
Abstract
To evaluate the clinical efficacy of screw fixation with cortical bone trajectory for adjacent segment disease after lumbar interbody fusion. A total of 14 patients with adjacent segment disease were enrolled, and a retrospective analysis was performed. All patients experienced posterior lumbar interbody fusion of the affected segments combined with internal fixation of cortical bone trajectory screw. Operation time, intraoperative blood loss, and complications were recorded. Clinical outcomes was evaluated by Visual Analogue Scale, Oswestry disability index, and Japanese Orthopaedic Association score. X-ray and computed tomography and sagittal reconstruction were used to check regularly during the follow-up. Bone graft fusion rate was evaluated by Brantigan classification. Preoperatively, Visual Analogue Scale, Oswestry Disability Index, and Japanese Orthopaedic Association scores were 7.0 ± 1.0, 72.2 ± 3.2, and 11.9 ± 1.3 points, respectively. At the 12th month after surgery, their scores were 1.9 ± 0.7, 28.6 ± 1.2, and 23.7 ± 0.9 points, respectively, which were significantly improved compared with those before surgery, and there were statistical significance in all differences (all p < 0.05). At the 12th month after surgery, X-ray and computed tomography showed there were no complications related to internal fixation, such as breakage and displacement. At the 12th month after surgery, according to the Brantigan classification, 10 patients were classified as Grade E, 3 as Grade D, and 1 as Grade C, with a fusion rate of 92.9%. At the final follow-up, clinical outcomes were assessed by the Stauffer-Coventry criteria: there were 10 patients with excellent outcomes, 1 with good outcomes, 3 with fair outcomes, and 0 with poor outcomes, with an excellent and good rate of 78.6%. The clinical outcomes of posterior lumbar interbody fusion combine with cortical bone trajectory screw for adjacent segment disease without removing the previous internal fixator were satisfactory, but further clinical researches were still required to explore its long-term outcome.
Introduction
Adjacent segment disease (ASD) is a condition that new lesions occur in the spine motion segment adjacent to the surgical segment after lumbar interbody fusion, and causes some clinical symptoms.1,2 Generally, these factors of ASD development can be divided into two broad categories: patient factors which include age, obesity, preexisting degeneration of adjacent discs, menopause, and sacral inclination, and surgical factors which include length of fusion, stiffness of the construct, radical decompression, disruption of facet capsules (either during exposure or by the instrumentation), loss of lumbar lordosis, and sagittal and coronal imbalance. 3 It was reported that patients who suffered ASD after lumbar interbody fusion were up to 14%, and ASD was one of the key reasons for symptoms relapse after lumbar interbody fusion and even revision surgery. 4 Patients with ASD, who were insensitive to conservative treatment, may need surgical treatment.3,5 So far, posterior lumbar interbody fusion (PLIF) has been one of the most common revision surgery. 6 Because it is necessary to remove the previous internal fixator, conventional revision surgery can increase the risk of complications, such as postoperative infections, incision pain, and blood transfusion. Cortical bone trajectory (CBT) screw technique 7 is a novel fixation method, which has a different entry point and direction of the trajectory compared with the conventional pedicle screw, and a cortical bone screw can be inserted into a vertebral body even if a pedicle screw has already existed, so the adjacent segment can be immobilized without removing the previous internal fixator. In this study, the data of patients with ASD who experienced CBT screw fixation was analyzed retrospectively to evaluate its clinical outcome in treating ASD.
Materials and methods
This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of Xuzhou Central Hospital. Written informed consent was obtained from the participants.
Inclusion and exclusion criteria
Inclusion criteria were as follows: (1) patients with ASD-caused severe lumbar or leg pain, intermittent claudication, decreased muscle strength in legs, hypoesthesia, and so on; (2) poor outcome after formal conservative treatment for more than 3 months; (3) imaging findings being consistent with clinical symptoms; (4) preoperative computed tomography (CT) and magnetic resonance imaging (MRI) making a definite diagnosis and confirming that the residual space of pedicle in the surgical segment was enough to insert a CBT screw. Exclusion criteria as follows: (1) Patient experiencing operation for inflammation, tumor, and trauma; (2) inadequate residual space of the pedicle to insert a CBT screw; (3) patients with other related diseases affecting the evaluation of clinical efficacy.
