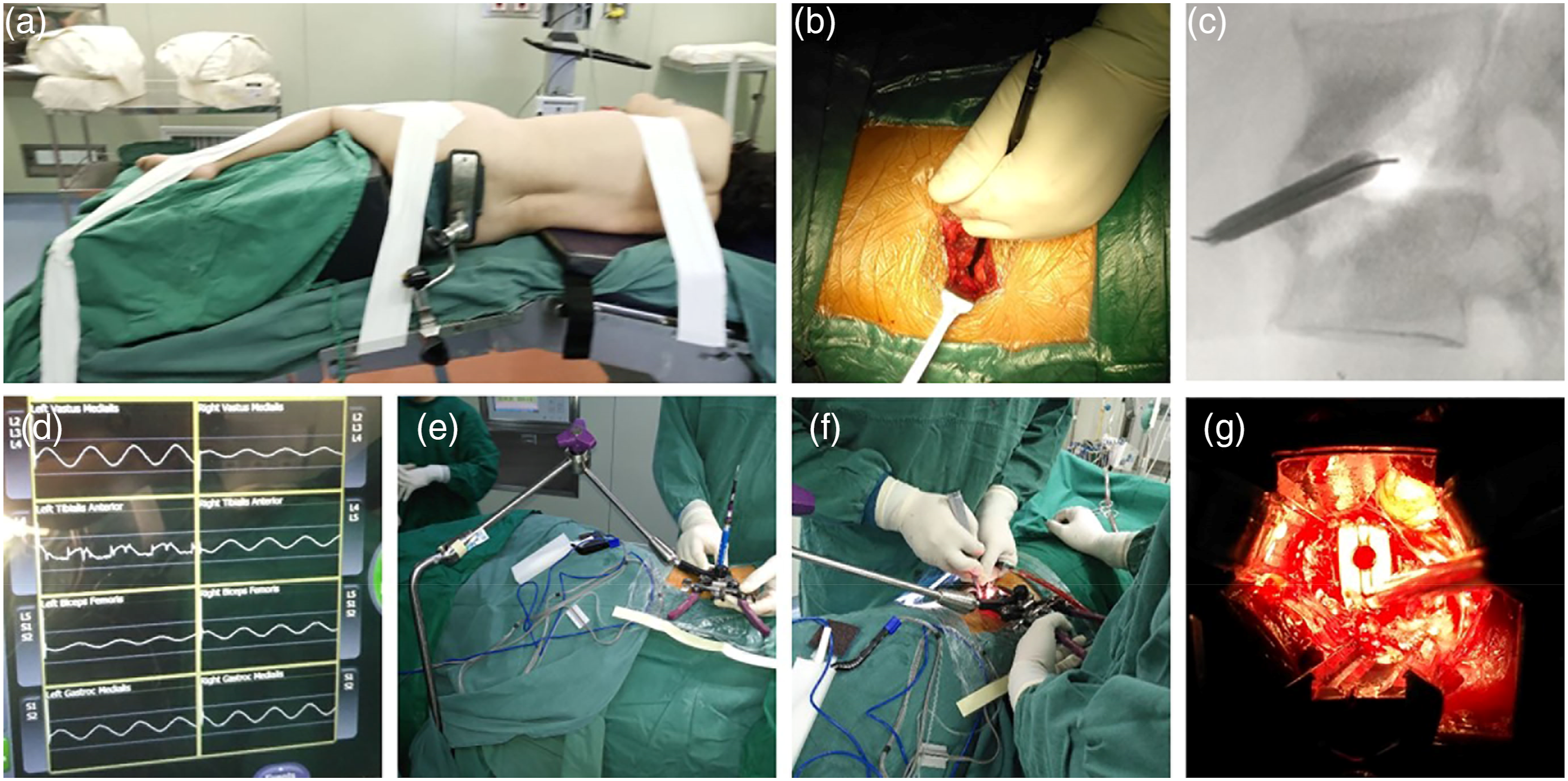

We collected basic information including the patient’s age, gender, intraoperative blood loss, operation time, follow-up time, and so on. The patient’s antibiotic application and inflammatory index were collected before and after surgery. Visual analog scale (VAS) was used to evaluate the lumbar and leg pain of patients before, 3, 6, and 12 months after surgery. VAS practices a horizontal line of 10 cm on the paper. One end of the horizontal line is 0, indicating no pain, the other end is 10, indicating severe pain; the middle part indicates different degrees of pain. Oswestry disability index (ODI) was used to evaluate the improvement of postoperative function including the intensity of pain, self-care, lifting, walking, sitting, standing, interference with sleep, sex life, social life, and tourism. The formation of new bone in operative space and perioperative complications were recorded for patients at each follow-up period. Robust intervertebral fusion was defined as the presence of significant bridging trabecular bone formation between at least two consecutive layers of the spiral computed tomography (CT). The bacterial cultures of blood and intraoperative tissue were obtained from all 13 patients.
