
Abstract
This study investigated associations between inflammatory markers, sickness behaviour, health anxiety and self-rated health in 311 consecutive primary care patients. Poor self-rated health was associated with high sickness behaviour (ρ = 0.28, P < 0.001; ρ = 0.42, P = 0.003) and high health anxiety (ρ = 0.31, P < 0.001; ρ = –0.32, P = 0.003). High levels of interleukin 6 were associated with poor self-rated health in men (ρ = 0.26, P = 0.009). Low levels of interleukin-6 were associated with poor self-rated health in women (ρ = –0.15, P = 0.04), but this association was non-significant when adjusted for health anxiety (ρ = –0.08, P = 0.31). These results are consistent with the theory that interoceptive processes draw on both inflammatory mediators and the state of sickness behaviour in inferring health state.
Introduction
Unspecific sickness symptoms such as fatigue, malaise, lack of energy and increased pain sensitivity are common in the general population, and routinely managed in primary care. Such symptoms resemble sickness behaviour, a set of behavioural changes in response to inflammation, putatively functioning to redirect energy to the immune system to promote recovery. 1 It has been proposed that the brain uses both signals of inflammatory activation and ensuing behavioural changes to appraise health status. 2 This mechanism may explain why a simple rating of health status, performed subjectively by the individual and not by a clinician, is a strong predictor of future morbidity and mortality, also when controlling for objective medical health issues and risk factors. 3 In support for such a model, a transient immune activation and ensuing sickness behaviour induced by injecting lipopolysaccharide causes healthy individuals to rate their general health as less favourable. 4 Furthermore, several cross-sectional studies have shown associations between higher levels of systemic inflammatory markers and poor self-rated health.5,6 However, only one study has previously measured sickness behaviour, represented by an ad hoc composite measure, as a potential mediator of the association between inflammatory markers and self-rated health. 5 Since then, a validated measure of sickness behaviour has been published that would be better suited to understanding the relation between inflammation and subjective health ratings. In addition, health anxiety, which refers to persistent and excessive fears of having or of acquiring a serious somatic disease common in medical settings, 7 has not been investigated in this context. Against this background, we hypothesised that patients with higher levels of systemic (interleukin (IL)-6, IL-8 and tumour necrosis factor (TNF)-α) or local (exhaled nitric oxide; FENO) inflammatory markers would rate their health as poorer, and that this association would be mediated by sickness behaviour. Health anxiety was included as a covariate to investigate its potential influence on the association between inflammation and self-rated health.
Methods
Participants
Patients were consecutively recruited during two 6-week periods, starting the first week in February 2012 and the third week in September 2013, from a drop-in clinic at a primary health care centre in Stockholm. The typical patient encounter is a 15-min consultation and the drop-in clinic serves a wide range of medical problems. Consultations regarding annual health examinations, prescriptions for addictive drugs, chronic pain conditions and extensions of sick leave or other certificates are referred to booked appointments and were therefore automatically non-eligible. Pregnant patients, patients under 18 years of age and patients not able to speak and read Swedish were excluded. Out of 215 eligible patients during the first data collection, 179 completed the study (83%). In the second data collection, 132 out of 193 eligible patients completed the study (68%). In total, 311 patients were included.
All participants gave written informed consent after the procedure had been fully explained. Participants received no compensation. The study was approved by the Regional Ethical Review Board in Stockholm Dnr 2011/1851-31/1 and 2012/995-32.
Procedure
Following a regular consultation with a general practitioner, body mass index (BMI) and FENO were measured and the participants completed questionnaires regarding sickness behaviour, self-rated health, health anxiety, and background information. Venous blood for analysis of cytokines was sampled in ethylenediaminetetraacetic acid (EDTA) tubes. The samples were centrifuged, and plasma aliquots were initially stored at −20°C before being transferred to −80°C until analysis. Blood samples were taken between 8:00 a.m. and 12:00 p.m. without fasting, and all patients sat down during at least 15 min before sampling.
Measures
Self-rated health
Self-rated health was assessed using the question ‘How do you rate your general health status’, 8 and was rated on a 5-point Likert-type scale where the response alternatives were very good (1), rather good (2), neither good nor poor (3), quite poor (4) and poor (5).
