
Abstract
Objective: Being overweight is associated with an increased risk of diabetes mellitus, hypertension, and cardiovascular disease. Lipoprotein-associated phospholipase A2 (Lp-PLA2) can independently predict the risk of cardiovascular disease. This study is aimed to investigate whether Lp-PLA2 was associated with an overweight status. Methods: This was a cross-sectional study that enrolled 3760 Chinese adults (age, 18–50 years) who underwent medical examination department of Xiamen Chang-Gung Hospital (XCGH) from 2018 to 2020. To explore the distribution of overweight classifications in the Chinese population, we evaluated the correlation of the overweight status with Lp-PLA2, after correcting for possible influencing factors. Results: The Lp-PLA2 level was greater in male than in female subjects (p < 0.001). Subjects with a central overweight status had a greater Lp-PLA2 level than those with normal weight and a peripheral overweight status, in both male and female cohorts. The Lp-PLA2 level was significantly greater in those with additional comorbidities (namely diabetes mellitus (DM), hypertension (HTN), overweight, and metabolic syndrome (MetS)). The age-adjusted and LDL-adjusted Lp-PLA2 level also was significantly higher in the DM (+) and HTN (−) subgroups than in the DM (−), HTN (−), DM (−), and HTN (+) subgroups. Conclusion: Lp-PLA2 is associated with sex, central overweight status, diabetes, hypertension, and MetS in adults aged < 50 years and the age-adjusted and LDL-adjusted Lp-PLA2 was significantly higher in the DM (+) and HTN (−) subgroups than in the DM (−) and HTN (−) and DM (−) and HTN (+) subgroups.
Introduction
Obesity is a chronic metabolic disease 1 that contributes to inflammatory response in the adipose tissue, 2 and its prevalence is also increasing worldwide. 3 Obesity is closely associated with cardiovascular diseases, 4 such as hypertension and hyperlipidemia. 5 Therefore, it is important to assess cardiovascular-predictive factors associated with obesity.
Lp-PLA2 (lipoprotein-associated phospholipase A2) catalyzes the hydrolysis of acetyl ester at the sn-2 position of platelet-activating factor (PAF), 6 also known as platelet-activating factor acetylhydrolase (PAF-AH). It is a calcium‐independent serine lipase produced predominantly by the macrophages, monocytes, T lymphocyte, and mast cells, which circulates by binding mainly to apolipoprotein B (apo B), 7 with the low-density lipoprotein (LDL) (80%) and high-density lipoprotein (HDL) (20%), 8 could independently predict cardiovascular risk. 9 Since Lp-PLA2 activity is positively associated with LDL and adiposity 10 that helps predict the risk of atherosclerosis and cardiovascular disease. 11 Lp-PLA2 had significant positive correlation with systolic, diastolic, mean arterial pressure (MAP), total cholesterol, LDL, plasma glucose, and HbA1c 12 as well, so it may be a proper predictor for obesity.
LDL oxidation is associated with lipid peroxidation, an extensive hydrolysis, and releasing pro-inflammatory mediators like oxidized fatty acids (oxFA) and lysophosphatidylcholine (lysoPC). 13 The hydrolysis is mediated through a Lp-PLA2 which is closely associated with LDL. 14 The study by Laura Jackisch et al. suggests that adipocytes viewed as an important contributing source of Lp-PLA2 expression in adipocytes and adipose tissue. Also, a multiple-regression model found triacylglycerols as the key predictor of Lp-PLA2, 15 so we may predict obesity by measuring Lp-PLA2.
Lp-PLA2 is a novel inflammatory biomarker of cardiovascular disorders in metabolic diseases 12 that can provide important information about plaque inflammation and stability 16 and is also the main cause of coronary artery disease. The United States Food and Drug Administration approved Lp-PLA2 as a predictor of coronary artery disease using the PLAC Test ELISA kit on December 2014. 17 It may also be used to predict obesity as an independent risk factor. In summary, both an overweight status and increased Lp-PLA2 activity can cause heart damage.
Internationally, the most common parameters for measuring obesity are the waist-to-height ratio (WHtR) and body mass index (BMI), which evaluate the degree of obesity through weight, height, and waist circumference. Few studies have analyzed the correlation between Lp-PLA2 and an overweight status in the Chinese population. Therefore, we aimed to analyze the correlation between the overweight type and Lp-PLA2 level through physical health examinations and to better understand the difference sexes.
