
Abstract
The catheter related blood stream infections (CRBSI) in hemodialysis (HD) patients with vein tunneled cuffed catheter (TCC) and misuse of antibiotic in clinical practice seriously affected the prognosis of MHD patients. The present study aimed to investigate the pathogen distribution and drug resistance of CRBSI in HD patients with TCC to guide clinical empirical pharmacy. The clinical data of 75 HD patients with TCC diagnosed with CRBSI between January 2011 and March 2015 were retrospectively collected, and the distribution and drug resistance of pathogens were analyzed. In 75 HD patients with TCC diagnosed with CRBSI, there were 33 patients with positive blood culture, and the positive rate of blood culture was 44%. The majority of the 33 pathogens were Gram-positive bacteria (22 strains, accounting for 66.7%). Gram-positive cocci hardly resisted to vancomycin and linezolid, while the resistance rate to penicillin G nearly reached to 100%. Gram-negative bacilli had low resistance rates to carbapenems and quinolone antibiotics, and the resistance rate to cephalosporins antibioticsexceeding 50%. The positive rate of blood culture in 75 HD patients with TCC diagnosed with CRBSI is low. The pathogens resulting in CRBSI in HD patients are mainly Gram-positive bacteria which are significantly resistant to penicillin G, and have a low resistance rate to methicillin. Gram-negative bacteria have high resistance rates to commonly used antibiotics. The pathogen examination should be performed as early as possible and effective antibiotics should be chosen according to drug sensitivity test results in CRBSI in HD patients.
Keywords
Introduction
With the increase of the incidence of uremia and the development of Hemodialysis (HD) technology, there are more and more maintained Hemodialysis (MHD) patients, and the selection, establishment and protection of vascular access (VA) have become particularly important. Arteriovenous fistula (AVF) is the preferred vascular access to MHD patients for the long-term patency.1,2 Furthermore, vein tunneled cuffed catheter (TCC) has been widely used in HD patients, and become an important and optimal VA to the HD patients who are with immature AVF, limited life span, poor cardiac function, and poor vascular conditions. 3
As TCC has been widely used in MHD patients, the catheter complications have become increasingly common, such as catheter related infection, malfunction, and central stenosis.4,5 Recently, catheter related-blood stream infections (CRBSI) have been increasing, and CRBSI-related deaths are also significantly increased.6–8 The misuse of antibiotic in clinical practice is prone to leading to the emergence of drug-resistant bacteria strains, which not only increases the expense of patients and the number of hospitalizations, but also seriously affects the prognosis of MHD patients. Some of CRBSI patients have secondary serious complications, such as infective endocarditis, suppurative arthritis, epidural abscess, and other suppurative infections, which Staphylococcus aureus infection is an independent risk factor for.9,10 Antibiotic selection for CRBSI caused by Staphylococcus aureus especially drug resistant strains, is particularly important. In the case of severe secondary complications of CRBSI, the average length of hospital stay, number of hospital admissions and treatment costs are all increased compared with the simple CRBSI. 10 Therefore, analysis of common pathogenic bacteria distribution and antibiotic susceptibility of bacteria of CRBSI in HD patients with TCC has become increasingly important for the treatment and prognosis by clinicians. In the present study, the bacterial distribution and drug sensitivity of 75 HD patients with TCC diagnosed with CRBSI were retrospectively analyzed, providing a reference for clinical diagnosis and treatment.
Materials and methods
Patients and data collection
This was a single-center retrospective observational study to analyze the bacterial distribution and drug sensitivity in HD patients with TCC diagnosed with CRBSI. Total 75 HD patients with TCC diagnosed with CRBSI were recruited between January 2011 and March 2015 from the department of nephrology of the First Affiliated Hospital of USTC (Anhui Provincial Hospital, Hefei, China). Catheter exit infection, catheter related tunnel infection, and other non-catheter related infection were excluded in HD patients with TCC. The pathogen distribution and drug resistance in 75 HD patients with TCC diagnosed with CRBSI were collected and analyzed. This study was conducted in accordance with the Declaration of Helsinki and with approval from the ethics committee of the Anhui Provincial Hospital. The data in this study were derived from previous medical records, did not disclose patient privacy, consisted with the principles expressed in the Declaration of Helsinki. This study met the criteria for waiving informed consent.