Sickness behaviour
Sickness behaviour was measured using the ‘Sickness Questionnaire (SicknessQ)’, a 10-item validated questionnaire rated on a 4-point Likert-type scale (with a maximum score of 30 points) in the first data collection. In the second data collection a short form of SicknessQ including four items, ‘SicknessQ4’ (maximum score 12 points), was included, and the SicknessQ4 score is available for both data collections (311 patients). High agreement between SicknessQ and SicknessQ4 was found, ρ = 0.91, P < 0.001.
Health anxiety
Health anxiety was measured using seven items selected to cover a range of health anxiety symptoms aspects from the original 18-item ‘Short Health Anxiety Inventory’ (including Items 1, 3, 8, 9, 10, 11 and 15, see Supplementary Material S1). Items were rated from 1–4 where mean ratings were used with a higher score representing higher health anxiety. The correlation between Short Health Anxiety Inventory (used in Hedman-Lagerlof et al. 7 in a population including 132 patients with health anxiety) and the summary score of the seven items included in the present study was ρ = 0.87, P < 0.001.
Fraction of FENO
FENO was measured according to standardised recommendation using NIOX MINO© (Aerocrine AB, Solna, Sweden). The participant was asked to inhale to total lung capacity through the NIOX MINO followed by exhalation for 10 s at 50 mL/sec (assisted by visual and auditory cues). FENO values (parts per billion) were reported as mean value from two successive measurements divided by predicted normal FENO values in non-atopic adult subjects adjusted for height and age.
Cytokines
EDTA-plasma was used to analyse levels of IL-6, IL-8 and TNF-α with high-sensitive enzyme-linked immunosorbent assays (Quantikine hs ELISA HS600B SS600B (IL-6), HS800 (IL-8) and HSTA00D SSTA00D (TNF-α), R&D Systems, Minneapolis, USA).
Statistics
Partial correlations between cytokines, FENO, SicknessQ, SicknessQ4, health anxiety and self-rated health were calculated with Spearman’s correlation. Partial correlations were adjusted for age and BMI as they are potential confounders in the association between inflammation and subjective health perception, and stratified by sex as a known moderator of the same association. 9 In follow-up exploratory analyses of associations between inflammatory markers, sickness behaviour and self-rated health, health anxiety was added as a covariate. Indirect statistical effects of mediation were tested with the Sobel–Goodman test. Due to the non-normal properties of the included parameters, P values were estimated by bootstrapping with 1000 repetitions. For data analysis, the statistical software STATA® 11.0 and 14.0 (StataCorp LP, Texas, USA) were used. An α level of 0.05 was used for significance tests.
Results
Study group characteristics
Study group characteristics are shown in Supplementary Material S2 Table 1. In total, 74% of the 311 patients were women (mean age: women = 49.7 years and men = 53.4 years). Mean self-rated health was 2.3 in women and 2.5 in men, corresponding to ratings between ‘rather good’ and ‘neither good nor poor’. There were no significant differences between men and women regarding self-rated health, sickness behaviour nor IL-8 (Mann–Whitney U test). However, women were significantly younger, had lower BMI, rated higher health anxiety and had lower FENO values compared to men. In addition, levels of IL-6 were higher in men compared to women, but levels of TNF-α were higher in women compared to men. For both women and men, the most common cause of visit was infection and fever, including almost a third of the sample.
Correlations between sickness behaviour, inflammatory markers and self-rated health
Partial correlations between sickness behaviour, inflammatory markers and self-rated health adjusted for age and BMI are presented in Supplementary Material S3 Table 2 and visually presented in Figure 1. Poor self-rated health was strongly associated with more pronounced sickness behaviour in both men and women. In women, poor self-rated health was associated with low levels of IL-6 (ρ = –0.15, P = 0.036), TNF-α (ρ = –0.19, P = 0.010) and FENO (ρ = –0.22, P = 0.002). In men, poor self-rated health was associated with higher levels of IL-6 (ρ = 0.26, P = 0.010). No strong associations were found between IL-8 or TNF-α and self-rated health in men.

Bivariate scatter plots showing associations between variables of interest in (a) women after rank transformation and (b) men after rank transformation.
