
Abstract
Epstein–Barr virus (EBV) belongs to a subfamily of herpesviruses, also known as human herpesvirus type 4. EBV is widely distributed in the population, with a high infection rate of 90%. EBV infects mainly B lymphocytes, stimulates cell proliferation and transformation and even causes cancer. In recent years, it has been found that it can also infect T lymphocytes, epithelial cells and natural killer (NK) cells and can cause related diseases. EBV infection can cause a variety of clinical symptoms and clinical manifestations, which brings some confusion to clinical diagnosis and easily leads to missed diagnosis and misdiagnosis. In this article, we report a case of EBV-induced severe abdominal and pelvic infection, which eventually led to death.
Introduction
Epstein–Barr virus (EBV), also known as human herpesvirus 4, can cause many symptoms, including, commonly, fever, lymphadenopathy and/or hepatosplenomegaly.1,2 EBV can also cause some unusual diseases, such as acute kidney injury and conjunctival tumours.3,4 Because of the diversity of clinical manifestations of EBV infection, early detection of atypical clinical manifestations caused by EBV infection is very important for judging the condition and prognosis. To date, no cases of abdominal and pelvic infections caused by EBV infection have been reported. Here, we present a case of EBV infection with abdominal-pelvic tissue involvement and the results of quantitative viral DNA determination in plasma and pelvic tissue suspension supernatant.
Case Report
A 20-year-old female was referred to our hospital because of weak abdominal pain and fever for 3 months. Three months prior, the patient was hospitalized in a local hospital and considered to have a "pelvic abscess". She underwent laparoscopic pelvic adhesiolysis under general anaesthesia, right salpingectomy, right ovarian biopsy and ring removal. The patient still had fever after the operation, and the body temperature fluctuated from 37.2°C to 39.5°C.
Past history
Three years prior, she was diagnosed with haemophagocytic syndrome in an external hospital, and she recovered after 3 months. Two years prior, she had an ectopic pregnancy and received conservative treatment (chemotherapy). She had no history of infectious diseases. On admission, the temperature was 39°C, the pulse rate was 80/min, and the blood pressure was 100/60 mmHg. The respiratory rate was 18/min. Flat abdominal and right lower abdomen and lower abdomen tenderness were present, and the remaining physical examination was negative. On abdomen computed tomography (CT) scan (Figure 1), a pelvic mass shadow was present, with possibly infectious lesions. Laboratory test results revealed that haemoglobin and platelet levels were normal at first. Gramme stain tests and bacterial cultures from blood were negative. Serological tests were negative for HIV, cytomegalovirus, measles, respiratory syncytial virus, influenza virus, Mycoplasma pneumoniae and Legionella pneumophila. Anti-nuclear antibody spectrum, neutrophil cytoplasmic antibody and cardiolipin antibody were all negative. The detection of EBV-DNA in serum by qualitative polymerase chain reaction (PCR) was 8.89 × 102 copies/mL initially and increased to 1.52 × 103 copies/mL after re-examination. EB-CA-IgG was 216.15 RU (reference range 0.00–22.00), and EB-CA-IgA was positive, with S/CO = 4.99. The patient was treated with a variety of antibiotics, but the patient still had repeated fever, abdominal pain, swelling and pain of the right lower extremity. Routine blood tests showed pancytopenia (leukocyte count 2.46 × 109/L, haemoglobin 7.5 g/L, platelet count 66 × 109/L). Laboratory test results revealed hypoimmunity and CD3+/CD4+ at 47.98 cells/μL (normal 414–1123), CD3+/CD8+ at 98.85 cells/μL (normal 238–874), natural killer (NK) cells at 74.28 (normal 90–590) cells/μL and CD19+ at 57 cells/μL (normal 90–660), which had obviously declined. Abdominal CT (Figure 2) showed inflammatory lesions beside the psoas major muscle, which was worse than before hospitalization. Therefore, another laparotomy exploration and parapsoas major mass resection was performed to remove the parapsoas major mass, which was approximately 4 cm in size. Postoperative pathology revealed a large amount of lymphocyte-like cell infiltration in some tissues (Figure 3). Tissue suspension PCR resulted in 7.54 × 105 (positive) copies/mL. Dexamethasone (10 mg) was given for 3 days, after which the patient was discharged automatically. The patient was finally diagnosed with EBV pelvic infection and haemophagocytic syndrome. The patient died 1 week after discharge.

