
Abstract
Bloodstream infection (BSI) is a severe infectious complication in critically ill patients. This study was aimed to investigate the diagnostic accuracy of procalcitonin (PCT) to differentiate Gram-negative bacteria (Gram-neg) from Gram-positive bacteria (Gram-pos) and fungal BSI. PCT and other inflammation markers of monomicrobial BSI patients were retrospectively collected and compared between patients with Gram-neg, Gram-pos, or fungal BSI. The differential diagnosis performance of PCT was evaluated by receiver operating characteristic curves (ROC). The area under curve (AUC) of PCT for differentiating Gram-neg BSI from Gram-pos BSI was 0.95 with an optimal cut-off value of 4.15 ng/mL, a sensitivity of 82.05%, and a specificity of 96.15%. AUC of PCT for differentiating Gram-neg BSI from fungal BSI was 0.92 with an optimal cut-off value of 3.13 ng/mL, a sensitivity of 84.62%, and a specificity of 88.89%. Serum PCT concentration can be used to differentiate Gram-neg from Gram-pos and fungal BSI.
Keywords
Introduction
Bloodstream infection (BSI) is caused by a broad spectrum of causative pathogen. A recently published multicenter observational study found that among hospital-acquired BSIs in intensive care unit (ICU), 58.3% were caused by Gram-negative bacteria (Gram-neg), 32.8% Gram-positive bacteria (Gram-pos), 7.8% fungi, and 1.2% due to strict anaerobes. 1 If BSI is suspected, for the lack of evidence of causative pathogen and its sensitivity to antibiotics, initial antibiotic treatment has to be guided by empirical data. It was reported that inappropriate empirical antibiotic treatment was positively associated with a higher risk of drug resistance, longer hospital stays, and a higher rate of death in patients with BSI.2,3
Procalcitonin (PCT) was reported to be a rapid biomarker for diagnosing bacterial infections, guiding the initiation or termination of antibiotic treatment, and evaluating the appropriateness of therapy. 4 Several recent studies found that PCT serum concentration was higher in patients with Gram-neg BSI than those with Gram-pos or fungal BSI.4–6 However, the power of PCT to discriminate distinct groups of pathogens and guide initial empirical antibiotic choices is still controversial. This study aimed to investigate the diagnostic ability of PCT to differentiate Gram-neg from Gram-pos and fungal BSI in critically ill patients.
Materials
Clinical and laboratory data were retrospectively collected from ICU in the First Affiliated Hospital of the University of Science and Technology of China between January 2014 and July 2018. Inclusion criteria were as follows: (1) clinical manifestations of infection; (2) monomicrobial BSI: isolation of only one pathogen from two or more blood culture in one BSI episode; (3) PCT and blood culture collected simultaneously from consecutive blood samples; and (4) 18 years of age or older. In the case of two or more BSI episodes observed in one patient, only the first one was considered. One BSI episode was defined as the time period associated with one or more positive blood culture specimens until at least two subsequent blood cultures conducted every 24 h were negative. 4
Exclusion criteria were as follows: (1) history of the immune system disease or history of taking immunosuppressive drugs; (2) history of malignant tumors; and (3) history of acute pancreatitis. The following data were collected from the medical file of each patient: (1) main clinical and epidemiological data on ICU admission, including age, gender, sequential organ failure assessment (SOFA) scores, and 28-day mortality. (2) White blood cells (WBC, 109 L−1) and C-Reactive protein concentration (CRP, mg/L) within 12 h before or after blood culture extraction.
Blood culture samples (aerobic and anaerobic) were collected by sterile venipuncture and processed using the BACTEC 9240 automated blood culture system. Plasma PCT levels were assessed by FS-112 II immunofluorescence measurement instrument according to the manufacturer’s instructions (Wondfo, Guangzhou, China). The linear range of detection was 0.1–100 ng/mL, and the sensitivity of the assay was 0.01 ng/mL.
Statistical analysis was performed by the software SPSS 25.0 (SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as mean ± standard deviation or median and interquartile range (IQR) unless otherwise stated. One-way analysis of variance (ANOVA) and Kruskal–Wallis nonparametric ANOVA were used for multi-group comparisons, and Dunnett’s multiple comparison tests were used to detect differences between the two groups. Categorical variables were compared using the Chi-square test. All tests were performed as two-tailed tests. P < 0.05 was considered statistically significant. The diagnostic accuracy was evaluated by receiver operating characteristic curve (ROC) and described by the following parameters: sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). The area under the curve (AUC) was used to assess diagnostic accuracy. Youden’s index (Youden’s index = sensitivity + specificity − 1) was calculated to find the optimal cut-off value.
