
Abstract
We aim to reveal the clinical features of transluminal broncholiths and to evaluate the efficacy and safety of bronchoscopy for treating transluminal broncholiths. Patients with transluminal broncholiths were enrolled in this retrospective study in Lanzhou University Second Hospital between January 2010 and December 2018. Then age, gender, symptoms, and signs, imaging characteristics, treatment methods, outcomes as well as complications were retrospectively analyzed. Twenty-eight patients with 36 pieces of transluminal broncholiths were diagnosed using chest CT and bronchoscopy, of which two patients underwent broncholiths removal via an elective surgical procedure and six patients were treated with one-time removal of broncholiths by bronchoscopy. Among the six patients who received one-time removal of stones by bronchoscopy, two underwent massive hemorrhage and one suffered from bronchial wall laceration in the process of broncholiths removal, all of the three patients received surgical treatment eventually. No serious complications occurred in the other 20 patients who underwent broncholiths removal via repeated bronchoscopy. Removal of transluminal broncholiths by bronchoscopy are effective and safe with less complications. When it is difficult to remove the transluminal broncholith completely at one time, repeated bronchoscopy could be chosen: First, to remove the portion which causes airway obstruction; and then to remove the remaining part by repeated bronchoscopy during the follow-up period. In case that severe distal lung tissue injury, massive hemoptysis or bronchial wall laceration occurs or the diagnosis of broncholiths is unclear, surgical treatment is required.
Introduction
Broncholithiasis is defined as the presence that calcified lymph node erodes into the lumen of the tracheobronchial tree, forming broncholiths and further causing inflammation and obstruction. 1 The calcified substances are derived from chronic necrotizing granuloma infection including tuberculosis, histoplasmosis and rare actinomycosis, which cause calcification of mediastinal and hilar lymph nodes. 2 Broncholiths are classified into intraluminal, transluminal and extraluminal acc-ording to the anatomy between calculus and bronchial lumen confirmed by chest CT or bron-choscopy. An intraluminal broncholith means that the stone is confined to the bronchia lumen, while an extraluminal broncholith means that the stone is located outside the bronchial lumen and does not penetrate the bronchial wall. A transluminal broncholith is defined as the mixed type with both intraluminal and extraluminal components of stone-like material in the tracheobronchial tree. 3
While chest CT can reveal the presence of lymph node calcifications, it lacks the resolution to identify the transluminal broncholiths. On occasion, a broncholith cannot be identified even by high-resolution CT due to partial erosion of the node into the airway. 4 Bronchoscopy plays a crucial role in the diagnosis of broncholiths via accurately and directly identifying the specific location of the broncholith, the degree of endobronchial obstruction and the anatomy between calculus and bronchial lumen. 5
At present, the treatment methods of broncholithiasis mainly include bronchoscopy and surgical intervention. 2 Intraluminal broncholiths can be removed entirely or in part by biopsy forceps, foreign body forceps or net baskets under bronchoscope, with or without pretreatment of holmium laser lithotripsy. 6 Olson et al. 7 have reported that intraluminal broncholiths can be removed by a rigid bronchoscope or flexible bronchoscope with a 100% success rate. However, it is often difficult to remove a transluminal broncholith completely at one time with no complications such as massive hemorrhage and bronchial wall laceration. 2 We aim to explore the advantages and importance of the staged extraction of transluminal broncholiths via bronchoscopy. In this study, 28 patients with transluminal broncholiths were enrolled retrospectively in Lanzhou University Second Hospital between January 2010 and August 2018 to evaluate clinical presentation, imaging characteristics, treatment methods, outcomes and complications, exploring the efficacy and safety of the staged extraction of transluminal broncholiths via bronchoscopy.
Methods
Patients diagnosed with transluminal broncholiths in Lanzhou University Second Hospital between January 2010 and August 2018 were enrolled in this retrospective study. Ethical approval for human subjects was obtained from the research ethics committee of Lanzhou University Second Hospital (Approval Number: 2020A-049), and the requirement for informed consent was waived by the ethics commission. The inclusion criteria were as follows: (a) transluminal broncholiths as confirmed by chest CT, bronchoscopy or pathology; (b) no other pulmonary malignant tumors; (c) no improvement of clinical situations by non-interventional treatments. Age, gender, symptoms, and signs, imaging characteristics, treatment methods, outcomes as well as complications were retrospectively analyzed. Statistical analysis was carried out using the SPSS 13.0 software (SPSS Inc., Chicago, IL, USA). Group comparisons were performed using Fisher’s Exact Test. P < 0.05 was considered to be statistically significant.