Diagnostic criteria
All patients met the five stage and diagnostic criteria of chronic kidney disease (CKD) according to the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines, 11 and were being treated on HD with TCC (Tyco Healthcare, USA) for more than 3 months, whose AVF lost function or were not recommended for re-establishment. We diagnosed catheter-related bloodstream infection (CRBSI) in catheter-dependent patients on hemodialysis with a clinical suspicion of infection (fever especially on dialysis day, rigors, altered mental status, or unexplained hypotension), blood cultures growing the same organism from the catheter hub and a peripheral vein (or the dialysis bloodline), and absence of evidence for an alternative source of infection. 5 When blood culture was one positive or two negative, and the patient undergoing HD with TCC had clinical suspicion of infection, elevated white blood cell counts in peripheral blood and absence of evidence for an alternative source of infection, the patient was also clinically diagnosed with CRBSI.
Methods of catherization
The TCC was produced by Tyco Healthcare, USA. All patients preferred jugular vein catheterization, which was carried out by professional technicians in the operating room. Seldinger technique was applied to catheter the TCC, and the Cuff to the exit of the skin was about 1–2 cm. The tip of TCC should reach the connection between the vena cava and the right atrium, or the top of the right atrium to ensure adequate blood flow. The catheter was sealed with anticoagulant and the bleeding was stopped by salt bag.
Identification of bacteria
The aseptic operation was strictly applied, then the blood culture of catheter arteriovenous end and a peripheral venous was carried out respectively, each of which Aerobic bacteria and anaerobic bacteria were cultured in. The blood samples were inoculated in sheep bloodagar plate (Bio-Merieux, France) and incubated for 18–24 h. The positive culture specimens were identified by Vitek automatic microbiological analysis system (Bio-Merieux, France).
Drug susceptibility test
The Vitek automatic microbiological analyzer (Bio-Merieux, France) were used in the drug sensitivity test, and the results of drug sensitivity were determined according to the 2004 edition of National Committee for Clinical Laboratory Standards (NCCLS). 12 For Gram positive bacteria, the susceptibility to Penicillin G, Methicillin, Moxifloxacin, Quinupristin, Clindamycin, Rifampicin, Erythrocin, Bactrim, Gentamicin, Tetracycline, Linezolid, Tigecycline, Levofloxacin, Vancomycin, and Macrodantin had been tested. For Gram negative bacteria, the susceptibility to Amikacin, Aztreonam, Cefepime, Bactrim, Ciprofloxacin, Ceftriaxone, Cefoperazone-sulbactam, Gentamicin, Imipenem, Levofloxacin, Tobramycin, and Piperacillin-tazobactam had been tested.
Statistical analysis
All statistical analysis were performed using IBM SPSS Statistics 20.0 version (IBM Corporation, Armonk, NY, USA). A normal distribution of continuous variables was summarized as means ± standard deviation (SD), while a skewed distribution of continuous variables was expressed as medians with interquartile ranges. The number (n) and percentage (%) in each category were calculated for categorical variables.
Results
General information of CRBSI patients
A total of 75 patients developed CRBSI. The patients included 34 males and 41 females aged between 16 and 82 years. The basic kidney diseases were 51 of chronic glomerulonephritis, nine of diabetic kidney disease, seven of polycystic kidney, four of hypertensive kidney disease, three of hyperuricemia kidney disease, and one of chronic obstructive kidney disease, respectively.
Distribution and constitution of isolated pathogens
The blood culture of catheter arteriovenous end and a peripheral venous was carried out respectively. There were 33 patients with positive blood culture, and the positive rate of culture was 44%. Pathogen distribution was dominated by Gram-positive bacteria, while Staphylococcus aureus accounted for 45.5%. The distribution of Gram-negative and Gram-positive bacteria are shown in Table 1.
Distributions of pathogens isolated from blood culture.

Drug sensitivity test results of Gram-positive bacteria
The data showed that Gram-positive cocci hardly resisted to vancomycin, linezolid, tigecycline, and furantoin, while the resistance rate to penicillin G was 100% (22/22) and to Methicillin just to 22.7% (5/22). The susceptibility rate of Staphylococcus aureus to vancomycin, furantoin, gentamicin, linezolid, quinupristin, moxifloxacin, and tigecycline was 100% (15/15), among which methicillin-resistant Staphylococcus aureus (MRSA) were detected accounting for 20%. The sensitivity rate of other Gram-positive bacteria except Staphylococcus aureus to vancomycin, linezolid, tigecycline, and furantoin was 100% (7/7) (Table 2).
Drug sensitivity of Gram-positive bacteria to common used antibiotics.

