
Abstract
Due to an imbalance between aggressive factors known as hydrochloric acid (HCl), pepsin, leukotrienes, refluxed bile, defensive factors and reactive oxygen species, the peptic ulcer is formed in the stomach and duodenum which mostly include the function of prostaglandins, mucus bicarbonate barrier, enzymatic antioxidants, and some growth factors. H. pylori infection remained one of the considerable causes of peptic ulcer as it caused hypochlorhydria and struck off the defense mechanism of the stomach. The nonsteroidal anti-inflammatory drugs (NSAIDs) and stress are the most prevailing causes of peptic ulcer disease. Lack of physical exercise, little rest and due to poor leisure cause the peptic ulcer disease. Candies, chocolate, coffee, cigarettes, stress, and alcohol are the cause of peptic ulceration and suppression of acid in the stomach due to the utilization of antacid medication. Most of the ancient medical practices in the traditional alternative medicinal system include Unani, Ayurveda, Siddha, Homeopathy, Naturopathy, Chinese customary medicine, African conventional medicine, and Native American medicine. Without a hostile effect, the rate of curing the disease is the significance of natural products research. Peptic ulcer disease is the widespread nature of peptic ulcer in all class of population, which mostly may be due to rapidly changing the food habits and stress, causing the imbalance between gastric offensive and defensive factors. Curcuma longa is the most effective plant for the cure of peptic ulcer. Curcuma longa has anti-inflammatory and antioxidant activity. Curcuma longa remarkably reduces the level of inflammatory mediator (IL1) and (TNF) which was increased during the formation of an ulcer. In the rhizome of Curcuma longa, yellow pigment is present and widely used for the treatment of ulcer and decrease the inflammatory response. Symptoms include abdominal pain after taking a meal, nausea, vomiting, Anorexia and lose weight.
Keywords
Introduction
A peptic ulcer is a gastrointestinal disease and most chronic disease. 1 Affecting a large number of people all over the world, it becomes a common world health problem and still a major cause of death. 2 The main etiology of peptic ulcer is equilibrium deficiency between aggressive gastric factors and mucosal defensive factors. Scratch area of duodenal mucosa and gastric mucosa is peptic ulcer which caused by gastric juice. 3 Stomach and first few centimeters of duodenum are most ordinary sites for the formation of an ulcer. The Interruption of the mucosa of duodenum and stomach continuously break off by the pepsin, gastric acid and some medication like non-steroidal anti-inflammatory drugs (NSAIDS) finally causing lesions. 4 Barry Marshal and Robin Warren firstly identified the H. pylori which cause the peptic ulcer in the late 20th century. 5 Barry Marshal and Robin Warren receive Nobel prize in 2005 6 for their discovery. About 50% of the population is affected by H. pylori globally, and in developing countries, it approaches round about 100% whereas the population in developed countries is 50% affected. The bacteria present with different outcomes like gastritis, gastric carcinoma and peptic ulcer where 70% of gastric ulcer and 90% of duodenal ulcers are caused as results of H. pylori infection. H. pylori is a normal flora of gastric slot but became pathogenic in two focused circumstances, firstly when the defense factors are compromised in the stomach due to dietary factor or medication is another cause and secondly due to ingestion of a virulent strain of H. pylori. There are two types of causes which include NSAIDs mainly to harm the gastric mucosa and duodenal mucosa. One cause is that drugs behave like a weak non-ionized acid, which enter the mucus layer and in the epithelial cells. The other harm is to decrease the ability of cyclo-oxygenase inhibitory enzyme, by reducing the intracellular concentration of prostaglandins. They maintain the probity of the gastroduodenal mucosa, and the blood flow intact due to their vasodilator effect and also energizing the secretion of bicarbonates and mucus. 7
Transmission
The first way of bacterial transmission is iatrogenic in which instrument such as endoscope comes in contact with person gastric mucosa which endoscope was used in infected person so contact from infected to healthy person spread. 8 Disinfection reduced the chance of infection.9,10 Physicians who don’t use gloves while examining patients are at risk of gastritis or infected. 11 The oro-fecal route is also important because this bacteria is isolated from feces of infected person. 12 Contamination of water from feces can cause a peptic ulcer. 13 In Africa women give premasticate food to infants which causes ulcer. It is not associated with sexually transmitted infection. 14 Aspiration of bacteria from vomitus can cause ulcer but not documented.