Results
Clinical presentation, imaging characteristics, and bronchoscopy findings
Twenty-eight patients diagnosed with transluminal broncholiths, including 13 males (46.4%) and 15 females (53.6%) were enrolled in this study. The age ranged from 27 to 78 years, with an average of (53.2 ± 10.6) years. There were 36 pieces of transluminal broncholiths, of which four patients each had two transluminal broncholiths and two patients each had three transluminal broncholiths. Among the 28 patients, 20 had the history of tuberculosis, four had the history of pneumoconiosis and one had the history of lobectomy for bronchopulmonary mucinous adenocarcinoma; the remaining three patients had no clear causes, but postoperative pathology proved that one was aspergillus infection accompanying a broncholith and two were tuberculosis. The most common symptom was cough and expectoration, other symptoms were hemoptysis, chest pain, dyspnea and lithoptysis. The baseline characteristics and clinical symptoms are shown in Table 1.
Baseline characteristics and clinical presentation of the patients enrolled in this study.

All 28 patients underwent chest CT examination. The results showed high-density plaque in the bronchial lumen with obvious calcification, which blocked the bronchial lumen and further led to distal bronchial stenosis, bronchiectasis, emphysema, atelectasis or pulmonary consolidation (Figure 1). The imaging characteristics of transluminal broncholiths are summarized in Table 2.

Chest CT imaging findings in patients with transluminal broncholiths. The results showed high-density plaque in the bronchial lumen with obvious calcification: (a) transluminal broncholiths located in right upper lobe, (b) transluminal broncholiths located in bronchus intermedius, and (c) transluminal Broncholiths after resection of left upper lobe due to bronchopulmonary mucinous adenocarcinoma.
Imaging characteristics and bronchoscopy findings of the patients enrolled in this study.

When a transluminal broncholith is suspected based on clinical presentation and imaging characteristics, bronchoscopy is often employed to confirm the diagnosis by direct visualization of a calcified stone in the airway. The typical broncholith appears as a yellow or gray-yellow, hard and foreign body-like lesion (Figures 2 and 3). Thirty-six pieces of transluminal broncholiths were found in the 28 patients by bronchoscopy, of which four patients each had two transluminal broncholiths and two patients each had three transluminal broncholiths. The most common location of transluminal broncholiths was the right lung, especially the right middle lobe. The number of transluminal broncholiths located in right lung was 4.1-fold than those located in left lung (P < 0.01). The location of transluminal broncholiths found by bronchoscopy are also shown in Table 2.

Bronchoscopy findings in patients with transluminal broncholiths. The typical broncholith appears as a yellow or gray-yellow, hard, and foreign body-like lesion: (a) transluminal broncholiths located in right upper lobe, (b) transluminal broncholiths located in bronchus intermedius, (c) transluminal broncholiths located in right middle lobe, and (d) transluminal broncholiths after resection of left upper lobe due to bronchopulmonary mucinous adenocarcinoma.

Pathological manifestations of transluminal broncholiths: (a) hematoxylin and eosin staining of a broncholith (magnification × 100) and (b) fungal infection accompanying a broncholith was found by hematoxylin and eosin staining (magnification × 100).
