
Abstract
Background
Omalizumab is shown to be effective in the treatment of chronic spontaneous urticaria (CSU), a disease with high personal and social impact. Sex differences in CSU are recognized with women more frequently affected. Scarce is the knowledge about response to omalizumab between sex groups. We sought to identify any differences based on the sex of patients receiving omalizumab.
Methods
We evaluated data of patients diagnosed with CSU refractory to high-dose second-generation H1 antihistamines and treated with 300 mg omalizumab every 4 weeks for 6 months and then at relapse.
Results
Discussion: All patients, regardless of sex, age, or any other factor, achieved the clinical remission of the disease after the first 3 doses with a reduction of the disease activity indices and impact on the quality of life. Recurrences predominate in men, two months after the suspension of the drug. Respect to sex and recurrence we did not find any correlation with age, body mass index, peripheral eosinophil counts, total IgE levels, D-dimer, plasma prothrombine level or C-reactive protein. We found no sex differences in tolerability and safety. CSU in girls may persist longer and have worse prognosis, but no one has so far noted sex differences in response to omalizumab.
Conclusions
Although there are no certainties on the mechanism of action of omalizumab in CSU, the noticeable difference in response between males and females lead us to suppose a role of the hormonal balance both on the pathogenesis of the CSU and on the efficacy of OmAb.
Introduction
Chronic spontaneous urticaria (CSU) is a heterogeneous inflammatory itching skin disease 1 in which the female to male ratio is approximately 2–4:1 but to date we ignore the pathogenic mechanism determining the female prevalence. Sex dependent immunological features may be responsible for this predilection. 2 CSU is a common nosological entity in older individuals, although few data are available regarding clinical features and epidemiology in the elderly.3-5 Omalizumab (OmAb) is recommended to be added to CSU therapy if sufficient improvement does not occur after 2–4 weeks that the dose of second-generation H1 antihistamines were increased up to fourfold.6-8 10–30% of patients do not achieve a satisfactory control of the disease and recurrence is possible. 9 Epidemiology shows the weight of sex’s matter in CSU but sex- or gender-stratified analysis for treatment efficacy is missing. Unfortunately, in clinical practice, the sex and gender differences are still neglected in the era of precision medicine. The objective of our study was to identify any differences between female and male patients receiving OmAb, in terms of tolerability, safety, and clinical efficacy.
Materials and methods
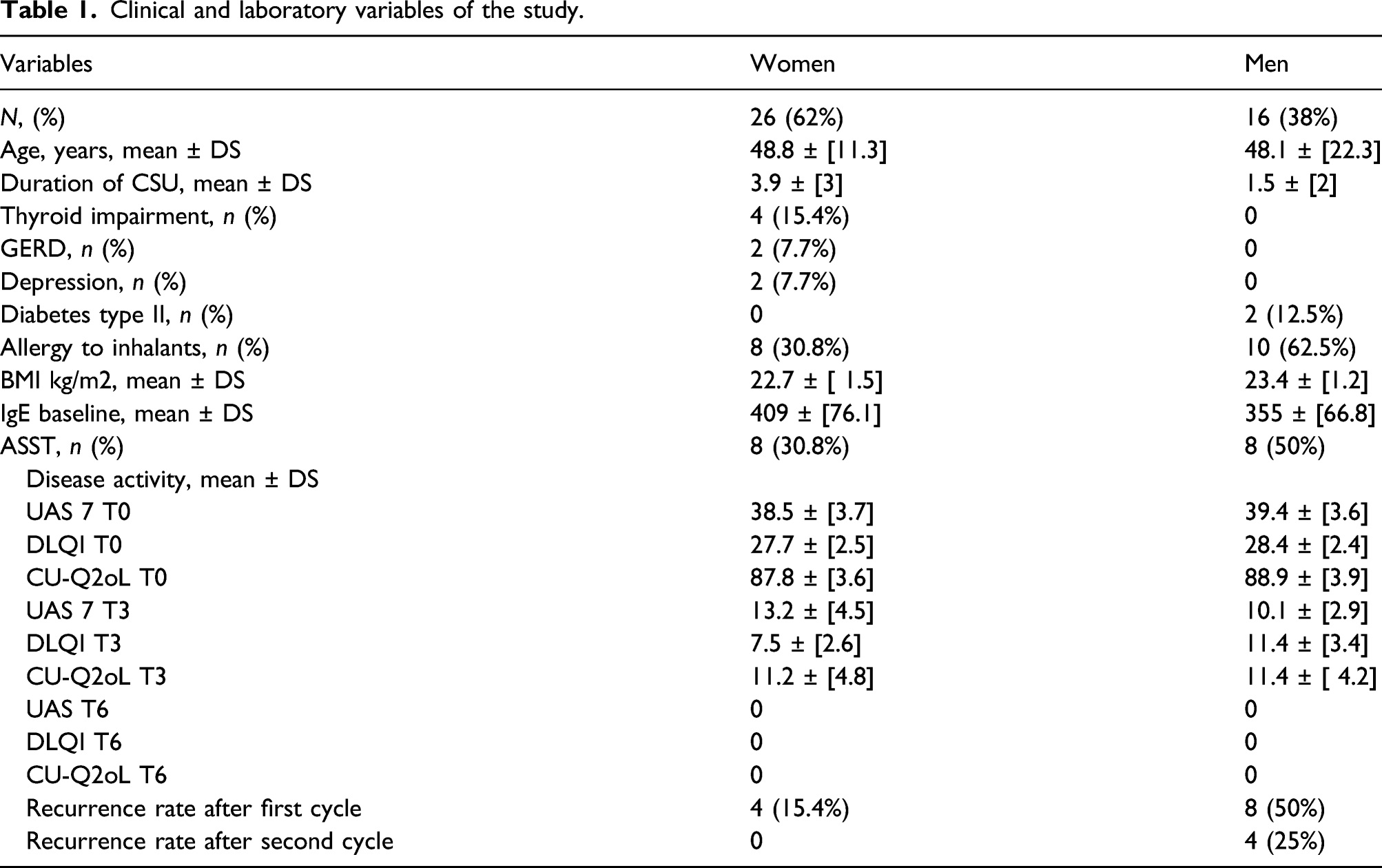
Clinical and laboratory variables of the study.