Symptoms of peptic ulcer
Symptoms of peptic ulcer include abnormal weight loss, abdominal pain, Anorexia, nausea, vomiting and stools containing blood. 15 If the patient has a duodenal ulcer, then pain usually occurs in the epigastrium before breakfast or night time and can be grateful after taking meal and acid-neutralizing agent. 15 Some patient has heart burn in the absence of esophagitis. 15 The ulcers which occur due to NSAIDs intake mostly are asymptomatic in which upper gastrointestinal bleeding may be a clinical diagnosis. 16 The frequent complications of the peptic ulcer are bleeding noted 50–170 per 100,000, in those people who are aged more than 60 years. 16 The gastric obstruction which occurs due to ulceration convinced fibrosis minimum and increased impression unrevealed malignant disease. 17
Diagnosis of peptic ulcer
The diagnosis of peptic ulcer done by endoscopy when the mucosa of stomach and duodenum break of 5mm diameter and intact with fibrin, if mucosa breakdown less than 5 mm than it is known as erosion. Mostly peptic ulcer can be single sometimes multiple peptic ulceration occurs. Peptic ulcer in duodenum occur in the bulb of duodenum, where the stomach material enter into the small intestine. 18 Mostly gastric ulcer occur on the side of lesser curvature, usually from pylorus to cardiac end. 18 If ulcer is from one part of duodenum than chances of diseases like Zollinger-Ellsion syndrome and Crohn’s disease increases. 19 Sometimes patient aged more than 55 years can’t be diagnosed by endoscopy and their treatment is done on the bases of positive peptic ulcer. 19
H. Pylori as gut pathogen and its virulence factors
Helicobacter pylori, a Gram negative spiral shaped, microaerophilic bacteria is considered the most common pathogen of gastrointestinal tract since its discovery. Barry Marshall in 1982 and Robin Warren in 1984 assumed special significance in scientific world for the first isolation of H. pylori from the stomach of human. At first the naming of bacterium began with Campylobacter pyloridis, later on declared that Helicobacter genus is the right place for it. Subsequently, the word coined to denote the bacterium was “Helicobacter pylori” from ancient Greek, meaning "spiral gate keeper”. The Helicobacter genus is classified into two lineages, gastric and non-gastric (enterohepatic), and consists of 20 recognized species but the one that specifies human and primates (Mouse, Mongolian gerbil, Guinea pig, Gnotobiotic piglet) as hosts is H. pylori.
H. pylori has specific ultra-structural characteristics that became the focal points for its introduction such as it is a Gram-negative, microaerophilic (for its survival necessarily demands less O2 (5-15%) and CO2 (5-10%) compared to ordinary air, slowly growing but highly mobile, spiral shaped or curved rod but under stressful condition like nutrient deficiency or antibiotic administration can transformed to coccoid that although is non-culturable but viable and can make the subject carrier and facilitate its adhesion to gastric mucosa. It ranges in size from 3 µm to 5.0 mm long with a diameter of about 0.5 µm to 1.0 mm. The presence of 4-6 sheathed lophotrichous unilateral polar flagella about 3 µm long and having membranous terminal bulb formed by two copolymerized flagellins FlaA and FlaB, is responsible for motility of all enterohepatic as well as gastric Helicobacter species. H. pylori is surrounded by double membrane; inner membrane chemically composed of peptidoglycan, the periplasm, and the outer membrane is formed by variety of substances including cholesterol glucosides, phospholipids and LPS. The bacterial genes encodes five families of proteins associated with outer membrane, of which most important family has 21 Hop and 12 Hor outer membrane proteins that contains adhesins and other families comprises iron transporters, porins, flagella-associated proteins and proteins of unknown function.
Along with motility and adhesion characteristic enzymes production is an obligatory component for H. pylori nourishment and terrific virulence and on the other hand these enzymes possess toxic (phospholipases and alcohol dehydrogenase), antioxidant (catalase and superoxide dismutase), proteolytic and metabolic (phosphatases and ATPases) activities that are proven to be necessary for its survival in gastric acidic slot. H. Pylori virulence factors which facilitate it’s colonization in gastric environment like flagella, blood-group-antigen-binding adhesion (BabA) and urease; enzymes for pathogen survival including NADPH oxidase 1 (Nox1), alcohol dehydrogenase, catalase, phospholipase A, superoxide dismutase; along with inflammation in infected tissue and damage by bacterial structures like Vac A, Cag A, duodenal ulcer promoting A (DupA), outer inflammatory protein A (OipA), Lewis x and y antigens, H. pylori neutrophil activation protein (HP-NAP), and lipopolysaccharides (LPS) are other H. pylori virulence components which made this microorganism a potential gut pathogen.
H. pylori genome
Being the commonest infectious agent worldwide, H. pylori are subjected to vigorous identification of genome and up to 2013 the data submitted to GeneBank consists of complete genomes and draft genome sequences as 43 and 198, respectively. The first genome of H. pylori “26695” had 1.7 million base pairs and about 1550 genes were sequenced in August 1997, second complete genome “J99” in January 1999 and third complete genome “HPAG1” in June 2006 from gastritis patient in the UK, patient of duodenal ulcer in the USA and that of chronic atrophic gastritis in Sweden, respectively. The estimated H. pylori genome average size is 1.62 Mb with a 38.92% GC content. It is predicted that the average H. pylori genome possess 1590 open-reading frames that encode proteins 1532. Among all about 29% of loci are associated with pathogenesis containing the cagA gene and vacA gene. Approximately 6% of nucleotides are different among sequenced strains that represent a large genetic variation. The genomic survey is imperative in understanding the pathogenesis and especially enigmatic divergence of H. pylori also the ancestral relationships among various populations. 20
Pathogenesis of H. Pylori associated Peptic Ulcer
H. pylori possesses characteristics to adapt a critical gastric environment and cause tissue injury to cope up host immune response and persists in stomach for long time which other microbes cannot. Two types of factors are blamed for virulence of H. pylori; factors responsible for colonization (urease, flagella, adherence) as well as factors that cause injury to tissue (LPS, leukocyte enrollment, activating factors, Vac A & Cag A). Once the bacterium gains entry in the gastric acidic niche it shows chemotactic movement by using its flagella towards existing urea and bicarbonates on the gastric mucosal surface. For its temporary existence it immediately produces urease enzyme to make the surroundings alkaline by converting urea in to ammonia and CO2. Also the spiral shape of bacteria allows zigzag movement to facilitate colonization and penetration across thick mucus layer, epithelial cell surface and inter-cellular junctions only 20% remain adherent over cell. The pH varies among surfaces of mucosa as 2 on luminal and 5–6 on epithelial surface. H. pylori prefers to stay in the epithelial layer of mucosa as pH is slightly alkaline here. The tlpB gene encodes a specific chemoreceptor helps in swimming and avoiding acidic regions. The autotransporter proteins (BabA, SabA, AlpA, AlpB, HopZ, and OipA) are responsible for adhesion of H. pylori on the surface of epithelial cells. The adhesin protein “SabA” induces inflammation that causes epithelial cell damage and derivation of nutrients from damaged cells for H. pylori.