The patient’s abdomen CT scan, showing a pelvic mass shadow.

Abdominal CT showing inflammatory lesions beside the psoas major muscle.
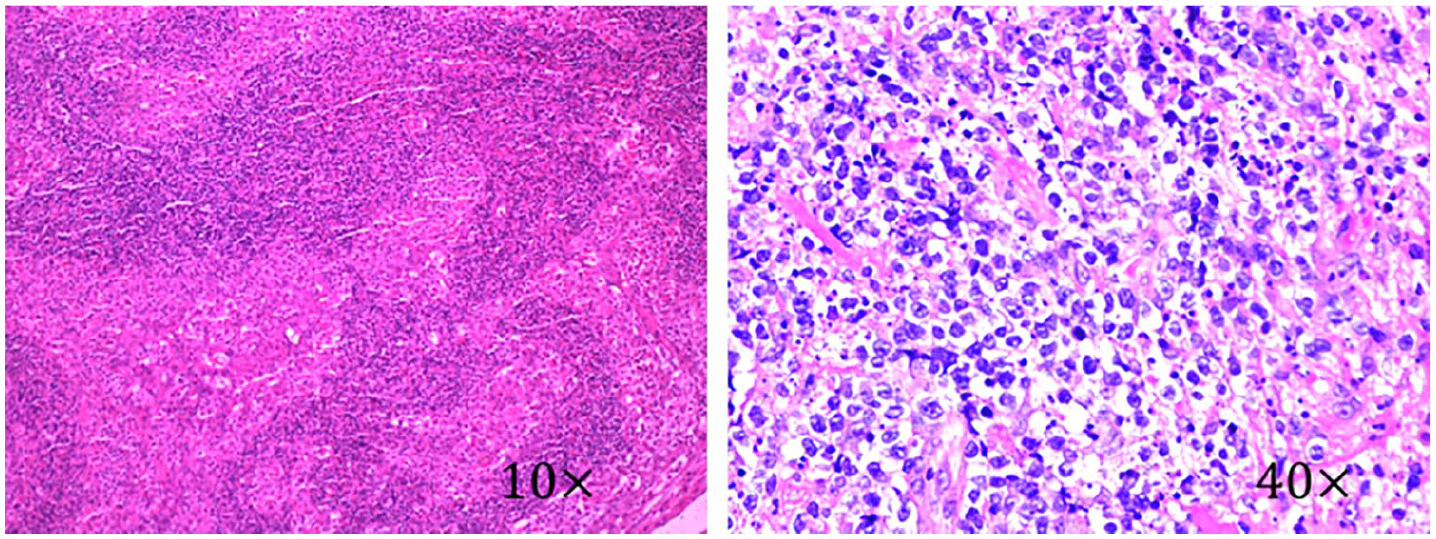
Pathological examination showed that there were many abnormal lymphocytes infiltrating the mass beside the psoas major muscle.