Methods
Subjects and data collection
This was a cross-sectional study that enrolled 3760 Chinese adults (age, 18–50 years) who underwent health examinations at the medical examination department of XCGH from 2018 to 2020. The study was approved by the Institutional Review Board of XCGH (XMCGIRB2020030) and was conducted in accordance with the Declaration of Helsinki in 2013. Trained nurses collected the data at the health examination by using a standardized questionnaire that contained all complete data, including past history, personal history, medication history, fasting time, and physical examination data, including weight, height blood pressure, and waist circumference. We excluded subjects (1) age younger than 18 years old or over 50 years old; (2) with pregnancy, which affects metabolic tests; (3) who were not fasting for more than 12 hours, which affects metabolic test values; (4) with chronic diseases that significantly affect metabolic function, such as abnormal thyroid function, status post thyroidectomy, chronic hepatitis, liver cirrhosis, pituitary gland disease, adrenal gland disease, and malignant tumors.
Laboratory measurements
The clinical chemistry workup included fasting blood glucose (FBG) measured by Hexokinase enzyme assay (Cobas Mira Chemistry System: Roche Diagnostic Systems, Montclair, NJ); total cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL), and triglycerides (TG) measured by automatic biochemical analyzer (DxC 800, Beckman CoulterUniCel® DxC SYNCHRON®, Ireland). Glutamic pyruvic transaminase (GPT), creatinine, and lipoprotein-related phospholipase A2 (Lp-PLA2) with quantitative test measured by turbidimetric immunology (ABBOTT ARCHITECT c8000/c16000).
Body height and weight were measured using scales and calibrated meters, respectively. BMI was estimated using the following formula: body weight (kg)/[height (m)]2, the cut-off point was 24 kg/m2, 18 with normal BMI <24 kg/m2 and overweight BMI ≥24 kg/m2. Waist circumference was measured between the lowest rib and the midpoint of the iliac crest. The cut-off point of the waist-to-height ratio (WHtR) was 0.5, with peripheral overweight definition: WHtR < 0.5 and central overweight definition: WHtR ≥ 0.5. 19 Blood pressure was measured after a 15-min rest, and the subject was seated using an automated sphygmomanometer which is placed on the right arm. The mean arterial pressure was calculated using the following equation: (2/3) × diastolic pressure + (1/3) × systolic pressure. 20 Hypertension was defined as systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg. Diabetes mellitus was defined as fasting glucose ≥ 7.0 mmol/L. Metabolic syndrome (MetS) was defined as subjects who had three or more of the following criteria: (1) waist circumference ≥ 90 cm in men and ≥ 80 cm in women; (2) hypertriglyceridemia: triglycerides (TG) ≥ 1.7 mmol/L (3) low HDL level < 1.03 mmol/L in men and < 1.29 mmol/L in women; (4) blood pressure ≥ 130/85 mmHg; and (5) fasting glucose ≥ 5.6 mmol/L.
Statistic analysis
According to a previous study investigating the relationship between LDL and Lp-PLA2 level in type 2 diabetic patients, the standardized regression coefficient of LDL was 0.11. Given the effect size, a minimum sample size of 1966 was required to achieve a type I error of 1% and power of 99%. 12 The basic characteristics of male and female subjects were compared using an independent sample t-test for continuous variables or the chi-square test for categorical variables. We further compared the Lp-PLA2 level of subjects according to the presence or absence of comorbidities (hypertension, diabetes, MetS, and weight status) using an independent sample t-test in the whole cohort and after stratifying by sex. The basic characteristics of the subjects among different overweight types (normal weight, peripheral overweight, and central overweight) were compared using one-way analysis of variance for continuous variables or chi-square test for categorical variables. A pairwise comparison was performed using the Bonferroni adjustment when the overall test was significant. Finally, the Lp-PLA2 levels of subjects were compared according to the combination of hypertension and diabetes mellitus using a general linear model in which age was adjusted. In an alternative model, LDL-adjusted Lp-PLA2 levels were compared among the subgroups. All tests were two-tailed, and statistical significance was set at p < 0.05. Data analyses were conducted using SPSS 25 (IBM SPSS Inc., Chicago, IL, USA).
Results
The basic characteristics of the study subjects by sex.

SBP: systolic blood pressure; DBP: diastolic blood pressure; MAP: mean arterial pressure; LDL: low-density lipoprotein; HDL: high-density lipoprotein; TG: triglycerides; GPT: glutamic pyruvic transaminase; Lp-PLA2: lipoprotein-associated phospholipase A2.
Data are shown as mean ± standard deviation or frequency (percentage).
The Lp-PLA2 level (IU/L) according to comorbidity, metabolic syndrome, and weight status in the whole cohort and after stratification by sex.