General information
Based on the above inclusion and exclusion criteria, a total of 14 patients (8 males and 6 females) who received CBT screw insertion in our Department of Orthopedics from January 2015 to August 2016 were enrolled into this study. They aged from 42 to 71 years old [mean, (65.2 ± 7.2) years old]. Previous surgical segments were located at L4/5 in nine patients and at L5/S1 in five patients; ASD-affected segments were located at L4/5 in five patients, at L3/4 in six patients, and at L5/S1 in three patients. There were 10 patients with lumbar pain, 8 with intermittent claudication, 9 with leg radicular pain, and 11 with sensory disability in legs. The interval between two operations ranged from 23 to 60 months, with a mean of 43.643 ± 13.826 months (Table 1). Preoperatively, all patients were examined by X-ray, CT + sagittal reconstruction, and lumbar MRI.
Summary of demographics in 14 patients with ASD.

ASD: adjacent segment disease.
Surgical procedure
After induction of general anesthesia, the patients were placed in the prone position. An incision was made in the midline of the low back. The bilateral muscle was dissected along the spinal process to the lamina, and attention was paid to protect the integrity of supraspinous, interspinous ligaments and joint capsules. The surgical segment was confirmed by C-arm. The internal fixator in the previous surgical segment was not removed, and a CBT screw was inserted into the segment to be decompressed (Figure 1). The entry point was isthmus-guided, which was located at 1 mm below the transverse process, and 3–5 mm medial to the lateral border of the isthmus. When the screw entered, it was tilted upside down at an angle of 30°C–45°C and tied at an angle of 10°C–20°C. In some patients, because of vertebral rotation or scoliosis, the entry point could not be defined. Thus, the lamina 2 mm inferior and 2 mm medial to the inferomedial margin of the superior articular process could be selected to be an entry point; alternatively, the entry point could be at the intersection point of the vertical line of the middle superior articular process with the horizontal line 1 mm below the transverse process. After removal of the cortical bone at the entry point, a blunt-pointed pedicle access appeared, and then, 1.5 mm in diameter was used to gain access to the pedicle, and four walls of the pedicle were explored finally by a pedicle probe. After confirmation of C-arm and tapping, a CBT screw with proper length was screwed slowly in the direction of the probe (in general, the screw of 3.5–5.0 mm in diameter and 25–35 mm in length). Decompression procedure was performed on the side where the stenosis was significant or the symptoms were serious. In order to ensure thorough decompression and facilitate fusion cage insertion, traditional pedicle screw insertion was performed at cranial segment. After meticulous hemostasis, a negative pressure drainage tube was placed and the incision was sutured layer by layer.