We used SPSS v22.0 for statistical analysis. The measurement data conforming to the normal distribution were expressed by the mean ± standard deviation; otherwise, the measurement data were represented by the median (interquartile range). Count data were expressed as a percentage. The comparison of the indicators before and after the operation was performed by repeated measures analysis of variance. p< 0.05 indicated a statistical difference.
Results
Clinical information of surgical patients.


A diagram of postoperative treatment details.
Clinical efficacy and intervertebral fusion rate.
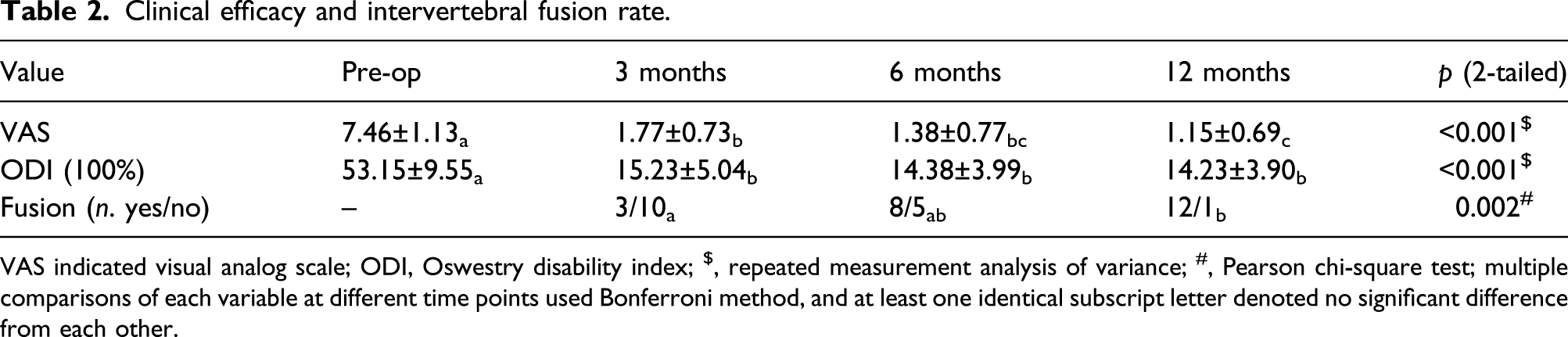
VAS indicated visual analog scale; ODI, Oswestry disability index; $, repeated measurement analysis of variance; #, Pearson chi-square test; multiple comparisons of each variable at different time points used Bonferroni method, and at least one identical subscript letter denoted no significant difference from each other.

Postoperative VAS (a) and ODI (b) were significantly reduced compared with those of preoperation.
In this study, 1 case of numbness and weakness occurred in the left thigh and returned to normal on the fifth day after surgery. No major blood vessels, nerves, or organ damage occurred during the perioperative period.