Results
In all, 83 patients of monomicrobial BSI were collected, among which 26 patients were positive with Gram-pos, 39 patients positive with Gram-neg, and 18 patients positive with fungal. There was a significant difference in gender (20 males and 6 females, 20 males and 19 females, and 5 males and 13 females, respectively, P < 0.05) and no significant difference in age (61.08 ± 17.82, 63.31 ± 17.72, and 60.11 ± 13.65 years, respectively, F = 0.265, P > 0.05) between patients with Gram-pos, Gram-neg, or fungal BSI. The SOFA scores were higher in patients with Gram-neg BSI (8, IQR: 6–12.75) than those with Gram-pos BSI (4, IQR 3–5, P < 0.01) or fungal BSI (2.5, IQR 1.75–3.25, P < 0.01). During the first 28 days, 6 (23.07%) patients with Gram-pos BSI, 19 (48.72%) patients with Gram-neg BSI, and 4 (22.22%) patients with fungal BSI, respectively, died. The 28-day mortality was higher in patients with Gram-neg BSI than those with Gram-pos BSI (χ2 = 4.33, P < 0.05).
There were no difference in WBC (10.96 ± 4.81 × 109 L−1, 10.14 ± 7.01 × 109 L−1, and 10.70 ± 4.33 × 109 L−1, respectively, F = 0.163, P > 0.05) and CRP concentrations (124.59 ± 64.59 mg/L, 144.42 ± 67.33 mg/L and 110.03 ± 62.79, respectively, F = 1.864, P > 0.05) between patients with Gram-pos, Gram-neg or fungal BSI (Figure 1(a) and (b)). PCT concentrations were significantly higher in patients with Gram-neg BSI (10.91 ng/mL, IQR: 5.14–33.0) than those with Gram-pos BSI (0.8 ng/mL, IQR: 0.59–2.01, H = –37.18, P < 0.0001) or fungal BSI (1.07 ng/mL, IQR: 0.56–2.11, H = 34.38, P < 0.0001), and there was no difference in PCT concentrations between patients with Gram-pos or fungal BSI (H = –2.80, P > 0.05; Figure 1(c)).

(a) WBC, (b) CRP, and (c and d) PCT levels corresponding to pathogens isolated from two blood cultures. Data are presented as a box plot with median lines, 25th and 75th percentile boxes, and 10th and 90th percentile error bars. The Y-axis is a log two scale in c and d. (NS: not statistically significant; ****P < 0.0001, **P < 0.01).
Distribution of BSI pathogens and their corresponding PCT concentrations are summarized in Table 1. Klebsiella pneumoniae and Acinetobacter baumannii were the most frequent causative bacterial species, and Candida albicans were the most frequent causative fungal species. Furthermore, PCT concentrations were significantly higher in patients with A. baumannii (11.30 ng/mL, IQR: 5.54–23.65, H = –15.51, P < 0.01) or K. pneumoniae BSI (18.02 ng/mL, IQR: 7.77–53.7, H = –26.95, P < 0.0001) than those with other BSI pathogens (0.99 ng/mL, IQR: 0.59–2.15; Figure 1(d)).
PCT levels corresponding to different pathogens isolated from blood cultures.