Correlations between inflammatory markers and sickness behaviour
Partial correlations between inflammatory markers and sickness behaviour adjusted for age and BMI are presented in Supplementary Material S4 Table 3. Increased sickness behaviour as measured by SicknessQ was significantly associated with increased levels of IL-6 in both women (ρ = 0.19, P = 0.049) and men (ρ = 0.34, P = 0.023). The association was also significant as measured by SicknessQ4 in men (ρ = 0.29, P = 0.005) but not in women. No strong associations were found between IL-8, TNF-α nor FENO and sickness behaviour.
Correlations between sickness behaviour, inflammatory markers and self-rated health with health anxiety as covariate
Higher levels of health anxiety were associated with poor self-rated health in both women (ρ = 0.31, P ⩽ 0.001) and men (ρ = 0.32, P = 0.003), but correlated with lower levels of IL-6 in women (ρ = –0.28, P < 0.001), see Supplementary Material S5 Table 4. Possibly, the correlation between low levels of IL-6 and high health anxiety could be explained by both women and men seeking care for infection and/or fever, had higher levels of IL-6 compared to the rest of the sample (Ps < 0.02, Mann–Whitney rank sum test), while women but not men had a tendency for lower health anxiety (P = 0.07). Thus, as health anxiety seemed to possibly confound the analysis, we performed follow-up exploratory analyses with health anxiety as a covariate in the partial Spearman correlations. Correlations between sickness behaviour, inflammatory markers and self-rated health with health anxiety added to age and BMI as a covariate are presented in Supplementary Material S6 Table 5 and S7 Table 6. The negative correlation between poor self-rated health and higher levels of IL-6 in men remained significant (ρ = 0.28, P = 0.008), while the strength of the correlations between low levels of IL-6 (ρ = –0.08, P = 0.31), TNF-α (ρ = –0.10, P = 0.72), FENO (ρ = –0.14, P = 0.07) and poor self-rated health in women was attenuated and all non-significant. The correlations between increased sickness behaviour and poor self-rated health remained unchanged, and the same was true for the correlations between IL-6 and sickness behaviour. Furthermore, in men but not in women, higher health anxiety was associated with increased sickness behaviour (ρ = 0.29, P = 0.049).
The correlations in women between self-rated health, IL-6 and sickness behaviour with and without the addition of health anxiety as a covariate are graphically presented in Figure 2.
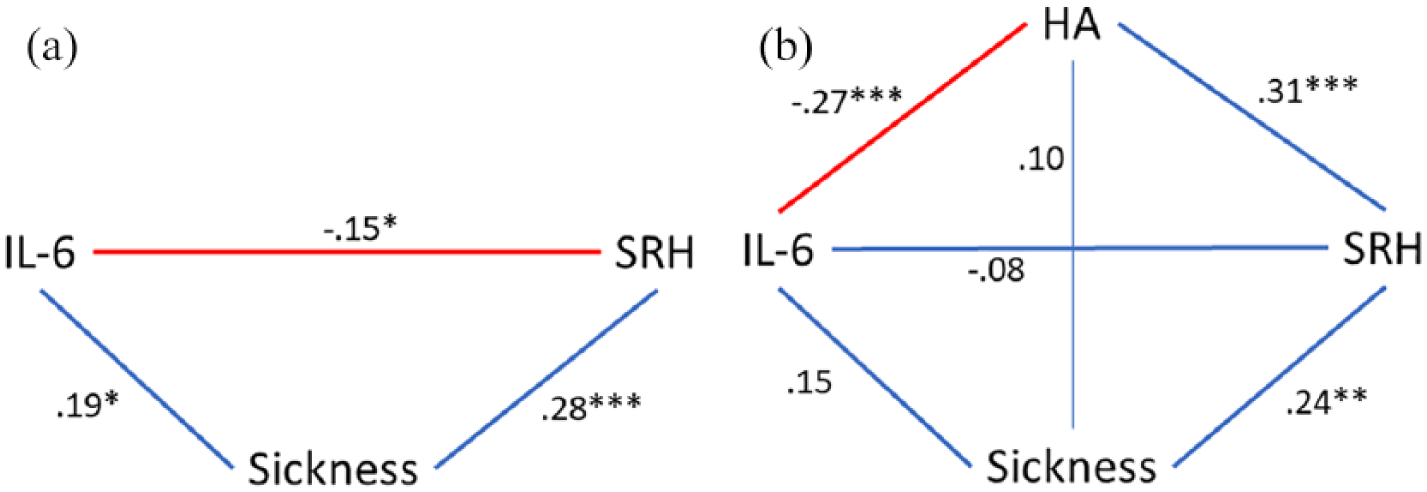
The associations between SRH, IL-6 and sickness behaviour in women without (a) and with (b) the addition of HA as a covariate. Spearman correlation coefficients adjusted for all factors included in each model. (a) High levels of IL-6 were associated with good SRH when HA was not included in the model. (b) High levels of IL-6 were associated with lower HA, which in turn was associated with LOW SRH. High levels of IL-6 were simultaneously associated with higher sickness behaviour, which in turn was associated with HIGH SRH. There was no significant association between IL-6 and SRH when HA was included in the model.