Clinical and laboratory variables in woman.

Clinical and laboratory variables in men.

The study was conducted according to Good Clinical Practice guidelines, the Declaration of Helsinki, was approved by the local ethics committee (Internal Review Board University of L Aquila ex “Academic Ethics Committee” D.R. n. 206/2013 modified D.R. n. 46/2017) and written informed consent was obtained from each participant.
Results
After 3 months of treatment (T3) with OmAb, the mean value of UAS 7 improved to 13.2 ± [4.5] points (range 5–22) for women, and then zeroed at the end of the treatment when nobody showed signs or disease symptoms. Similar trend for male patients who at T3 had an average UAS 7 value of 10.1 ± [2.9] points (range 6–14) and 0 points at the end of the treatment. The mean DLQI value at time 0 (T0) was 27.7 ± [2.5] points (range 30–25) for women and 28.4 ± [2.4] points (range 30–24) for men. At T3 the same value was 7.5 ± [2.6] points (range 3–12) for women and 11.4 ± [3.4] points (range 6–16) for men. Average of CU-Q2oL score at T0 was 87.8 ± [3.6] (range 80–92) for women and 88.9 ± [3.9] (range 80–92) for men, at T3 was 11.2 ± [4.8] (range 5–22) for women and 11.4 ± [4.2] (range 5–20) for men. After six months of treatment patients achieved in both scale 0 points with clinical remission in all patients. To the next evaluations, 8 males (50%) resorted to a second cycle of therapy and 4 (25%) to a third OmAb cycle. Only 4 (25%) men definitively recovered after the first cycle. Instead among females, 22 (84.6%) were in complete remission and 4 (15.4%) underwent a second cycle. After 4 months of observation by the end of the last therapeutic cycle no women showed recurrence. Among the six male subjects with the highest relapse rate, then undergoing the third therapeutic cycle with OmAb, four were positive for autologous serum skin test (ASST) (25%), two (12.5%) of the six with only one recurrence, and two (12.5%) of the four first cycle responders were ASST positive. In the female sample, half of the non-responders in the first treatment cycle were positive for ASST (7.7%), while six (23.1%) of the twenty-two responders were positive. Although there was a greater ASST positivity among men with more relapses, a greater response to treatment was found among women despite the higher ASST positivity rate. The mean IgE level in women with remission in the first cycle of therapy was 478.69 while the non-responders in the first cycle had an average level of IgE less than 23.7. On the contrary in the male sample, the highest level of IgE was found in patients with a relapse after the first therapeutic cycle with a mean value of 749, mean values equal to 155.1 were documented in patients with double relapse and then underwent the third therapeutic cycle, while the lowest values (mean 14.4) were detected in the responders at the first OmAb cycle. Although in the literature it is documented high basal IgE levels (above 100 KU/l) in CSU patients responsive to treatment and with a faster relapse after discontinuation of therapy, this seems to happen in our sample only for the female population while the data relating to men would seem not to comply with what is reported, offering a further reason for reflection on the possible implication of gender difference.11,12 Our analysis laboratory is not equipped for distinguishing free IgE from those linked to OmAb or to effector cells this makes IgE assay after therapy of little significance. 13 All patients, regardless of sex, age, or any other factor, achieved a partial clinical remission of the disease after the first 3 doses of OmAb with a reduction of the disease activity indices and impact on the quality of life measured by UAS7, DLQI, and CU-Q2oL.14,15 Thus confirming effectiveness of the therapy and improvement of the patient’s quality of life. 16
Discussion
The identification of response biomarkers to therapy in CSU is a key topic and was showed as the combination of eosinopenia and basopenia is a better predictor of non-response to second-generation H1 AH than eosinopenia alone. 17 Several biomarkers have been indicated to differentiate severity and prognosis in CSU patients: older patients have more severe disease, females have a longer remission, duration of urticaria is directly linked to severity, such as with less evidence positivity of ASST, the coexistence of angioedema seem to have a less favorable prognosis.18,19 In our patients, recurrences predominate in men, two months after the suspension of the drug. Respect to sex and recurrence, we did not find any correlation with age, body mass index, peripheral eosinophil counts, total IgE levels, D-dimer, plasma prothrombine level or C-reactive protein. We found no sex differences in tolerability and safety. No one has so far noted these sex differences as well as recently in the study by Özyılmaz-Bozat G. et al. that found no differences with respect to sex between recurring and not recurring patients although in a previous research they showed that CSU in girls may persist longer and have worse prognosis. 