Treatment
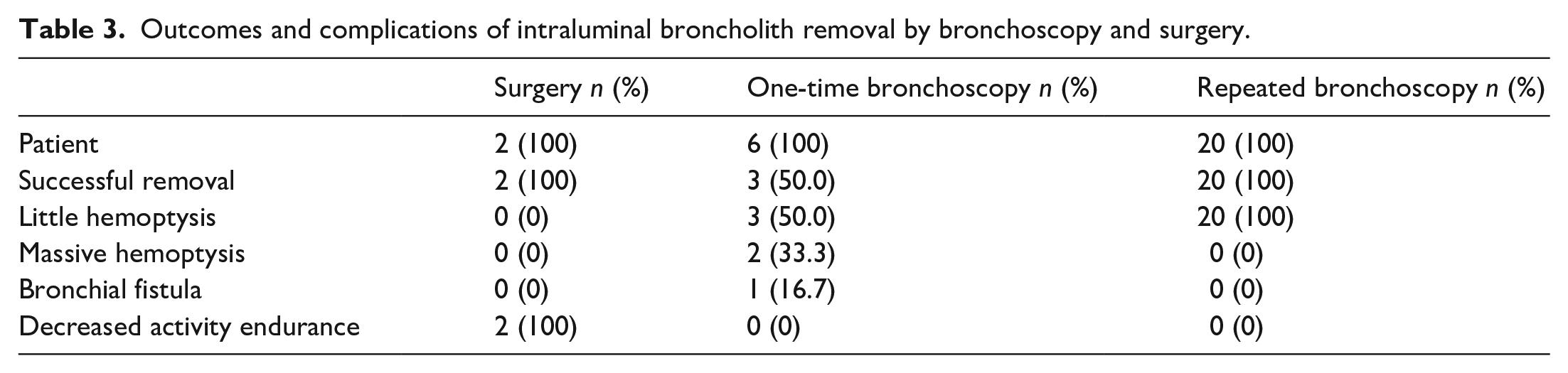
The treatment methods for transluminal broncholiths included bronchoscopy and surgery. Two patients were first assigned to receive surgical treatment: one was with massive hemoptysis and the other was judged to have the risk of massive hemorrhage in case of receiving bronchoscopic treatment, because the broncholiths were adjacent to bronchial arteries. Twenty-six patients were treated with bronchoscopy: six patients with single stone were treated with bronchoscopic forceps and net baskets for one time. However, broncholiths were removed successfully only in three patients, the other three patients were shifted into surgery because of massive hemoptysis or bronchial wall laceration occurring during bronchoscopy. Twenty out of the 26 patients were treated with repeated bronchoscopic lithotripsy: First, the intraluminal part of the broncholiths was fragmented and removed segmentally with foreign body forceps to relieve the obstructive symptoms. Then the remaining part of broncholiths within the bronchial lumen was removed eventually by repeated bronchoscopy during monthly follow-up period. The detailed results are shown in Table 3.
Outcomes and complications of intraluminal broncholith removal by bronchoscopy and surgery.
Outcomes and complications
The outcomes and complications of transluminal broncholith removal by bronchoscopy and surgery are also summarized in Table 3. Two patients firstly received surgical treatment due to massive hemoptysis or having the risk of massive hemorrhage. Two patients with broncholiths in right middle lobe had a complication of 200 ml massive hemorrhage during stone removal via bronchoscopic forceps. Eventually they received right middle lobe resection to treat the broncholiths and hemorrhage. One patient with broncholiths in right middle lobe underwent surgical resection of the right middle and lower lobes due to complicating with bronchial wall laceration during one-time removal of stones with bronchoscopic forceps. There was little bleeding in the other 23 patients who underwent complete or partial removal of broncholiths by foreign body forceps under bronchoscope. After local application of 1:10,000 adrenaline solutions, these small amounts of bleeding stopped.
Twenty-two transluminal broncholiths had obvious granulation tissue around the lesion after the first time of endoscopic stone extraction. Among these granulation tissue, 16 cases were removed by cryotherapy, four cases were removed by cryotherapy combined with high-frequency electrotome, and the remaining two cases were removed by biopsy forceps.
All the 28 patients were followed up for 5 months after broncholith removal. Five patients who received partial lung resection were recovered but with decreased activity endurance. The clinical symptoms disappeared completely in 21 patients and improved in two patients. There was no death in the 28 patients. During the follow-up period, bronchoscopy found that granulation tissue was completely removed and bronchial mucosa became smooth in all patients (Figure 4).

Transluminal broncholiths located in the left main bronchus were removed with basket and local granulation tissue was cleared with cryoablation under bronchoscope: (a) transluminal broncholiths located in the left main bronchus, (b) the stone was removed with basket under bronchoscope, (c) the residual granulation tissue after removal of the stone under bronchoscope, and (d) granulation tissue was completely cleared and bronchial mucosa became smooth.
Discussion
Broncholithiasis is a rare clinical disease. Tuberculosis is the most common causative organism both in China and Europe, 8 while histoplasmosis is the main infectious etiology in North America. 3 Less common causes include actinomycosis and silicosis. 9 The etiologies of broncholiths found in this study mainly included tuberculosis and pneumoconiosis, followed by lobectomy and aspergillus infection, which is consistent with previous research results. Since bronchial irritation and obstruction caused by broncholiths are main clinical manifestations,10,11 the treatment target for transluminal broncholiths should be to remove the intraluminal part of the broncholiths, relieving obstruction and improving symptoms. When the stone embedded in the bronchial wall is loose, it can be successfully removed by bronchoscopy without serious complications. It should be remembered that more complications can occur due to erosion of a branch of the bronchial artery during the procedure. Transluminal broncholiths without clinical symptoms should be followed up. It is unnecessary to treat them and some stones can even be coughed up by patients. 12
Several studies have reported successful experience in surgical treatment of transluminal broncholiths.13 –15 For broncholiths in close proximity to the mediastinum, surgical treatment should be preferred due to the possibility of massive bleeding via eroding the surrounding bronchial artery. 15 If there are contraindications to surgical treatment, endobronchial therapy can be considered, but it must be fully prepared and evaluated before the procedure. 2 Surgery is a classic method to treat transluminal broncholiths, and the inflammatory tissue around the stones should also be removed. Studies have reported that 80%–95% patients who need surgical treatment undergo segmentectomy or lobectomy and it is difficult to separate tissues in the surgical field due to distortion and adhesion during operation. 3 Therefore, surgical treatment is more traumatic and often intolerable to many patients, especially the elderly.