Discussion
The incidence of lumbar tuberculosis, brucellosis, and lumbar spine non-specific infection was increasing year by year.20,21 For lumbar spondylodiscitis, we first considered conservative treatment with antibiotics. However, surgical treatment should be actively carried out for abscess formation, nerve compression, and deformity aggravation. Traditional open anterolateral surgery and lumbar posterior surgery were effective and reliable for the treatment of lumbar spondylodiscitis.6,11,22 However, open surgery had the disadvantage of large trauma and slow recovery. XLIF was widely used for the treatment of lumbar diseases due to its advantages of minimally invasive, rapid recovery, non-invasive spinal canal, and high interbody fusion rate.13,14 XLIF can fully reveal the lateral of intervertebral disc and vertebral body through the retroperitoneal space under the minimally invasive channel and complete the clearance of the intervertebral space and paravertebral lesions. To date, only few studies have reported that XLIF was used to treat lumbar spondylodiscitis.15-19 However, the current research studies only simply summarized the technology and lacked the evaluation of the clinical effectiveness of this surgical treatment for lumbar spondylodiscitis. This study reviewed the cases of lumbar spondylodiscitis treated by XLIF in our center to evaluate the clinical effectiveness.
Previous studies have reported that the traditional posterior and anterior surgery has a large amount of bleeding and long operation time.8,11 The average bleeding volume of this study was 70 mL and the average operation time was 99.23 min, which reflected the minimally invasive advantage of XLIF compared with traditional surgical methods. Timothy J et al. 16 reported that the intraoperative bleeding volume of 14 patients with intervertebral discitis was less than 100mL. Up to now, all the studies on XLIF in the treatment of lumbar infection were case series studies. Research studies by Blizzard et al., 15 Patel et al., 19 and He et al. 18 were all brief introduction of this clinical application without clinical evaluation. Timothy et al. 16 included 11 cases of non-specific lumbar infection and 3 cases of lumbar tuberculosis, and VAS and ODI improved by 3.0 (95% CI, 1.7–4.4) and 40 (95% CI, 10-52), respectively, at the last follow-up (range 41–93 months) after XLIF. He 17 reported 31 cases of septic spondylodiscitis with preoperative ODI and VAS of 69.7 ± 8.0 and 7.2 ± 1.1. ODI and VAS became 28.9 ± 4.0 and 2.2 ± 1.1 at 2 years postoperatively in the above research. Our study included 8 cases of lumbar non-specific infection, 4 cases of lumbar tuberculosis, and 1 case of lumbar brucellosis. VAS and ODI were significantly reduced in all follow-up periods after operation, which were similar to the results of previous studies on the relief of symptoms and functions. This study reported a case of brucellosis treated by XLIF. Low back pain was relieved after operation and no recurrence of brucellosis was found during follow-up.