20 Gouder C. et al., analyzing the difference between men and women in terms of effectiveness, tolerability, and response rate of OmAb found no difference in their study on the patients Maltese with asthma. 21 Recently Johal KJ et al. explored if under OmAb treatment of CSU the rate of clinical remission is concordant with baseline basophil features or the rate of change of IgE-dependent functions of basophils and/or plasmacytoid dendritic cells. Their data show as changes in basophil IgE based HR, surface IgE or FcεRI, bear no relationship to the kinetics in the change in clinical symptoms while the baseline basophil count and basophil functional phenotype may be predictive of responsiveness to OmAb. Analyzing their data, it should be noted that among 7 non-responders basopenic patients 4 are males out of 6; of the other two one is basopenic unclassified and the last is non-basopenic responder. 22 These numbers are consistent with our personal experience showing a better response to OmAb in women than in men with CSU: 84.6% of complete remissions in women versus 25% in men after the first cycle of OmAb. A recent review on the predictors of treatment response in CSU show a strong level of evidence for no association of sex as a possible markers of non-response to OmAb. 23 In their recent work, Yu et al. 24 observed that gender is not linked to the speed of achieving complete control with OmAb treatment.
Although there are no certainties on the mechanism of action of OmAb in with CSU,25,26 the noticeable difference in response between males and females lead us to suppose a role of the hormonal balance both on the pathogenesis of the CSU27,28 and on the efficacy of OmAb. In fact, CU is at least twice as frequent in women than in men and may be associated with several diseases and conditions characterized by sex hormones fluctuations as female hormones have immunologic effects and modulate the inflammatory response while gender differences in the expression profiles of histamine receptors and of mast cells exists. Recent studies revealed that a female predominance of urticaria is observed only in specific age groups. Hyun-Sun Yoon et al. also showed a clear female predominance for new-onset urticaria only for those aged 20 × 1044 and 45 × 1064 years. A female predominance of urticaria in specific age groups could be due to estrogen. Estrogen is believed to enhance humoral immunity and antibody synthesis. The fact that CU is twice as frequent in women than in men and may be associated with some diseases and conditions characterized by sex hormone changes, include hormonal contraceptives, pregnancy, menstrual cycle, menopause, and or hormone replacement therapy, suggest that fluctuations in hormonal milieu may play a role in pathogenesis of the disease. A support of this hypothesis is that, like estradiol, low concentrations of environmental estrogens are capable of causing mast cell degranulation, suggesting their role in the pathogenesis of mast cell-dependent diseases. A gender difference in the expression profiles of histamine receptors and of mast cells was demonstrated, also, in experimental studies. These characteristics lead to the hypothesis that OmAb may affect differently depending on the gender, explaining the lower recurrence rate in women present in our study.29,30 The limitations of the study are the paucity of the sample as conducted in a small peripheral center and based on a disease with a low incidence in the population. A further limitation is that sample power analysis was not performed. Although limited by a small sample this study offers the possibility to reflect on the gender difference in the context of therapy with OmAb.31-34 It will be a future objective to expand the series over time to evaluate the influence of gender on a larger sample.
Conclusions
In conclusion, OmAb is an effective and safe drug in the treatment of CSU and our results show a better response in women than in men. Further studies would be useful in order to confirm our data and to highlight possible mechanisms underlying the sex differences of OmAb effectiveness. It is important to increase the awareness of potential sex-specific effectiveness of therapy also in allergies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This type of study does not require specific approval from our ethics committee. We have strictly adhered to the rules laid down in these cases by our Internal Review Board of the University of L’Aquila, Italy, (ex “Comitato etico di Ateneo” D.R. n. 206/2013 modified D.R. n. 46/2017) and conducted in accordance with the 1975 Helsinki Declaration and its subsequent amendments.
Informed consent
Written informed consent was obtained from all subjects before the study.