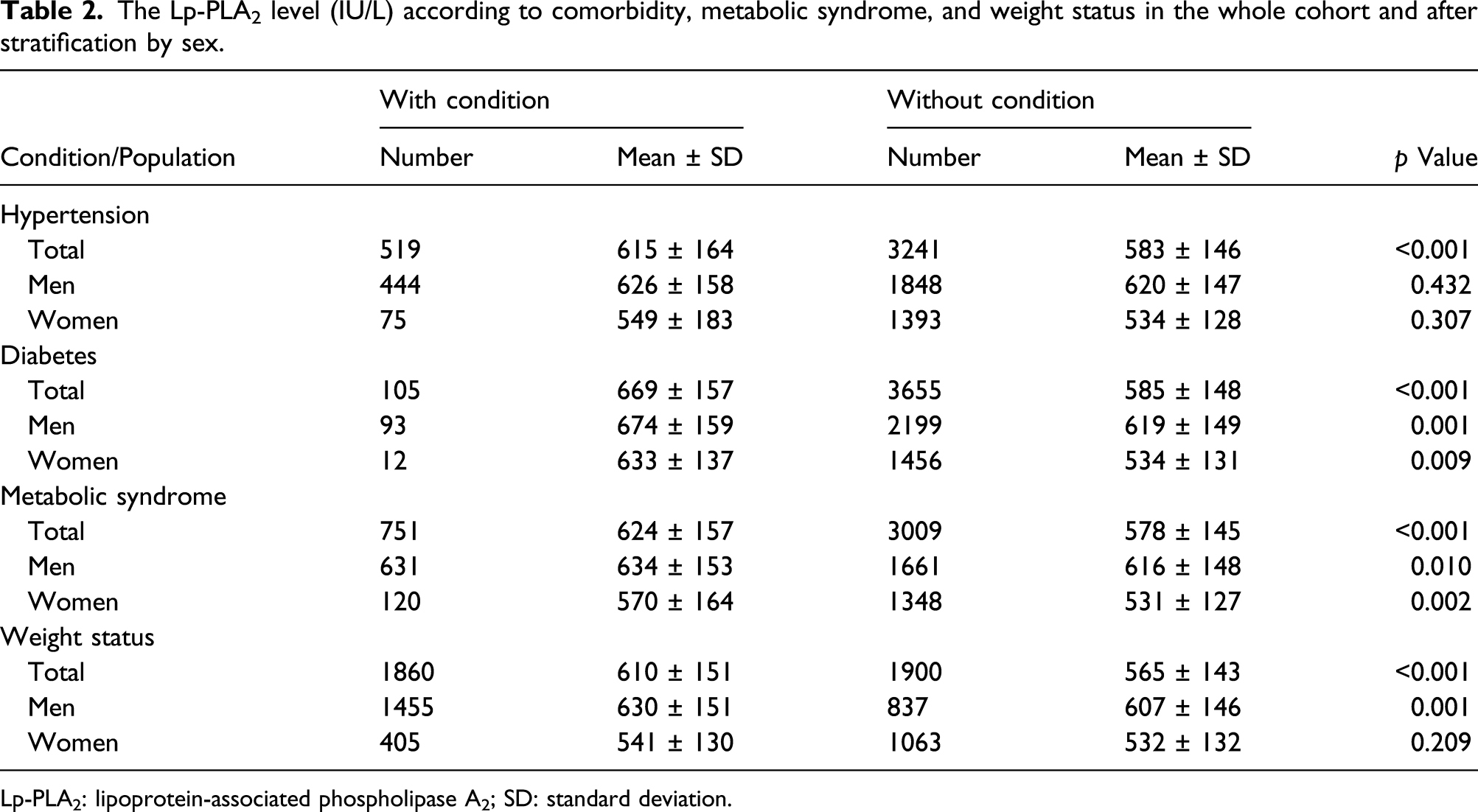
Lp-PLA2: lipoprotein-associated phospholipase A2; SD: standard deviation.
The basic participant characteristics according to overweight type in male and female subjects.

SBP: systolic blood pressure; DBP: diastolic blood pressure; MAP: mean arterial pressure; LDL: low-density lipoprotein; HDL: high-density lipoprotein; TG: triglycerides; GPT: glutamic pyruvic transaminase; Lp-PLA2: lipoprotein-associated phospholipase A2.
Data are shown as mean ± standard deviation; “a” and “b” indicate a significant difference in the central overweight group compared to the normal group and peripheral overweight group, respectively, in the Bonferroni multiple comparison test.
The age-adjusted and LDL-adjusted Lp-PLA2 level (IU/L) according to the comorbidity combination in the whole cohort, after excluding subjects with peripheral overweight and normal weight.

Data are shown as the estimated marginal mean ± standard error derived from the general linear model.
“a,” “b” indicate a significant difference between the DM (−), HTN (−) group and DM (+), HTN (−) group, respectively, in the Bonferroni multiple comparison. Lp-PLA2, Lipoprotein-associated phospholipase A2.