Cytotoxic associated gene (Cag-A) is also the potent virulence factor incorporated by type-4 secretion system (T4SS) in to host cell to expose apical cell surface to facilitate multiplication of pathogen and provision of nutrition. The bacteria elicit a cell mediated immune response by stimulating the generation of T helper 1 (Th1) expressed by H. pylori interrupts signaling of toll-like receptor 4 (TLR4) an innate immune receptor. Other mechanisms of bacteria for initiation of immune response include presence of flagella, an innate immune receptor TLR5 recognized part, that provoke a slight immune response by altered recognition site of N-terminal TLR5. The adaptations of bacterial membrane also plays a part in enhancing antigenic property of H. pylori by addition of cholesterol in membrane along with its glycosylated effects and the coating of membrane by host molecules that is plasminogen. 21
H. pylori possesses potent virulence factors such as Vacuolating cytotoxin (Vac A), which aimed at directly hitting the host immune cells to stimulate immune system. Vac A can induce apoptosis or disrupt phagosomal maturation 22 to reduce the functional ability of macrophages and is responsible for inhibition of proliferation of B-cells and CD8+ cells 23 also blocks T-cell proliferation of CD4+ cells 24 via hindrance of nuclear transcription of NFAT. The functions of T-cells are also affected negatively by bacterial arginase and γ-glutamyl transferase that in turn causes decline in the expression of inducible nitric oxide synthase. 25
H. pylori infection is seated in the roots of majority cases of gastritis. About 80% of patients diagnosed with gastritis have H. pylori isolated from their antral biopsies. Gastritis is a state of hypochlorhydria (reduced HCl) that appear as momentary, vague, dyspepsia like symptoms including nausea, vomiting and gastric overload. If having unbroken secretion of acid H. pylori migrates to antral region and results in antrum-predominant gastritis. Whereas in cases of reduced acid secretion corpus remains the mainstay of inflammation and condition is denoted as corpus predominant pangastritis as represented in Table 1 H. pylori associated digestive and extra-digestive disorders. 26 The inflammation gradually upgraded to atrophic gastritis, intestinal metaplasia and ultimately gastric carcinoma. 26 Gastric carcinoma is a neoplastic state of stomach illustrated by uncontrolled proliferation of gastric epithelial cells. It is a disease of high mortality with survival rates of 65% in early stage diagnosed patients and 15% in those diagnosed at a later stage. H. pylori are responsible for the basic pathogenesis of gastric cancer and are justified by the nomination of H. pylori as class one carcinogen according to the International agency for research on cancer (IARC). Surprisingly, despite the high prevalence of H. pylori in Africa and South Asia the incidence of gastric carcinoma is low and known as African and Asian enigma, the possible reasons behind are our lifestyle, food type and genotype of bacterial strain and host as well. 27
H. pylori associated digestive and extra-digestive disorders.

Non-Infectious reasons for peptic ulcers
Some ecological factors which also cause the peptic ulcer are known such as smoking, large intake of alcohol and some drugs uses, but Non-steroidal anti-inflammatory drugs (NSAIDs) are one of them which are more known ulcerogenic agent, some psychological disorder like depression and stress are important factor which increases the pathogenesis of ulcer. 28
NSAIDs specifically damage the mucosa of gastroduodenal by inhibiting the prostaglandin synthesis through the inhibition of cyclooxygenase-1 (COX-1) which leads to low blood flow towards mucosa, decrease the secretion of mucus and bicarbonate, and halt the proliferation of cell. The inhibition of enzymes is reversible which directly related to NSAIDs concentration ingested. It was also reported that NSAIDs associated peptic ulcers could be decreased by co-administration of exogenous prostaglandins and cyclooxygenase-2 (COX-2) 29 and further the gastric ulcers inducing toxicity also depend upon physicochemical characteristics of NSAIDs used. 30 After ingestion of NSAIDs in acidic environment they became protonated at very low pH (pH 2) and then cross the plasma membrane of gastric cells. On entering into epithelial cells at slight alkaline pH (pH 7.4) H+ ions are released which potentially target to mucus phospholipids and lead to the uncoupling of mitochondrial oxidative phosphorylation, thus initiating mucosal damage. Further, ionized drugs entrapped in gastric epithelial cells which damage organelles lipids membrane, destroyed mitochondrial activities, reduced energy production, enhanced permeability of cells, as well as decreased cellular survival. Old age patients with gastric ulceration or hemorrhage history along with using multiple drugs both steroids and NSAID or anticoagulants enhanced the risk of peptic ulcers development. 31 A new study on the animals shows that on gastric mucosa neutrophils circumference and they play a critical role for helping the NSAID injuries. 32 On the gastric mucosa neutrophil circumference and they damage the mucosa by generating the oxygen free radicals, liberate the proteases enzyme and impediment the blood flow. Neutrophil circumference difference also increases the capacity of NSAIDs which damage the mucosa of the stomach. During this process, Nitric oxide (NO) and hydrogen sulfide (H2S) release and they minimize the neutrophil circumference and normalized blood flow and mucus secretion. According to value if ulcer bleed approximately 1.79% volume then it known as H-pylori cause and bleeding occur 4.85% then it may be NSAIDs cause, and if ulcer bleeding occur approximately 6.13% then H-pylori and NSAIDs both are positive. 33