Drug sensitivity test results of Gram-negative bacteria
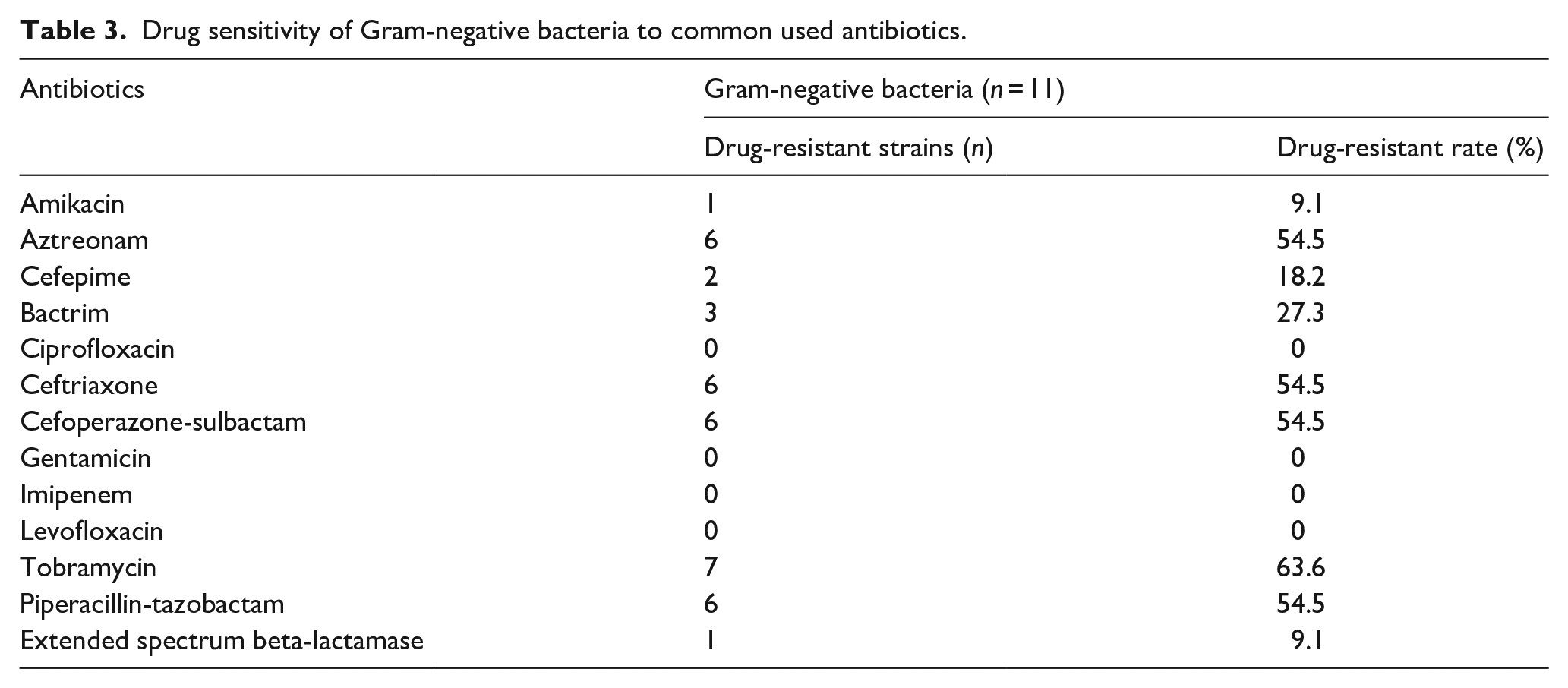
The Gram-negative bacilli had low resistance rates to imipenem, levofloxacin, gentamicin, and ciprofloxacin. The susceptibility rate of Gram-negative bacilli to imipenem was 100% (11/11), and the resistance rate of Gram-negative bacilli to ceftriaxone, piperacillin-tazobactam, tobramycin, and cefoperazone-sulbactam was 54.5% (6/11), 54.5% (6/11), 63.6% (7/11), and 54.5% (6/11) respectively (Table 3).
Drug sensitivity of Gram-negative bacteria to common used antibiotics.
Discussion
TCC is mainly suitable for uremia patients with immature arteriovenous fistula, limited life span, poor cardiac function and poor vascular conditions. 3 CRBSI seriously affects the service life of catheter and becomes the first cause of catheter disuse. 13 Analysis of common pathogenic distribution and antibiotic susceptibility of bacteria of CRBSI in HD patients with TCC has become increasingly important for the treatment and prognosis by clinicians.