Discussion
EBV is a lymphotropic DNA virus that is transmitted mainly through saliva. EBV proliferates in the epithelial cells of the oropharynx and then infects B lymphocytes and concentrates in B lymphocytes. Once EBV infects B lymphocytes, it will incubate in the host for a long time, and the infected person will become a lifelong carrier of the virus. EBV infection is more common in adults than in children. More than 90% of adults have been infected. Children under 6 years of age experience mostly recessive or mild infections. People above 15 years of age are mostly infected with typical symptoms. After the onset of EBV infection, they can obtain lasting immunity. Most people have a good prognosis. A few people have a poor prognosis. They develop severe hepatitis, haemophagocytic syndrome, chronic infection and cancer, which endanger their lives.5,6 Infected cells entering the human blood circulation will cause systemic infection, which involves the respiratory, blood, nerve, immunity, kidney and heart systems and other multisystem and multiorgan conditions.1,2,7
Our patient presented with persistent high fever, right lower abdomen and right lower extremity pain and low immunity. The retroperitoneal soft tissue shadow on abdominal and pelvic CT scans suggested a high possibility of inflammation. The EB-DNA in the blood of the patients was positive and increased progressively. EB-DNA was positive in the suspension of the mass beside the psoas major muscle. In summary, the diagnosis of EBV infection was clear. However, there are rare reported cases of abdominal and pelvic infection caused by EBV in the past, which makes the diagnosis more difficult. The diagnosis was confirmed only when EB-DNA positivity was detected by PCR in the suspension of the abdominal resection. The evolving pancytopenia, hypofibrinaemia, fever, ferritin elevation and decreased NK activity suggested the presence of virus-associated haemophagocytic syndrome. Haemophagocytic syndrome can be divided into two types: primary and secondary. The pathogenesis of haemophagocytic syndrome has not been fully clarified. Most scholars believe that it is related to the genetic background and immune factors. The activity of NK cells in patients with EBV-associated haemophagocytosis is low or even lacking, which leads to severe immune deficiency of the infected body, inefficient EBV clearance, abnormal activation and proliferation of CD8+ T lymphocytes, and activation of macrophages, 8 resulting in the production and release of inflammatory cells, hypercytokinaemia, proliferation and phagocytosis of histiocyte body blood cells. Histopathology showed that lymphocytes and histiocytes proliferated and infiltrated in all organs. The results of histopathological examination in this case were consistent with those reported in the literature, showing many abnormal lymphocytes infiltrated in the tissues and cells proliferated in the sinuses of lymph nodes. There is no standard treatment for severe EBV infection. The treatment of EBV infection mostly adopts single or double antiviral therapy, but the treatment of chronic active EBV infection is difficult. 9 There is no unified and effective treatment, and the treatment is mostly temporary relief. The use of autologous or donor EBV-specific T cells or allogeneic haematopoietic stem cells to reconstruct immune therapy for this disease has been reported, but the risk of the disease is high, which causes a primary disease, recurrence and progression leading to death. 10
In the past several years, some patients who had chronic active Epstein-Barr virus infection (CAEBV) infection with infiltration of the skeletal muscle were reported.11–13 However, skeletal muscle involvement is still very rare. In our case, EBV infection can cause pelvic and abdominal inflammatory mass and psoas major oedema. Haemophagocytic syndrome manifestations can also occur. At the same time, there was evidence of EBV infection. The diagnosis of EBV-related haemophagocytic syndrome was established.
In recent years, EBV infection has been increasing annually, and clinical manifestations have diversified. Patients with repeated fever due to EBV infection should be vigilantly followed in the clinic. Quantification of EBV-DNA in plasma by real-time PCR has been suggested for monitoring patients at risk of EBV-associated lymphoproliferation. 14 In our patient, the plasma EBV-DNA levels were always high.
This result is consistent with the patient's persistent fever, right lower abdominal pain and right lower extremity pain.
Conclusion
EBV infection is often characterized by increased monocyte counts, but fatal hemophagocytic syndrome, pneumonia and so on also occur from time to time. In this case, even abdominal and pelvic infection and psoas major oedema occurred. This clinical manifestation is very rare and may be related to the patient's low immunity, pelvic operation history and ectopic pregnancy operation history.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from the Medical Ethics Committee of Fu Xing Hospital, Capital Medical University (approval number/id 2019FXHEC-KY018).
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the subject’s legally authorized representatives.