One of the most ulcerogenic factors which cause peptic ulcer known as the gastric ulcer is gastric acid, approximately 50% patient of stomach ulcer also cause ulcer due to over secretion of acid and pepsin. 34 Normally gastric acid secretion is the known defense particle for stomach; they play an important role to stop the bacteria for their entrance into stomach on the mucosal line if bacteria enter into the stomach then gastric acid inhibit them from forming their colonies. 35 Gastrin, acetylcholine, and histamine are three main factors for the motivation of gastric acid, histamine deliver from mast cells by help of H2 receptors, acetylcholine also deliver from vagus nerve, when bacteria inter into the gastric mucosa then these inflammatory mediators react on bacterial antigen cause inflammation and pathogenesis start in gastric mucosa and ulceration to occur. 36
Diagnostic techniques for H. pylori
H. pylori can be diagnosed by using various invasive and non-invasive techniques. Choice of the test depends largely upon availability, cost-effectiveness, clinical circumstances, and prevalence of infection in the particular region. Histological examination, culture, gram staining, rapid urease test and polymerase chain reaction (PCR) are molecular techniques for the detection of H. pylori depends upon endoscopic biopsy. Usually, biopsies are taken from antrum, but the body of the stomach may be focused for such purpose. Non-invasive tests such as UBT, H. pylori stool antigen, serology for H. pylori, ELISA IgG CagA are usually performed to detect urease activity, antibodies and bacterial antigens. Additional tests include pepsinogen ratio, anti-parietal cell antibodies and gastrin levels. 37
Epidemiology of H. pylori
A study conducted in Pakistan indicated that age increment, worse socio-economic and education status of the parents play a part in H. pylori sero-positivity. The major focus for risk factors of H. pylori are poor hygienic conditions and host genetic makeup and in Table 2 some alterable and unalterable risk factors of H. pylori infection has been summarized. Also the pets keeping is considered due to isolation of bacterium from stomach of house hold animals. 38
Alterable and unalterable risk factors of H. pylori.

Although scientists remain successful in detecting H. pylori from saliva, vomitus, gastric refluxate and feces 39 yet the authenticity for the route of transmission of H. pylori is scanty but those assumed to be the important one is horizontal transmission from one to other person via fecal to oral, mouth to mouth, gastro-oral route as vomiting and regurgitation is common in sufferers, the second is intrafamilial. 40
Global prevalence of H. pylori
The residents of developing countries are almost completely affected by H. pylori compared to half of the population of developed countries. 41 In developed countries almost 50% people aged more than 60 years and 10% of ages between 18 and 30 years are found infected with H. pylori. In United Kingdom 26% under 18–70 years age. 42
H. pylori prevalence in Asia
According to the Asia
H. pylori prevalence in Pakistan
There is no sufficient data available regarding prevalence of H. pylori in Pakistan. The reason is unavailability, high costs and troublesome invasive techniques of diagnosis. In Pakistan non invasive techniques revealed that 72.3% healthy children possess H. pylori in their stomach with negligible gender difference as 70.3% and 74.0% in girls and boys, respectively. Recent data revealed that in 1–15 and 15–65 years of age 47 and 92% of population in Pakistan is H. pylori positive, respectively. 45
Treatment strategies for H. pylori
For management of H. pylori induced anomalies the emphasis turns towards the strategies to alleviate H. pylori for successful rehabilitation of patient.
Standard therapies for H. pylori eradication
Various treatment options have been designed but there is not a single drug treatment suggested to overcome H. pylori infection rather combination of drugs are suggested that include proton pump inhibitors (PPI), bismuth salts and importantly antibiotics. 46 Multiple choices of antibiotics are prescribed with variable eradication efficacy and tolerance such as Clarithromycin, Amoxicillin, Metronidazole, Tetracycline, Fluoroquinolones, Tinidazole etc. Based on the low and high clarithromycin resistance areas, three lines of treatment of H. pylori has been determined with multiple choices of drugs combinations such as: first line of treatment, second line of treatment and third line of treatment (Table 3). 47