Solid interbody fusion was one of the criteria for cure of lumbar spondylodiscitis. There was no agreement on the fusion materials for lumbar interbody fusion in patients with lumbar spondylodiscitis. Timothy 16 used PEEK cage for intervertebral fusion and reported 2 cases of cage collapse. The collapse cases were both with severe vertebral osteomyelitis. This phenomenon of cage collapse may be due to the weak supporting force of vertebral endplate in the presence of severe vertebral osteomyelitis. In this study, intervertebral fusion materials were selected according to the destruction of vertebral endplates. We selected the autogenous iliac bone mass as intervertebral fusion material when the vertebral endplate was severely damaged. When the endplate was relatively intact, the cage filled with the allogeneic bone was selected for interbody fusion. We analyzed that when the upper and lower endplates were relatively intact, the endplates could provide sufficient support force, and the PEEK cage was used for interbody fusion without obvious collapse. All patients underwent lateral internal fixation at the same time to prevent the collapse of intervertebral space. No obvious cage collapse was found in each period of follow-up. This study reported that the interbody fusion of XLIF in the treatment of lumbar spondylodiscitis was 92.3% at 12 months postoperatively, which was equivalent to the fusion rate of XLIF in the treatment of lumbar degenerative diseases. 23
In this study, a case of postoperative transient thigh weakness and numbness occurred, which was considered to be related to the excess pulling the lumbar plexus in the operation. Lumbar plexus injury was the main complication of XLIF. 24 We use intraoperative neurophysiological monitoring to prevent the complication. In addition, we moved the surgical entry point of XLIF to the junction of the anterior one-third of the vertebral body and the operation was farther away from the lumbar plexus. The gap between psoas muscle and large vascular sheath was narrowed and adhered when lumbar spondylodiscitis affected the surrounding tissue. Therefore, the approach of XLIF through psoas major muscle was safe, which reduced the damage of nerves and blood vessels near the gap. There were no serious complications of perioperative neurovascular injury in this study. We recommended that neurophysiological monitoring should be routinely performed during surgery because more adhesion at the infected lesions could increase the risk of lumbar plexus. The surgeon also should separate adhesion carefully and bluntly.
The basic purpose of surgical treatment for lumbar spondylodiscitis was to completely remove infected necrotic lesions. Incomplete debridement often led to recurrence of infection. The reasons for the complete debridement of the lesions in this study were as follows: (1) XLIF was a pure lateral approach, so we could clearly expose lateral intervertebral space and vertebral body. (2) We opened the contralateral annulus fibrous to treat the contralateral psoas abscess after thoroughly debriding the intervertebral space. (3) We used a curette to scrape the infected lesions and further cleaned the lesions with wet gauze. (4) After removing the necrotic tissue, we soaked operative area in hydrogen peroxide and benzalkonium bromide for 5 minutes, respectively, then rinsed it with a large amount of saline. (5) We indwelled an irrigation tube and a drainage tube; the drainage fluid was cultured every 3 days, and the irrigation tube was changed into a drainage tube when the culture was negative for three consecutive times.
Of course, this study had certain limitations. This study was a retrospective study and lacked comparative studies. We need to carry out a comparative research between XLIF and traditional open surgery for lumbar infectious diseases in the future. The number of cases in this study was small because of relatively low incidence. The sample size needs to be further expanded to confirm the effectiveness of XLIF in the treatment of lumbar infection. As far as we know, there was no literature about chemotherapy protocol in the treatment of brucellosis and tuberculosis before and after XLIF. The chemotherapy protocol before and after surgery in this study followed the experience of our center. The selection of chemotherapy protocol before and after XLIF requires further research. According to our understanding, there was no comparative study on different interbody bone graft materials for XLIF in treatment of spondylodiscitis. Whether to choose autologous iliac bone mass or PEEK cage for interbody fusion needs further studies. XLIF had a small amount of bleeding during operation, and a drainage tube was not needed in the treatment of lumbar degenerative diseases with less bleeding. There was a doubt whether a drainage tube was needed for XLIF in the treatment of lumbar spondylodiscitis. If the drainage was retained after operation, there was no literature to support the choice of regular drainage or irrigation drainage. Indwelling an irrigation drainage in the present study was based on removal of pathogens as much as possible. Whether it is meaningful or not, further research studies are needed.
Conclusion
XLIF has shown good clinical effectiveness in the treatment of lumbar spondylodiscitis with the advantages of less bleeding and less tissue damage in the present study. At present, there were few studies on this clinical application. More multi-center prospective comparative studies are needed to further verify the clinical effectiveness of this procedure in lumbar spondylodiscitis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Bureau of Science and Technology of Hebei Province (20377750D). This funding supports the development of XLIF technology.
Ethics approval
The present study was a retrospective study. Ethics approval to conduct this study was obtained from ethics committee of Hebei medical university third affiliated hospital. The ethical code is 2021-009-1.
Informed consent
Written informed consent was obtained from all subjects before the study.