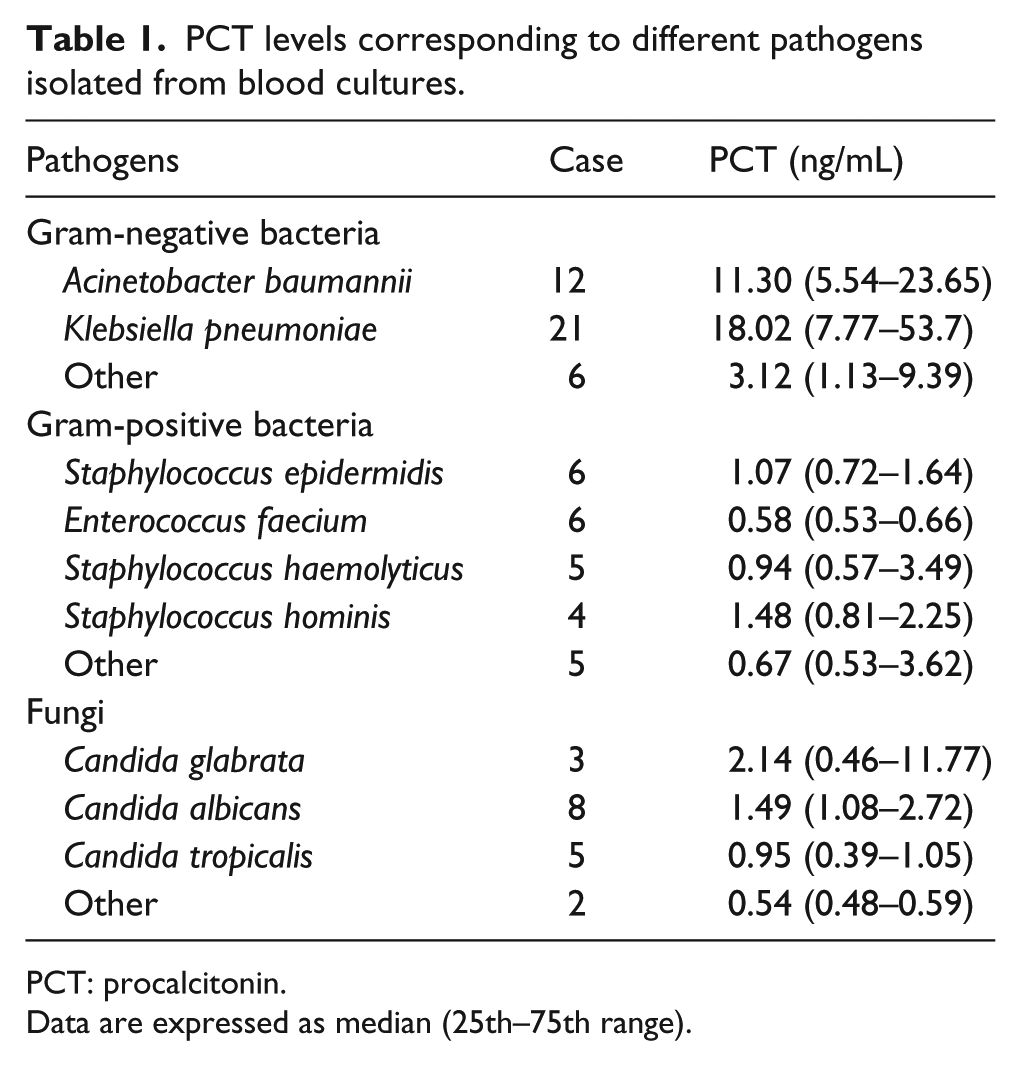
PCT: procalcitonin.
Data are expressed as median (25th–75th range).
The differential diagnosis of PCT was revealed by ROC analysis. For differentiating Gram-neg from Gram-pos BSI, PCT had the estimated AUC of 0.95 and the optimal cut-off value of 4.15 ng/mL, resulting in the sensitivity of 82.05%, specificity of 96.15%, PPV of 96.97%, and NPV of 78.13% (Figure 2(a), red line). For differentiating Gram-neg from fungal BSI, PCT had the AUC of 0.92 and the optimal cut-off value of 3.13 ng/mL, resulting in the sensitivity of 84.62%, specificity of 88.89%, PPV of 94.29%, and NPV of 64.00% (Figure 2(a), blue line).

Receiver operating characteristic curve for PCT to discriminate (a) Gram-neg BSI from Gram-pos BSI (in red line) and Gram-neg BSI from fungal BSI (in blue line) and (b) Acinetobacter baumannii BSI from other BSI pathogens (in red line) and Klebsiella pneumoniae BSI from other BSI pathogens (in blue line).
In addition, PCT had an AUC of 0.90 for differentiating K. pneumoniae from other causative BSI pathogens. The optimal cut-off value was 5.12 ng/mL, resulting in the sensitivity of 79.03%, specificity of 90.48%, PPV of 59.38%, and NPV of 96.08% (Figure 2(b), blue line). PCT had the AUC of 0.77 for differentiating A. baumannii from other BSI pathogens. The optimal cut-off value was 6.84 ng/mL, resulting in a sensitivity of 73.24%, specificity of 75.00%, PPV of 32.14%, and NPV of 94.55% (Figure 2(b), red line).
Discussion
The treatment and prognosis of BSI patients depend on different types of causative pathogens. This study showed that the isolated rate of Gram-neg from BSI was higher than Gram-pos and fungal, and the SOFA scores and 28-day mortality rates were higher in patients with Gram-neg BSI than those with Gram-pos or fungal BSI. In addition, K. pneumoniae and A. baumannii were the first two frequent bacteria of Gram-neg type. This result was consistent with the data from Italian Nosocomial Infections Surveillance in Intensive Care Units (SPIN-UTI) network that K. pneumoniae and A. baumannii were two of the most commonly isolated pathogens in ICU-acquired infections.7–9 Unfortunately, infections caused by multidrug-resistant A. baumannii (MDR-AB) and K. pneumoniae carbapenemase–producing K. pneumoniae (KPC-Kp) have increasingly appeared among critically ill patients in ICU.10,11 Antibiotic resistance is a major risk factor for growing medical costs, treatment failure, and increased mortality, making a grave threat to global public health. Therefore, biomarkers, which help to initiate empiric antibiotic therapy early and appropriately, have been paid close attention.