H. pylori eradication plan in standard therapies.
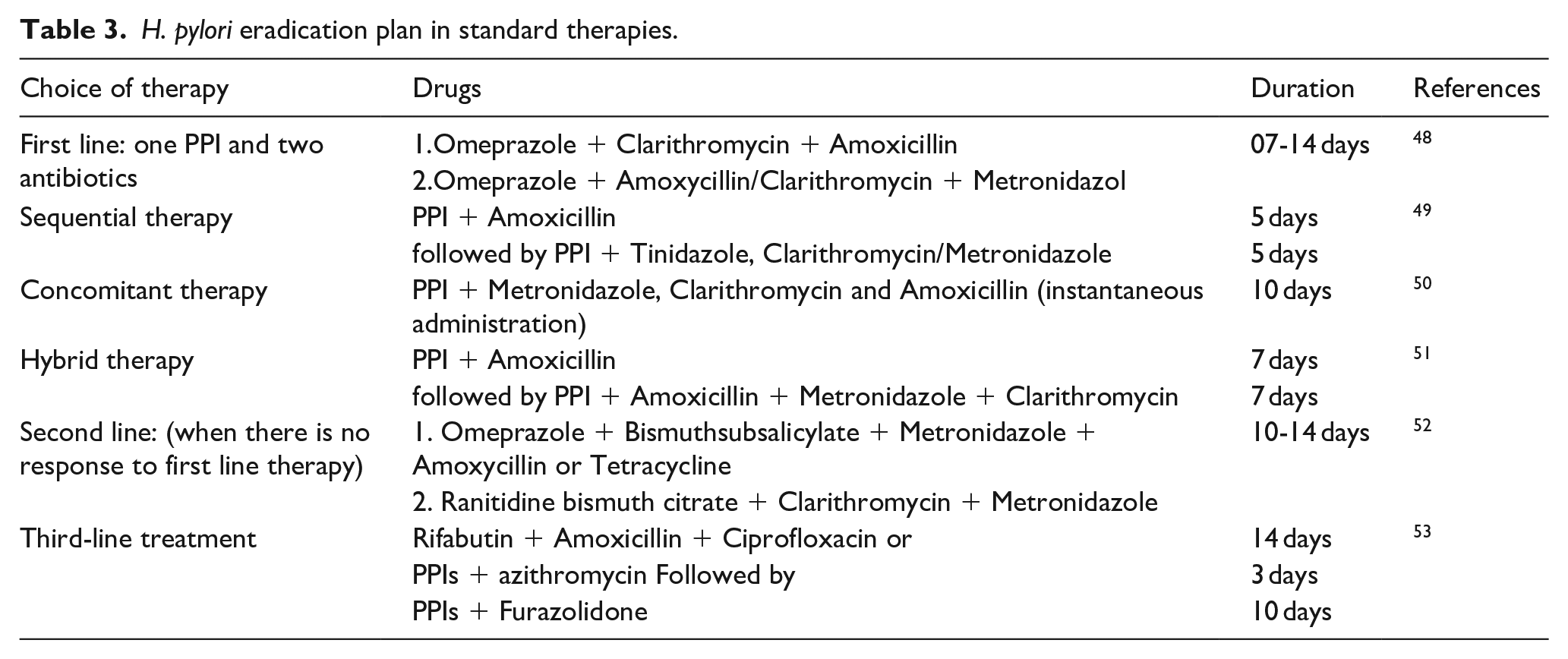
Clarithromycin is considered the most vulnerable drug to induce resistance in H. pylori followed by Metronidazole whereas Amoxicillin resistance is constant. The resistance rate should not exceed 20%. 54
Bismuth-based treatments were taken a gander at in extraordinary detail this year both as primary and second-line treatment. An exceptionally huge investigation from the European Registry on the Management of H. pylori contamination (Hp-EuReg) found that 1141 patients rewarded with first-line triple treatment in addition to bismuth accomplished a 88% fix. 50 An investigation of 101 treatment innocent patients in China accepting likewise a fourfold routine with bismuth brought about a fix 88% of the time. 55 Two examinations took a gander at the “single triple” case routine where bismuth and two anti-infection agents are given in a similar container, alongside a PPI. In the first of these from China, 192 patients got treatment with bismuth, metronidazole, and antibiotic medication and were contrasted with another gathering of 192 patients who got bismuth, amoxicillin, and clarithromycin given independently. 56 PPI was given independently in the two arms. No huge contrast between the annihilation rates was accomplished by the two regimens (86% versus 87%). In Italy, where successive treatment and bismuth-based fourfold treatment are the suggested first-line medicines, an investigation of right around 500 patients contrasted the Pylera® single triple container and consecutive treatment and again discovered comparable adequacy with destruction accomplished in 91% and 92%, individually. 57 Once more, considering obstruction, two other fascinating examinations rose up out of China. The first took a gander at a fourfold routine with bismuth and furazolidone and found a fix pace of 87%. 58 The second, from an area of high obstruction, thought about various regimens comprising of fluctuating dosages of rabeprazole with bismuth, amoxicillin, and either clarithromycin or antibiotic medication and discovered all to get annihilation rates in the district of 86% to 88%. 59 In Iran, another investigation of first-line patients with duodenal ulcer demonstrated identical destruction rates for bismuth fourfold treatment whether amoxicillin or antibiotic medication was utilized. 60 On account of penicillin-allergic patients, an examination from China detailed a destruction pace of 85% for patients getting bismuth, esomeprazole, clarithromycin, and metronidazole contrasted with 64% for those accepting anti-microbials without bismuth. 61
Two down to earth real-world contemplates were completed in Italy and Spain taking a gander at the utilization of bismuth-based fourfold treatment in day-to-day clinical practice. These are summed up in Table 4. 62
Real-world studies of bismuth-based quadruple regimens.

Two separate meta-analyses distributed in the most recent year inspected the job of bismuth-based treatment. One found that a 10-day treatment with Pylera® accomplished a powerful destruction pace of 90% both in first- and second-line treatment, paying little heed to the sort and portion of the PPI, in patients with clarithromycin- or metronidazole-resistant strains, and in those recently rewarded with clarithromycin. 63 Another meta-analysis which had more non-English language distributions announced a pooled destruction pace of 86%. In spite of the fact that bismuth-based regimens have for the most part been 10 days long, one examination on a 7-day bismuth-based treatment as second-line indicated extremely high annihilation paces of 94% contrasted with 74% for 14 days of moxifloxacin-based treatment. 64
Despite the fact that bismuth is an effective treatment for H pylori, disappointments and unfavorable occasions do happen. A multivariate examination acted in Korea taking a gander at consistence, treatment length, age >60 years, least inhibitory fixations for metronidazole and antibiotic medication, antagonistic occasions, and some other boundaries related with treatment disappointment, saw metronidazole opposition as the main free hazard factor for annihilation disappointment.