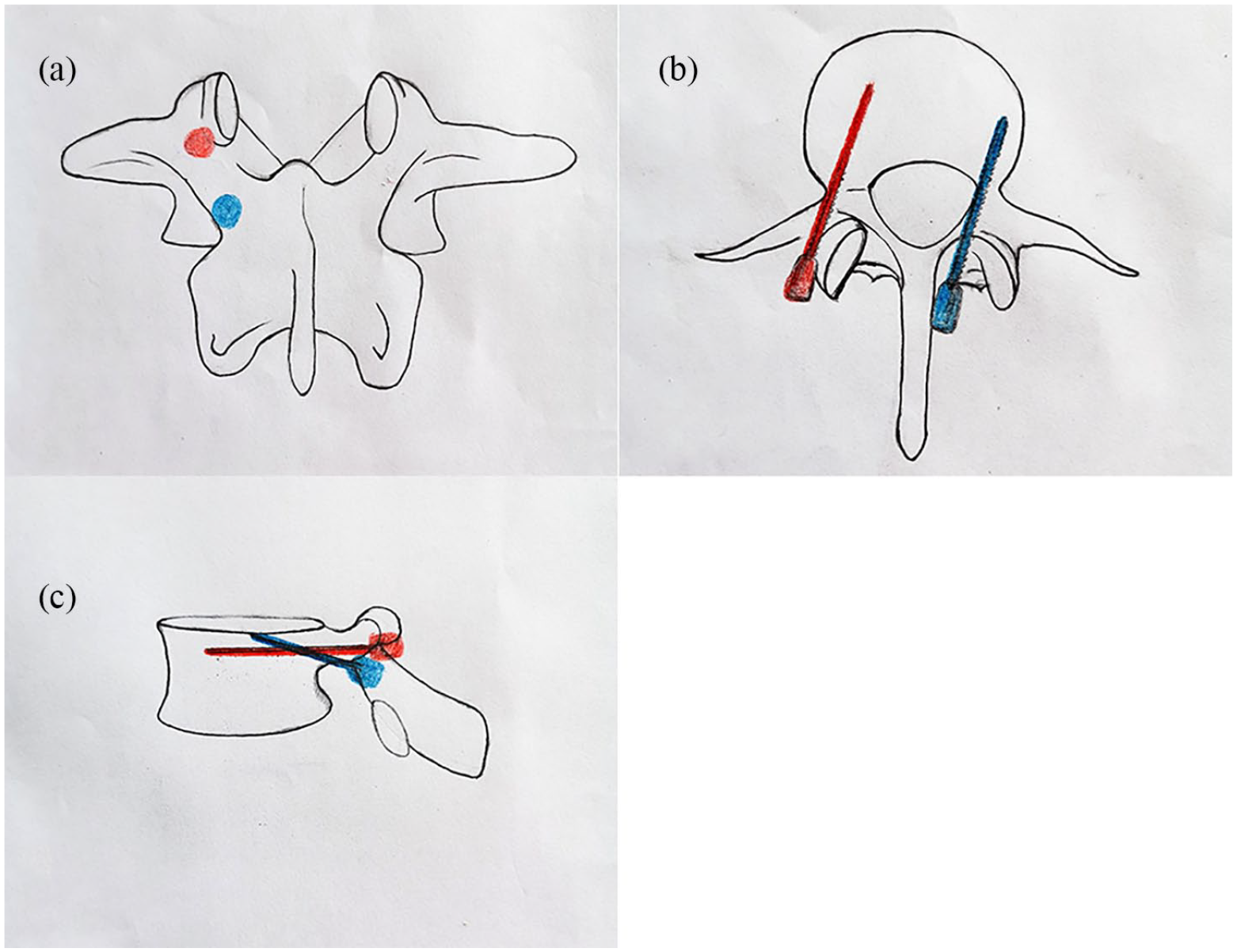
Diagrams of starting points of pedicle screw (red circle) and CBT screw (blue circle) on anteroposterior view (a). The orientation of pedicle screw (red screw) and CBT screw (blue screw) on cross-sectional view (b) and lateral view (c).
Postoperative management
Prophylactic antibiotics was used at 24 h after surgery. Trunk extension exercises and straight leg raising exercises begun to take on bed immediately after operation. Ambulation was allowed under the protection of the brace after the drainage tube was removed, and normal activities gradually recovered after 6 weeks.
Observations and outcomes evaluation
Operation time, intraoperative blood loss and complications were recorded. Neurologic function was evaluated by the scales of Japanese Orthopedics Association (JOA), 8 the low back pain and leg pain was evaluated by the 10-point visual analog scale (VAS), 9 and the clinical outcomes were assessed by the Oswestry Disability Index (ODI). 10 The VAS scores were recorded before operation, at the third month after operation, and at the final follow-up. The JOA scores and the ODI scores were recorded preoperatively, at the third month after operation, and at the final follow-up. The radiographic examinations, such as lumbar X-rays and three-dimensional computed tomography (3DCT) scans, were performed before and after operation, at the 12th month after operation, and at the final follow-up. At the 12th month follow-up, inter-body bone fusion was evaluated by the Brantigan grade, 11 and when the grade was classified as grade D or grade E, the bony fusion was considered to be completed successfully. At the last follow-up, clinical outcome was evaluated by the Stauffer-Coventry criteria, and the satisfaction rate was calculated.
Statistical analysis
All results were expressed as mean ± standard deviation. SPSS 11.0 statistical software (SPSS, Inc, Chicago, Illinois) was used. The quantitative data was analyzed by paired t-test, and the categorical data was analyzed by Chi-square tests or Fisher’s exact tests. The p < 0.05 was considered to be statistically significant.
Results
All operations were successful. The operation time was ranged from 130 to 250 min, with a mean of 166.4 ± 33.1 min; the estimated blood loss was ranged from 180 to 420 ml, with a mean of 331.4 ± 80.1 ml. No death or severe complications, such as nerve injury and deep infection, was reported during the peri-operative period. The average follow-up time was 26 months (19–48 months).
The average VAS score was 7.0 ± 1.0 preoperatively, which was improved significantly to 3.6 ± 0.8 at the third month after operation (p = 0.000) and 1.9 ± 0.7 at the final follow-up.
The average ODI was 72.2 ± 3.2 preoperatively, which was improved significantly to 38.4 ± 1.1 at the third month after operation (p = 0.000) and 28.6 ± 1.2 at the final follow-up.
