
Abstract
Bacterial meningitis is a rare event in children with cochlear implants. A 7-year-old child who underwent cochlear implantation (CI) for the right ear 6 years ago was admitted to our hospital with the chief complaint of intermittent fever and headache for 6 months. Cochlear implant infection was suspected. The right cochlear implant removal and middle ear exploration were performed. Postoperatively, the bacterial cultures of cerebrospinal fluid (CSF), cochlear implant and inserting electrodes all suggested Pseudomonas aeruginosa. The body temperature of the child was controlled within 2 weeks after the operation by using meropenem, and other symptoms like headache and abdominal pain disappeared. During 20-month follow-up visit, the child did not suffer any discomforts. In conclusion, we reported a child who developed Pseudomonas aeruginosa meningitis following head injury after CI. This case should serve as a reminder for clinical doctors.
Introduction
Cochlear implantation (CI) is a safe and effective procedure to rehabilitate the patients with bilateral severe-to-profound hearing loss.1 –3 With the development of CI, the incidence of CI-related complications has been decreased to a relatively low level. However, a previous study showed an increased incidence of bacterial meningitis in children with cochlear implants; compared with the adults with cochlear implants, the children may be easier to develop bacterial meningitis. 4
To our knowledge, Streptococcus pneumoniae is the most common organism identified in the reported cases of meningitis. 5 Nevertheless, in this article, we reported a 7-year-old child who developed Pseudomonas aeruginosa meningitis following head injury after CI.
Case presentation
History and examination
A 7-year-old boy from China was admitted to our hospital with the chief complaint of intermittent fever and headache for 6 months. Six years ago, the child underwent CI for the right ear due to severe binaural sensorineural deafness and incomplete partition type I (IP-I) malformation. On the third day after the operation, he fell down from the bed and cerebrospinal fluid (CSF) otorrhea in the right ear occurred, so a repair of cerebrospinal otorrhea for the right ear was performed, and meanwhile positive measures for the CSF leak, such as packing with muscle and fascia, were also taken during the operation. One month after the operation, the cochlear implant was started up and its effect of assisting hearing was very good. After that, he had never suffered from any discomforts.
Six months ago, the child began to have fever and headache under no circumstances of conspicuous precipitating factors, accompanied by abdominal pain. The highest body temperature had exceeded 39°C. He had no symptoms of nausea, vomiting, convulsion, insomnia, otorrhea, retroauricular swelling and pain, dizziness, rotary vision, deviated mouth and abnormal facial sensation. After systematic examination in local hospital, Pseudomonas aeruginosa was found in CSF and shown sensitivity to meropenem. The above-mentioned symptoms got remission after intravenous injection of meropenem for about 2 weeks but reappeared within 2 weeks after stopping the drug. Such a condition lasted about half a year.
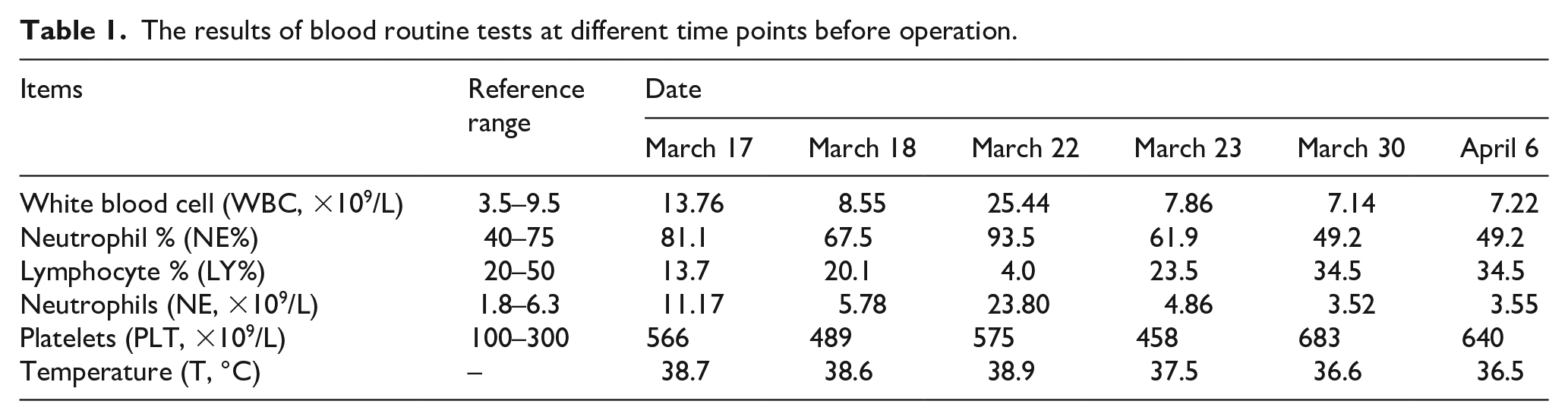
For the complete rehabilitation, the child came to our hospital. The physical examination showed positive meningeal irritation sign, negative Hoffmann sign and negative Babinski sign. The results of blood routine tests (Table 1), CSF examination (Table 2) and different-layer CT images (Figure 1(a)–(e)) supported Pseudomonas aeruginosa infection. The cochlear implant infection was suspected. The right cochlear implant removal and middle ear exploration were thus performed under general anesthesia on April 7, 2017 after the indicators of blood routine test and body temperature returned to normal.