Besides the availability of an efficacious eradication therapy, relapses frequently come to report. Drugs used for the eradication of bacteria has various moderate to severe side effects on patient that make their use more difficult (Table 5). 53
Side effects of standard therapy for H. pylori eradication.

Phyto-therapeutic modalities as Alternative therapies for H. pylori eradication
In the light of above drastic side effects of antibiotic therapy there is urgent need to introduce alternate therapeutic modalities to combat with H. pylori. Probiotics are one among such alternative strategies such as Lactobacillus reuteri are found as competitors of H. pylori in adhesion to epithelial cells and also produce antimicrobial molecules. However, therapeutic drugs from natural resources are the primary choice to eradicate the H. pylori with high efficacy, safety and easily available both in cost as well as in concentration sense. In this scenario studies were performed to evaluate medicinal herbs and reported that medicinal plants possessing excellent anti-H. pylori activity include Mallotus Philippinensis, Curcuma longa, Glycyrrhiza glabra, Zingiber officinale, Matricaria chamomilla.65,66 Although, more detailed studies are required to explore the exact mechanism of phytochemicals to cure H. pylori related conditions but some researches revealed following mechanisms of action to eradicate H. pylori associated peptic ulcers.
Mechanism of actions of phytotherapeutic modalities
It was well reported that medicinal plants contained a wide range of phytoconstituents which could act as immunomodulators, antioxidant compounds, boost body oxidant status, as nutraceuticals, inhibit microbial adhesion as well as halt the proliferation or multiplication of microorganisms and some might act as microcidals by damaging the enzymes, membranes, DNA etc. These beneficiary properties of herbs are due to the presence of various phytochemical constituents like Alkaloids, Flavonoids, Phenolic compounds, Saponins, Glycosides, Steroids, Sterols, Tannins, Terpenoids, Triterpenoids, Phytosterols, Hydrocarbons, Mono and sesquiterpenes, Anthraquinone, Phlobatannins and many other plant secondary metabolites. Different parts like leaves, seeds, flowers, fruit, stems, bark, and in sometimes entire plant as medicinal modalities were used to treat microbes including H. pylori and these parts or their extracts are consumed orally as sole preparation or might be mixed with different other foods or drinks like water, honey, milk, juices and black pepper etc. The dose of the herbs preparations also depends upon sex, age and current health status of patients. 67
Prevention of H. pylori Adhesion
It was reported that fresh parsley, turmeric and borage water extracts had ability to prevent the attachment of H. pylori 11637 to the stomach of human; further inhibitory potential of these extracts was also reported on Lewis a and Lewis b antigens which range from 33.9% to 61.9%. 68 Anti H. pylori adhesion activity of Glycyrrhiza glabra root aqueous extract and polysaccharides was reported on using fluorescent microscopy technique on human stomach. 69 Pelargonium sidoides DC (Geraniaceae) was available with different trade names which have significantly high anti-adhesive activity. Studies revealed that root extract anti-adhesive activities are directly related to the dose consumed (0.001–10 mg/mL). 70 A Thailand based tree known as Plau-noi tree (Croton sublyratus Kurz) was studied. The results of leaves extracts explored anti-adhesion activity against H. pylori evaluated by using adenocarcinoma cells and further it was also reported that it suppresses the secretion of IL-8 in a dose-dependent manner. 71
Urease as therapeutic target
As H. pylori infection manifested by high production of urease enzymes so it was reported that many medicinal plants specifically inhibit the urease activity to cure this infection. Acacia nilotica and Calotropis procera are used as anti-H. pylori drugs and reported that their extracts competitively inhibit the urease activity and some mixed type mechanisms, respectively. 72 Paeonia lactiflora roots extract contained 1,2,3,4,6-penta-O-galloyl-β-D-glucopyranose which destroyed H. pylori by damaging cell membrane, inhibit UreB (an adhesin) membrane as well as inhibit the activity of urease enzyme. Further, animal based study explored that stem bark extracts of Calophyllum brasiliense in different solvents possessed anti-urease activity and ultimately decreased the H. pylori burden confirmed by histopathological examination of Wister rats. 73
Reactive oxygen species and oxidative stress
Impatiens balsamina L. extract contained 2-Methoxy-1,4-naphthoquinone (MeONQ) which demonstrated high bactericidal activities to treat multiple resistant H. pylori. 74 MeONQ has high redox potential which have the ability to penetrate cell membrane and in cytosol flavoenzymes metabolized these compounds through serial redox cyclic reactions to produce a high amount of reactive oxygen species like O-•, MeONQ-•, and H2O2. Those ROS reacted with the macromolecules of cell to damage them and leaded the death of H. pylori. 75
Amphipathic behavior of phytocompounds
Secondary metabolite from Sclerocarya birrea (Anacardiaceae) as terpinen-4-ol has amphipathic nature and this type of nature overcome the H. pylori resistance towards treating drugs. The hydrophilic properties of such phytoconstituents facilitate the diffusion of molecules to reach the bacterial cell wall and the hydrophobic properties facilitate the compounds binding with cell membrane to damage membrane integrity. 76
DNA damage and other mechanisms