The average JOA score was 11.9 ± 1.3 preoperatively, which was improved significantly to 23.7 ± 0.9 at the third months after operation (p = 0.000) and 25.4 ± 1.0 at the final follow-up (Table 2).
Comparison of VAS, ODI, and JOA scores preoperatively, at 3 months after operation and at the last follow up duration for patients undergoing posterior lumbar revision surgery (x ± s).

At the 12th month after surgery, radiography and 3DCT was performed, which revealed internal fixation-related complications, such as screw pullout, breakage, and displacement of internal fixation, did not happened. Based on the Brantigan-Steffee classification, 10 patients were classified as Grade E, 3 as Grade D, and 1 as Grade C, with a bone graft fusion rate of 92.9%. At the final follow-up, all of the patients obtained excellent bony fusion. At the final follow-up, clinical outcomes were assessed by the Stauffer-Coventry criteria: there were 10 patients with excellent outcomes, 1 with good outcomes, 3 with fair outcomes, and 0 with poor outcomes, with an excellent and good rate of 78.6%. A typical case was showed in Figure 2.

Preoperative X-ray films (a) and (b) demonstrated that after PLIF, excellent L4-S1 interbody bony fusion was obtained, and the adjacent segment instability at L3–4 segment was observed. Preoperative MRI (c) and (d) revealed that the nucleus pulposus of L3–4 disc was sequestrated and prolapsed at the lateral recess, and the nerve root canal was compressed. X-ray films (e) and (f) at 1 month after PLIF + internal fixation of CBT screw. X-ray films (g) and (h) and 3D-CT (i) and (j) at 24 months after PLIF + internal fixation of CBT screw revealed that the internal fixture was well-located and interbody bony fusion was obtained.
Discussion
Lumbar inter-body fusion was the most commonly used procedure for spine surgery. With the aging of populations and advances in internal fixation technique, a growing number of people experienced lumbar inter-body fusion procedure. Therefore, more attention should be paid to the incidence of ASD after surgery. ASD was a common reason for revision lumbar surgery. 12 The revision procedures such as spinal endoscopy, laminectomy, anterior lumbar inter-body fusion, and posterior lumbar inter-body fusion had been reported. So far, PLIF was the most commonly used procedure. Conventional revision surgery required removal of the previous internal fixation devices when internal fixation and inter-body fusion on the adjacent involved segments were performed, which would increase operation time and iatrogenic injury.
CBT technique, proposed by Santoni et al., 7 is a technique - inserting a cortical bone screw in the vertebral column in a different way from the traditional pedicle screw technique. By changing the direction and point of the trajectory, this technique allowed the screw to maximize the contact area with the cortical bone in the pedicle and vertebral body, so as to increase the pullout strength of the screw. This technique was mainly used in senile patients with osteoporosis and decreased bone mineral density at the beginning of its design. To date, there have been many studies reporting that the CBT technique in treatment of spinal disease achieved similar or even better clinical efficacy than conventional internal fixation methods.13–15
CBT screw was placed on the vertebral interarticularis located at the inferomedial to the previous pedicle screw, and orientated from inside to outside without interfering with the previous pedicle screws, so the screw could be inserted into the vertebrae without removing the previous implants. Rodriguez et al. 16 first applied the CBT technique to patients with ASD caused by posterior lumbar interbody fusion, one more CBT screw was inserted into the vertebral column without removing the previous internal fixation device, and excellent clinical outcomes were achieved. Mullin et al. 17 conducted a clinical trial for patients having undergone traditional pedicle instrumentation previously to determine whether dual trajectories were feasible or not, of which the results indicated that successful dual trajectories were performed in 50% of the pedicles. In this cohort, the average operation time was 166.4 ± 33.1 min, the average intra-operative blood loss was 31.4 ± 80.0 ml, and there were no intra-operative complications, such as dural and cauda equina injury. At the final follow-up, the JOA scores, ODI, and VAS scores were improved significantly, compared with those before the operation. And the X-ray imaging showed there were no internal fixation-related complications, such as screw extraction, breakage, and displacement of internal fixation device. At the 12th month after surgery, according to bone fusion standard proposed by Brantigan-Steffee, 10 patients were classified as Grade E, 3 as Grade D, and 1 as Grade C, with a bone graft fusion rate of 92.9%, which was similar to results reported in the existing literature.