The potential of PCT to differentiate pathogen of BSI had been recently studied. Brodská et al. 5 found that the PCT levels in Gram-neg BSI was significantly higher than those in Gram-pos BSI and fungal BSI, and ROC curve analysis showed the AUC of 0.871 for PCT differentiating Gram-neg BSI from Gram-pos and fungal BSI.
Yan et al. 4 found that PCT levels were significantly higher in septic patients with Gram-neg BSI than those with Gram-pos BSI, and PCT levels were also significantly higher in septic patients with abdominal infection or urinary tract infection than those with pneumonia or infective endocarditis. In 2018, Thomas-Rüddel et al. 6 reported a prospective study including 4858 septic patients with organ dysfunction and found that in septic patients with positive blood cultures, PCT concentrations were higher in Gram-neg BSI than Gram-pos and fungal BSI, and in septic patients with a single focus of infection, PCT concentrations were different between the different foci of infection. Multivariate analysis in this study demonstrated that the spectrum of pathogens and focus of infection were independently associated with PCT concentrations in sepsis patient. This results suggested that PCT serum concentrations were determined not only by distinct groups of pathogens but also by different foci of infection.
Our study found that in critically ill patients with double positive blood cultures, PCT concentrations were significantly higher in Gram-neg BSI than Gram-pos BSI or fungal BSI. The ROC curve revealed a high diagnostic ability of PCT for differentiating Gram-neg from Gram-pos and fungal BSI. Our results confirmed that for suspected BSI, PCT might be a biomarker for guiding initial empirical antibiotic treatment. In addition, PCT levels in patients with A. baumannii and K. pneumoniae BSI were higher than patients with other BSI pathogens. The ROC curve revealed a high diagnostic ability of PCT for differentiating A. baumannii and K. pneumoniae BSI from another pathogen BSI. So, considerably high PCT concentrations might indicate A. baumannii and K. pneumoniae BSI among critically ill patients.
Although the underlying mechanism is still not completely clear, the observed differences of PCT levels in response to different pathogens may be partly due to the differences in pathogenic inflammatory signaling pathways and cytokines. Lipoteichoic acid (LTA), the pathogen-associated molecular patterns (PAMPs) that only exist in the cell walls of Gram-pos, is recognized by Toll-like receptor 2 (TLR2), while lipopolysaccharides, the PAMP that only exists in the cell walls of Gram-neg, is recognized by Toll-like receptor 4 (TLR4). 12 Tumor necrosis factor-α (TNF-α), interferon-γ (IFN-γ), interleukin-4 (IL-4), IL-8, and IL-10 plasma levels were higher in abdominal sepsis patients affected by Gram-neg than in those affected by Gram-pos. 13 Heat-shock protein 60 (Hsp60), β-glucans, phospholipomannan, O-linked mannans, zymosan, fungal DNA, and this fungal PAMPs are recognized by various TLRs including TLR 2, TLR 4, and TLR 9. IL-6, IL-8, IL-1β, IFN-γ, macrophage inflammatory protein-1α (MIP-1α), and MIP-1β are produced in response to fungal infections, promoting mast cell stimulation and the release of histamine, proteoglycans, proteases, and IgE. 14 These different cytokines’ release probably leads to the observed different PCT levels in Gram-neg, Gram-pos, and fungal BSI.
There are several limitations to our study. First, the discriminatory power of PCT was investigated only in patients with BSI, not including patients with other sites’ infection, so the clinical application is correspondingly restricted. Second, PCT levels are affected by underlying diseases and complications, such as severe shock, cardiac insufficiency, rhabdomyolysis, autoimmune disorders, renal insufficiency, and others. However, this information was not available in this study, affecting the analysis concluded.
In conclusion, the level of serum PCT had clinical value in differentiating Gram-neg from Gram-pos and fungal BSI in critically ill patients. So, it could provide the basis for initiating early empiric antimicrobial therapy, avoiding inappropriate antibiotic therapy and consequently reducing related adverse outcomes. In addition, considerably high PCT levels might indicate K. pneumoniae and A. baumannii BSI in critically ill patients.
Footnotes
Acknowledgements
All authors contributed equally to the design, data acquisition, and manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest concerning the research, authorship, and publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was financially supported by the International Science & Technology Cooperation Program of Anhui Province (No. 1403062022; Hefei, Anhui, China).