In this study, massive hemorrhage happened in two patients and bronchial wall laceration happened in one patient during one-time removal of stones with bronchoscopic forceps. The complication of massive hemorrhage was likely due to the invasion of transluminal broncholiths on large blood vessels, while bronchial wall laceration was related to the deep invasion of transluminal broncholiths on bronchial wall. Coincidentally, the three transluminal broncholiths were located in right middle lobe, which might be associated with the high incidence of right middle lobe stones, but had nothing to do with the occurrence of fatal complications. Twenty-six pieces of transluminal broncholiths were removed by repeated bronchoscopic lithotripsy: the intraluminal part was segmentally removed first to relieve symptoms, while the transmural part was retained without special treatment. During the residual stones further slowly moving into the lumen, the surrounding granulation tissue repaired the wound by itself. Regular removal of stones entering the lumen can achieve the desired therapeutic goals in the absence of severe hemoptysis and other serious conditions. Ferguson et al 16 have reported that two transluminal broncholiths were found adjacent to the large blood vessels by three-dimensional reconstruction CT, the intraluminal part was crushed and removed by Holmium laser, while the transmural part was retained, which relieved symptoms without serious complications. Recently Cheng et al. 6 have found that the pulse characteristics of Holmium laser are very suitable for lithotripsy. Since its energy is easy to be absorbed by water and its penetration is weak, it has little damage to normal tissues. Therefore, it is safe and effective in the treatment of broncholiths, especially for large broncholiths or transluminal broncholiths which are difficult to be removed directly through bronchoscopy.
Patients with transluminal broncholiths need regular bronchoscopy after removal treatment to observe if stones recur or residual granulation tissue blocks the lumen. Generally, the residual granulation tissue in bronchial cavity after lithotripsy can repair themselves and subside after the removal of etiologies and control of surrounding inflammation with a satisfactory prognosis. However, in case that granulation tissue affects secretion drainage and causes obstructive symptoms, bronchoscopic treatment is needed. Cryoablation is an effective method for clearance of granulation tissue, whose complications of bronchial perforation and bronchial stenosis are less than those of high-frequency electrotomy. 17
There are several limitations in the present study. First, our study retrospectively analyzed 28 patients with transluminal broncholiths diagnosed in Lanzhou University Second Hospital between January 2010 and August 2018. Data from multiple hospitals with larger size of number are needed to further validate our findings.
Second, we did not verify the detailed clinical characteristics of patients requiring repeated treatment or a one stage removal, such as the size or location of stones and other characteristic manifestations on CT or bronchoscopy.
Conclusions
The management of broncholithiasis should be individualized. Patients asymptomatic or with mild symptoms should be followed up regularly. Treatment strategy for patients with obvious symptoms should be chosen according to clinical presentation, imaging characteristics, and bronchoscopy findings. If broncholiths cause serious injury of distal lung tissue, massive hemoptysis, bronchial fistula or the diagnosis of broncholiths is unclear, surgical treatment is needed. In case that a transluminal broncholith is difficult to be removed completely, the treatment target should be to remove the intraluminal part of the stones under bronchoscope, relieving obstruction so as to improve clinical symptoms. Then during the regular follow-up period, to find and remove the residual stones which further slowly move into the lumen under bronchoscope.
Footnotes
Author contributions
Hong Wang and Yixin Wan designed the study; Fangwei Li and Li Zhang analyzed and organized the results; Fangwei Li wrote the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital (No. CY2020-BJ07).
Ethical approval
Ethical approval for this study was obtained from the research ethics committee of Lanzhou University Second Hospital (Approval Number: 2020A-049).
Informed consent
Informed consent was not sought for the present study because informed consent was waived by the ethics commission due to the retrospective nature of the study.
Trial registration
This randomized clinical trial was not registered because the retrospective observational study nature of the study.