Glabridin is a major flavonoid of medicinal plants which possessed potentially significant role in the inhibition of DNA gyrase and dihydrofolate reductase to control H. pylori infection. 77 Similarly, Emodin (1,3,8-trihydroxy-6-methylanthraquinone) present in Chinese herbal medicine also damage the H. pylori DNA. 78 Piper carpunya Ruiz & Pav contained a number of flavonoids like vitexin, isovitexin, isoembigenin and rhamnopyranosyl vitexin which have H. pylori destroying activity. These compounds have inhibitory effect on H+,K+ ATPase and stimulate the myeloperoxidase release from rat peritoneal leukocytes. 79 N-Acetylation, a major metabolic pathway for arylamine carcinogens, is catalyzed by cytosolic arylamine N-acetyltransferase. Rhein, one of the bioactive components of Dahuang, effectively inhibited N-acetyltransferase activity and H. pylori growth. 80
Medicinal Plants having Anti-H. pylori potential
Curcuma longa
Curcuma longa commonly known as turmeric, and it is obtained from the plant rhizomes. It is used for the treatment of peptic ulcer in drug form. Turmeric belongs to Zingiberaceae family, and it is cultivated in all South Asia. Curcuma longa has other properties like antioxidant and anti-inflammatory. 81 Turmeric has three main constituents like bisdemethoxycurcumin, demethoxycurcumin and diferuloylmethane (curcumin), some other constituents are known as resins, proteins, atlantone and tumerone. 82 Ronita De et al. conducted a clinical trial and found that Curcuma longa had a best medicinal effect and used orally and intravenously (iv). Curcuma longa is a more effective drug for peptic ulcer disease, most beneficial effect for H-pylori infection. Curcuma longa was given intravenously for 7 days at a dose of 50 ng/kg in vivo experiment. After 7 days H-pylori was checked by urease test, Curcumin eliminates the H. pylori infection from the gastric mucosa, it also breaks the colonies which formed by bacteria in gastric mucosa. 83
Foeniculum vulgare
Foeniculum vulgare is a potential source of potassium, sodium, phosphorus, and calcium. It contains neophytadiene (0–10.6%), exo-fenchyl acetate (0.3–3.8%), (E)-phytol (0.1–6.0%), estragole (0.1–2.5%) and fenchone (0.1–3.1%). Hydroethanolic extract of F. vulgare has shown in a study the inhibition of H. pylori and C. jejuni.84,85 A study assessed Fennel essential oil for antimicrobial activity using disk diffusion method and revealed inhibition of Bacillus cereus, B. magaterium, B. pumilus, B. substilis, E. coli, K. pneumonia, M. lutus, Pseudomonos pup-ida, P. syringae, and C. albicans. 86
Trachyspermum ammi
Trachyspermum ammi has found to constitute chemical compounds such as carbohydrates, saponins, glycosides, volatile oil, phenolic compounds, fiber, protein, fat, and mineral matter for example calcium, iron, phosphorous and nicotinic acid. T. ammi was investigated by Hussein et al. 87 and found its methanol extracts showed significant in vitro inhibitory effect on hepatitis C virus (HCV) protease at a concentration of 100 μg/ml. More over Gurinder and Daljit 88 reported remarkable antibacterial activity of acetone and aqueous extracts of T. ammi against Enterococcus faecalis, K. pneumonia, P. aeruginosa, Salmonella typhimurium, Shigella flexneri S. aureus, E. coli, and S. typhi. An in vitro study conducted on Hepatitis C virus proved the antiprotease activity at 100 µg/ml dose. 89 T. ammi is also proven to possess gastroprotective efficacy by exhibiting bactericidal activity for different H. pylori strains. 90
Mentha piperita
Mentha piperita is rich source of iron and magnesium, which play important role in human nutrition 91 and menthol is prescribed as a medication for gastrointestinal disorders, common cold and musculoskeletal pain. 92 Krzyzanowska et al. (2011) 93 reported the existence of cineole (3.5–14.0%), limonene (1.0–5.0%), menthone (14.0-32.0%), isomenthone (1.5–10.0%), menthofuran (1.0–9.0%), menthyl acetate (2.8–10.0%), menthol (30.0–55.0%), isopulegol (max. 0.2%), pulegone (max. 4.0%) and carvone (max. 1.0%) in mentha plant. A study conducted by Kaur and Arora (2010) 89 investigated the existence of flavanoids and tannins in the methanolic extract of mint leaf. A relationship has been suggested among the phytochemicals like tannins and flavanoids as well as the free radical scavenging activity and bactericidal activity of the extract adjacent to the test organisms and given as 3.125 and 6.25 μg/ml, respectively. Investigation of antimicrobial, antioxidant and anti-inflammatory activities of Peppermint and Chocolate mint oil was performed using broth dilution method and MICs determined were significant for Pepper mint that is 0.15, 0.08, 0.92 (% v/v) against E. coli, S. aureus and P. aeruginosa, respectively whereas anti-inflammatory and antioxidant activities were stronger in Chocolate mint oil. 94
Metricaria chamomilla
Metricarea chamomilla was assessed by various studies previously and found to possess antibacterial activities due to the presence of α-bisabolol and cyclic ethers. Umbelliferone contributes in fungal inhibition and Chamazulene and α-bisabolol are responsible for antiseptic properties, it also possesses potent antileishmanial activity. 95 In another study the aqueous and methanolic extracts of Chamomile showed differential apoptosis in cancer cells but not in normal cells at similar doses. 96 Martins et al.97,98 and Nayak et al. 99 conducted an in vivo study and stated that extract of M. chamomilla administered topically has wound healing potential in linear incisional wound model in rats. Animals treated with Chamomile presented significantly faster wound healing in comparison to those treated with corticosteroids. Further studies revealed that methanol extracts of M. chamomilla (flowers) and Ginkgo biloba (leaves) had an MIC > 100 µg/mL against the Gram-negative bacterium H. pylori. 84 The chemical constitutents thought to be responsible for such activities of Chamomile are sesquiterpene derivatives (75–90 %), monoterpenes (20%), polyynes, essential oil contains (E)-β-farnesene (4.9–8.1%), terpene alcohol (farnesol), chamazulene (2.3–10.9%), α-bisabolol (4.8–11.3%), and α-bisabolol oxides A (25.5–28.7%) and α-bisabolol oxides B (12.2–30.9%).