Mediation analysis
Since IL-6 was significantly associated to both self-rated health and sickness behaviour in men, we investigated whether the relationship between IL-6 and self-rated health was statistically mediated by sickness behaviour. We found that neither SicknessQ4 nor SicknessQ were significant mediators of the association between IL-6 and self-rated health (SicknessQ4 = 16.3% mediation—coeff. indirect effect = 0.001, P = 0.35, P(bootstrapped) = 0.90; coeff. direct effect = 0.006, P = 0.008, P(bootstrapped) = 0.66) and SicknessQ (20.8% mediation—coeff. indirect effect = 0.001, P = 0.29, P(bootstrapped) = 0.93; coeff. direct effect = 0.005, P = 0.02, P(bootstrapped) = 0.79). Thus, although there was a significant association between higher IL-6 and sickness behaviour in men, and a significant association between sickness behaviour and self-rated health in the partial correlation analyses, the association between higher IL-6 and poor self-rated health in men was not statistically mediated by sickness behaviour according to the mediation analyses.
Discussion
In this cross-sectional study of primary care patients, higher levels of IL-6, but not the other inflammatory markers, were associated with poor self-rated health in men, but not in women. High levels of IL-6 were associated with more pronounced sickness behaviour, and more pronounced sickness behaviour was associated with poor self-rated health, in both men and women. Even though increased levels of the inflammatory cytokines IL-6, IL-8 and TNF-α have previously been associated with a transient increased SicknessQ-score 1.5 h after injection of endotoxin in an experimental study on humans, 10 this is the first study investigating the naturalistic associations between inflammatory markers and sickness behaviour, here measured by the validated questionnaire SicknessQ, in a primary care population. The association between elevated levels of inflammatory cytokines and poor self-rated health has previously been found in female primary care patients but could not be replicated in this study. Here, increased levels of IL-6 were surprisingly associated with better self-rated health in women. This finding may be explained by the lower ratings of health anxiety in women with infection/fever with a concomitant higher level of IL-6, which may also explain the association between low levels of IL-6 and higher health anxiety in women. In support for this notion, the correlation between low levels of inflammatory markers and poor self-rated health in women was attenuated and rendered non-significant after adjustment for health anxiety. In conclusion, the results from the present study are consistent with the theory that inflammation causes sickness behaviour, and that interoceptive processes draw on both inflammatory mediators and the somatic state of sickness behaviour in inferring health state. Further studies will be required to corroborate these causal links.
Supplemental Material
ms_SIA_cyto_SRH_supplements – Supplemental material for Cross-sectional associations between inflammation, sickness behaviour, health anxiety and self-rated health in a Swedish primary care population
Supplemental material, ms_SIA_cyto_SRH_supplements for Cross-sectional associations between inflammation, sickness behaviour, health anxiety and self-rated health in a Swedish primary care population by Karin Lodin, Mats Lekander, Predrag Petrovic, Gustav Nilsonne, Erik Hedman-Lagerlöf and Anna Andreasson in European Journal of Inflammation
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Stockholm Stress Center. The study sponsor was not involved in interpretation of data, study design, collection, analysis or interpretation of data, nor in the writing of or the decision to publish the report.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.