This study showed that Gram-positive bacteria infection was the most common CRBSI with TCC, and Staphylococcus aureus and Staphylococcus epidermidis were the most common infectious bacteria, which was consistent with previous literature reports.14–16 All Gram-positive bacteria had a sensitivity rate of 100% to vancomycin, linezolid, tegacycline, and furantoin, and a resistance rate of 100% to penicillin G. There were three MRSA strains, accounting for 20% of Staphylococcus aureus infections, which was resistant to many commonly used antibiotics, such as beta-lactam, aminoglycosides, and quinolones, and may be only sensitive to vancomycin. Vancomycin has been widely used in clinical practice since 1958 and has become the preferred drug for treatment of MRSA infections. 17 But the emergence of vancomycin-resistant Staphylococcus and Enterococcus has been reported at present, 18 which may be related to the misuse of vancomycin. Vancomycin is mainly metabolized by the kidney and has nephrotoxicity, Dietrich et al showed that the incidence of renal impairment in vancomycin adverse reactions was 7–17%. 19 For patients with chronic renal failure (CRF), the glomerular filtration rate decreases and drug clearance slows down which may further aggravate renal function damage, the abuse of vancomycin may lead to the emergence of drug-resistant strains, and it can be eliminated by HD. Given the high rate of hospitalization and mortality in CRBSI, it is harder to keep balance between taking a rapid and effective treatment regimen and control use of vancomycin in the clinical treatment process, and more attention should be paid to the etiological examination so as to timely adjust the treatment plan. In addition, the safe interval and appropriate dose of vancomycin for HD patients are still unclear, and large sample data and prospective clinical trials are still lacking.
Gram-negative bacteria infection accounted for 33.3% in this group of data, including two strains of Enterobacter cloacae, two strains of Fluorescent pseudomonad, two strains of Klebsiella pneumoniae, one strain of Acinetobacter haemolyticu, one strain of Serratia marcescen, one strain of Enteroaerogen, one strain of Human pale bacillu, and one strain of Aeromonas hydrophila, most of which are the conditional pathogenic bacteria. This may be related with CRF patients with low immunity, 10 poor nutritional status, 10 and long-term hospitalization. One of the two strains of Klebsiella pneumoniae was found to be extended spectrum beta-lactamase (ESBL) positive, which was the main mechanism of resistance to beta-lactamide antibiotics. In this case, the use of three generations of cephalosporins and penicillin antibiotics are often ineffective. Previous studies have shown that ESBL-producing Klebsiella pneumoniae is a threat to clinical treatment.20,21 In addition, the results showed that the Gram bacteria were the most sensitive to imipenem, levofloxacin, gentamicin and ciprofloxacin, with the sensitivity rate of 100%, while resistant to other common used antibiotics such as ceftriaxone, piperacillin /tazobactam, cefoperazone/sulbactam, with the resistance rate of 54.5%. This may be related to the empirical use and tube sealing of third-generation cephalosporin and broad-spectrum penicillin in CRBSI patients. It can inferred that if the third generation of cephalosporin is administered or sealed in the catheter empirically, treatment may fail for patients diagnosed with CRBSI in our hospital, and it is necessary to strengthen the management of high-risk patients, pay attention to the hand hygiene of medical staff, and do a good job in disinfection and isolation and other protective measures.
This research had several limitations. Our study was just a single-center, observational research, the sample was small, and had no prognosis of patients. We could not get a causal conclusion, and the conclusions could not exclude the influence of the confounding factors (such as Specimen contaminated). Whether our research findings can be generalized to other clinical center remains uncertain.
Conclusion
The positive rate of blood culture in 75 HD patients with TCC diagnosed with CRBSI is low. The pathogens resulting in CRBSI in HD patients are mainly Gram-positive bacteria which are significantly resistant to penicillin G, and have a low resistance rate to methicillin. Gram-negative bacteria have high resistance rates to commonly used antibiotics. The pathogen examination should be performed as early as possible and effective antibiotics should be chosen according to drug sensitivity test results in CRBSI in hemodialysis patients.
Footnotes
Acknowledgements
The authors would like to express sincere gratitude to our colleagues who contributed to the research while their names do not appear on the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from the ethics committee of the Anhui Provincial Hospital. (Approval number/No.2020-P-063).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The data in this study were derived from previous medical records, did not disclose patient privacy, consisted with the principles expressed in the Declaration of Helsinki. This study met the criteria for waiving informed consent.
Trial registration
Not applicable.