According to Ines et al. 100 Viola odorata contains alkaloid, glycoside, vitamin C, saponins, mucilage and monoterepenes and sesquiterpene, 1-phenyl butanone, linalool, benzyl alcohol, methyl salicylate, α-cadinol, globulol, viridiflorol, Pulegone, epi-α-cadinol, terpinen-4-ol, germacrene A and paramethyl anisole. Study evaluated the activity of V. odorata against Haemophilus influenza, P. aeruginosa, S.aureus, S. pneumoniae and S. pyogenes by using agar well diffusion method and show significant MICs. 101
A study was conducted 77 to investigate the gastroprotective effects of some plants reported that extracts obtained from Iberis amara, Matricaria recutita, Melissa officinalis, Carum carvi, Glycyrrhiza glabra, Mentha x piperita, Angelica archangelica, Chelidonium majus and Silybum marianum separately and combined in the form of a compound drug commercial preparation, STW 5 (Iberogast) produced anti-ulcerogenic activity that is dependent upon dose is linked with a decreased acid output and an enhanced mucin secretion, an ascend in prostaglandin E2 release and a decend in leukotrienes. A previous study 102 described anti H. pylori activity of seeds of Myristica fragrans, rhizome of Zingiber officinale and leaves of Rosmarinus officinalis (rosemary). A study conducted by Mahady et al. 84 reported that Foeniculum vulgare, Achillea millefolium, Passiflora incarnata, Origanum majorana possess moderate H. pylori inhibitory activity where as weak activity was seen in Carum carvi, Elettaria cardamomum, Gentiana lutea, Juniper communis, Lavandula angustifolia, Melissa officinalis, Mentha piperita, Pimpinella anisum, Matricaria recutita and Ginkgo biloba.
Glycyrrhiza glabra
Glycyrrhiza glabra is a medicinal plant of Leguminosae family. It is used against different diseases, mainly show anti-ulcer activity. Mostly its roots and rhizomes are used for the production of medicine. The common name of Glycyrrhiza glabra is Liquorice. 103 The active constituent of licorice is glycyrrhizinic acid, glycyrrhizin and saponin. 104 Licorice plays a major role to inhibit the gastric ulcer disease, potassium and calcium salts are present in glycyrrhizinic acid; these salts also neutralize the acidity in the stomach. Glycyrrhizinic acid has free fractions glycyrrhizin, and these fractions interfere in gastric acid secretion, and these fractions are known as FM 100 fraction (40). Carbenoxolone and deglycyrrhiziniclicorice (DGL) is used for the treatment of ulcer, and these are the major component of the glycyrrhizinic acid while aspirin and cimetidine also damage the mucosa. 105
Silybum marianum
Silymarin containing a mixture of flavonolignans, derived from the extract of Silybum marianum, is most beneficial for the peptic ulcer disease. The main active component of silymarin is 4,5,7-trihydroxy–methoxy–flavanona-3-ol. Enzymatic oxidation is stopped by silymarin and it also limit the leukotrienes synthesis. If the levels of leukotrienes increase they crush the gastric mucosa and cause ulceration. In this way, silymarin slows down the level of leukotrienes. 106 Silymarin is administered orally and intravenously for the treatment of ulcer, but in this trial, silymarin was administered intragastrically. The maximum amount of 100 mg/kg is given intragastrically, and after 2 h silymarin starts their action against the inflammatory mediators like histamine and reduce the level of pepsin. When the inflammatory mediators stop their function, then inflammation became minimum and healing of ulcer occur, in this way silymarin play the most beneficial role for the gastric ulcer healing. 107
Limitations of the study
This review article has the limitation of being a general review rather than systemic or meta-analysis providing a general overview of peptic ulcer, its transmission, pathophysiology and mainly the treatment modalities focusing on the alternative medicinal system utilizing the natural plants bioactive constituents. Another limitation of the study is the limited data on the clinical trial evaluating the anti-H. pylori activity of plants phytoconstituents. Only limited number of plants with anti-H. pylori activities are discussed and there may be large number of plants enriched with bioactive compounds which have the potential to be used for the treatment of various types of ulcers including the H. pylori associated ulcer.
Conclusion
Herbal medicine has the most beneficial effect for the treatment of peptic ulcer; some allopathic drugs like NSAIDs proved crucial for gastric mucosa and caused ulceration in the stomach and duodenum. Clinical trial and their pharmacological action prove that peptic ulcer which becomes world health problem mainly cured by herbal medicine and this medicine has a significant global impact on health care delivery. Active constituents of Curcuma longa and licorice have the best potential against the inflammation caused by bacteria and another causative agent in gastric mucosa and the first part of the duodenum. These constituents have antiulcer activity and its safe option for management of peptic ulcer.
Footnotes
Acknowledgements
We acknowledge Dr Abid Rashid for providing us library facility. Authors are thankful to Government College University Faisalabad and the Higher Education Commission of Pakistan for providing the access to various data bases for literature search to accomplish this review article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.