Besides no need for removal of the previous internal fixation devices, there were some other advantages in revision lumbar surgery using CBT screws. Firstly, advanced age was a high risk factor for ASD after lumbar spine surgery, and lumbar ASD with osteoporosis was common. 18 Because osteoporosis mainly involving cancellous bone had less impact on cortical bone, and left adequate contact area with the cortical bone, CBT screw could achieve rigid fixation and strong pullout resistance. CBT technique could make the best use of the bone surface of the pedicle complex, and maintaine the biomechanical strength of the internal fixation devices. 19 Kojima et al. 20 found that the CT value within the bone with CBT screws was almost over four times higher than that within the bone with the traditional trajectory. An in vivo study by Matsukawa et al. 21 indicated that the axial pullout resistance of the CBT screws was 30% higher than that of pedicle screws, and maximum insertional torque of the CBT screws was 1.7 times higher than that of traditional screws. Ueno et al. 19 used a double-trajectory technique to treat a patient with degenerative lumbar scoliosis and osteoporosis, for whom CBT screws and traditional pedicle screws were inserted in the same pedicle, and satisfactory effecacy was obtained. For ASD patients with osteoporosis, the fixation strength of the CBT screw might reduce the complications related to internal fixation. Moreover, because the entry point of the CBT screw was located at the pars interarticularis, inferomedial to the articular process, away from the joint capsule, it could reduce the damage to the joint capsule of the upper vertebral body, and theoretically decrease the incidence of ASD. Secondly, it had been indicated that there was a higher risk for damage to the dural sac and/or nerve root when a screw penetrated the interior or inferior wall of the pedicle, whereas the entry point and direction of CBT screw allowed the screw path to keep away from the spinal dura and the nerve root to reduce the risk of nerve injury. 22 Furthermore, it could also reduce muscle stripping and facet joints expose, with less surgical trauma and intra-operative blood loss.
When revision lumbar surgery was performed by the CBT technique, the following items should be paid attention to. Firstly, the entry point should be located carefully, the reasons for which were that facet joints might be damaged during the primary surgery, and with significant scar hyperplasia, the entry points might be masked. So far, there has been no consensus on the entry point in existing literature, and thus it should vary with each individual. Matsukawa et al. 23 believed that the entry point of the CBT screw was supposed to be the junction of the center of the superior articular process and 1 mm inferior to the inferior border of the transverse process, and in the lumbar spine the entry point of the CBT screw was always projected to the 5 o’clock orientation in the left pedicle and the 7 o’clock orientation in the right pedicle. Akpolat et al. 24 used the intersection point of the inferior border of the transverse process and the midline of the facet joint as the entry point. Iwatsuki et al. 25 proposed an isthmus-guided CBT screw insertion technique, and the entry point was defined at a point about 3 mm medial to the lateral margin of the isthmus, which was the superior margin of the intervertebral foramen. Considering individual difference, it was necessary to read the preoperative radiographic data very carefully to obtain accurate screw implantation. 26 Secondly, keep the correct direction and angle of the trajectory, in order to obtain adequate fixation strength and avoid nerve root injury. In normal conditions, the direction of the trajectory was tilted cranially on sagittal view and in-out in transverse section. In fact, specific angle always depended on fluoroscopy, which, in general, was tilted at an angle of 30°–45° craniocaudally and at an angle of 10°–20° from inside to outside. Thirdly, select proper traditional pedicle screw or use special CBT screw. For some patients, bony structure removal might be excessive during the primary surgery, so the entry point of the CBT screw was damaged, and as a result, it was difficult or impossible to implant the screws. Therefore, we recommend other surgical procedures, rather than reluctant screw insertion.
There are several limitations in this study. Firstly, the sample size is small and the follow-up time is short. In the future, multicenter, large sample, and long-term clinical observations are required to evaluate the clinical outcomes of CBT screw technique in the treatment of lumbar revision surgery. Secondly, large sample and long-term clinical study are required to evaluate the impact of CBT screw on the adjacent segment. Thirdly, any power calculation was not done for estimation of sample size selected for this study. In the future, it should be done. Last but not least, this is a retrospective follow-up study without control group, so compared with other procedures should be done in the future studies. And higher evidence level is required in the future, such as randomized controlled trials.
Conclusion
The clinical outcome of PLIF combine with CBT screw for ASD without removing the previous internal fixator were satisfactory, but the further clinical research is still required to explore its long-term outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethic approval for this study was obtained from the Ethic Committee of Xuzhou Central Hospital, Approval Number: XZXY-LJ-20150121-011
Informed consent
Written informed consent was obtained from all subjects before the study.