The results of blood routine tests at different time points before operation.
The testing results of CSF samples obtained by lumbar puncture.


Different-layer CT images of the temporal bone in the child before the operation. (a) Bilateral IP-I malformations (the arrow represents the enlarged internal auditory canal); (b) CI in the right ear (the arrow represents the vestibular aqueduct); (c) presence of soft tissue density shadows in the middle ear tympanum and mastoid; (d) the electrode of electrical cochlea in the right cochlea; (e) presence of soft tissue shadows around the electrode.
Operation procedures
The mastoid was opened intraoperatively along the previous incision. It could be seen that the formation of mastoid new bones covered the original mastoid cavity. The mastoid new bones were partly grinded to make the mastoid cavity exposed, and the cochlear electrode wire was seen in the operative cavity. The implant was positioned along the electrode wire, and then the cochlear electrode wire was cut off near the facial nerve recess. The facial nerve recess was opened to expose the round window after implantation, reference electrode and gelatin sponge in the facial nerve recess were taken out. Finally, the connective tissue around the round window was removed, the inserting electrode was taken out, and the round window and mastoid were closed. The CSF obtained by lumbar puncture was colorless and transparent, and 5 mL was used for biochemical test and bacterial culture. Additionally, the cochlear implant and the inserting electrode were used for bacterial culture.
Postoperative condition
Postoperatively, the bacterial cultures of CSF, cochlear implant and inserting electrodes all suggested Pseudomonas aeruginosa. Cefepime and mannitol were used to control the symptoms. The body temperature of the child was decreased below 37.5°C within 2 weeks after the operation, and the symptoms, such as headache and abdominal pain, disappeared. CSF routine and biochemistry indicators returned to normal. During 20-month follow-up visit, the child did not suffer any discomforts, such as pain, swelling, rupture and purulence in the local skin, earache, headache, tinnitus, dizziness, facial paralysis, otorrhea, etc.
Regarding the future hearing reconstruction, it is almost impossible to successfully implant the cochlea on the same side to achieve the good hearing effect under the circumstances of no severe complications, thus the contralateral cochlear implantation will be taken into more consideration. If this method is not applicable, we will consider the auditory brainstem implant or updated techniques to reconstruct the hearing.
Discussion
Bacterial meningitis after CI may not only induce the facial nerve stimulation and cochlear ossification, but also put the children at risk of permanent hearing loss. 6 In this report, the child had bilateral IP-I malformations and suffered CSF otorrhea in the right ear after CI. IP-I malformation, also called cystic cochleovestibular malformation, is a rare malformation of the inner ear, characterized by a cystic featureless cochlea owing to complete absence of modiolus and interscalar septa. 7 The studies have demonstrated that inner ear malformations are associated with recurrent meningitis caused by CSF otorrhea which is very easy to put the patients at risk of bacterial meningitis.8 –10 Cohen et al. also found that the age (less than 2 years old and more than 65 years old), cochlear malformation complicated with CSF leakage and implants with a positioner were the risk factors for bacterial meningitis. 5
The positioner plays a pivotal role in the pathophysiological process of bacterial meningitis. It has two different silicon structures, which provide an unsealed passage for bacterial spread aggravated by the trauma due to the positioning in the scala tympani.5,11 However, in this report, the child with a cochlear implant without a positioner developed Pseudomonas aeruginosa meningitis, which suggested the occurrence of bacterial meningitis may be irrelevant to the positioner. A previous study showed that the highest bacterial meningitis occurred immediately after CI, and no cases of meningitis occurred more than 4 years after CI. 6 However, this report presented us that bacterial meningitis may occur even 6 years after CI.
Pseudomonas aeruginosa, a common cause of otitis externa, can spread to CSF space in a retrograde fashion through the abnormal communication between CSF space and inner, middle and external ears. Prompt diagnosis and intervention on the bacterial meningitis is conductive to alleviating the symptoms and preventing deleterious neurologic sequelae. 12 This report demonstrates that prompt removal of the right cochlear implant and treatment with antibiotics may prevent the bacteria from spreading to CSF space.
Conclusion
We reported a child who developed Pseudomonas aeruginosa meningitis following head injury after CI. This case should serve as a reminder for clinical doctors. When a child with a cochlear implant complains about intermittent fever and headache after a head injury, he may be at the risk of bacterial meningitis. Once diagnosed, intravenous antibiotics should be used immediately to control the symptoms, and surgical interventions may be required if necessary.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (No.: NFSC 81770993), Fundamental Research Funds for the Central Universities (No.: 2019-JYB-JS-052) and Beijing Natural Science Foundation (No.: 7194292).
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
We confirmed that we had obtained written informed consent from the legally authorized representative of the minor subject prior to study initiation and had obtained the necessary consent to publish patient information.