Discussion
This cross-sectional study investigated the association between overweight status and Lp-PLA2 in a population of 2292 men and 1468 women. We evaluated the correlation between Lp-PLA2 levels and risk factors of overweight status, such as hypertension, diabetes mellitus, and MetS, in a Chinese population. The age-adjusted and LDL-adjusted Lp-PLA2 level was significantly higher in the DM (+) and HTN (−) subgroups than in the DM (−), HTN (−), DM (−), and HTN (+) subgroups.
Insulin resistance, a reduction in the rate of glucose disposal caused by a given insulin concentration, often occurs in individuals with obesity or diabetes mellitus, and may develop with aging. 21 This means that the elderly are prone to be more insulin resistance and that Lp-PLA2 levels increase with age. This age-related phenomenon is due to the unavoidable natural aging process and often clusters in certain individuals during aging, 22 which compactible to our results aims at adults less than 50 years of age.
Lp-PLA2 was recently found to be a novel inflammatory biomarker that correlates with several components that contributes to MetS. Since Lp-PLA2 is a vascular-specific inflammation biomarker, measuring Lp-PLA2 levels may be useful for complete evaluation of atherosclerosis in patients with MetS. 23 The adipose tissue located in visceral or intra-abdominal cavities is likely to be infiltrated by macrophages, and this is an important cause of chronic low-grade inflammation with MetS and abdominal obesity. 24 Chronic low-grade inflammation displayed higher Lp-PLA2 activity was observed in patients with MetS. 25 Thus, the presence of elevated Lp-PLA2 activity and MetS may identify high-risk individuals. 26 The results in the study by Noto H et al. suggest that central obesity may contribute to changes in Lp-PLA2 activity in patients with MetS. 27 Lp-PLA2 activity and MetS have shown that abdominal obesity may have been independently responsible for the changes in Lp-PLA2 observed in the study by Gong et al. 28 . However, in our study, we used Lp-PLA2 mass which had stable results and good repeatability rather than Lp-PLA2 activity mentioned above. Since Lp-PLA2 mass concentrations measured by quantitative SISCAPA-mass spectrometry were substantially higher than activity concentrations measured by immunoassay and showed an improved consistency. Lp-PLA2 quantitatively detected by immunoassay appears to be strongly inhibited by interaction of Lp-PLA2 with lipoprotein, 29 which had low sensitivity and easy to be interfered by various components in blood like bilirubin, hemoglobin, chylomicron, fibrinogen, and other lipoproteins. Therefore, we only detect Lp-PLA2 mass by turbidimetric immunology quantitative test in this study.
Lp-PLA2 and its isoforms appear to be heavily influenced by metabolic status, weight, and circulating lipid levels. Patients with type 2 diabetes mellitus who were observed an increase in Lp-PLA2, which appear to be associated with an upregulation in systemic lipids. 15 Moreover, Lp-PLA2 is associated with an unfavorable circulating lipid profile, including increased triacylglycerol and oxidized LDL, which is exacerbated in type 2 diabetes mellitus 30 and produces strong oxidative and inflammatory mediators. 31 In summary, each member of the PLA2 family of enzymes plays a distinct role in generating active lipid metabolites that promote inflammatory metabolic diseases, including oxidative atherosclerosis, hyperlipidemia, diabetes mellitus, and obesity. 32
A total of 3760 subjects were included in the study, of whom 2292 (60.9%) were men. The level of Lp-PLA2 was greater in the male subjects than in female subjects, and Feng et al. reported that the Lp-PLA2 levels showed a statistically significant difference between females and males (t = 4.866, p < 0.001). The reference intervals of serum Lp-PLA2 were 194–640 U/L (18–49 years) and 208–698 U/L (50–88 years) for women and 230–728 U/L for men. 33 In addition, the median Lp-PLA2 levels in men and women in the study by Winkler et al. 34 were 504 U/L and 446 U/L, respectively. The low Lp-PLA2 levels observed in females may result from estrogen secretion, as Lp-PLA2 levels in premenopausal women were lower than those in menopausal women. This estrogen effect was also suggested in a study by Yoshimura et al. 35 which showed a 26% reduction in Lp-PLA2 levels in menopausal females 2 weeks after receiving estrogen replacement therapy. Subjects with central overweight status had a higher Lp-PLA2 level than those with normal weight and peripheral overweight status, in both male and female cohorts. Another prior study of the impact of obesity on Lp-PLA2 found that enzyme activity was positively associated with BMI and that Lp-PLA2 function changes with adolescent obesity. 36 In addition, Lp-PLA2 activity was discovered to be positively associated with BMI (p = 0.004) in the study by Seyfarth et al. 37 . We further evaluated the level of age-adjusted and LDL-adjusted Lp-PLA2 levels according to the combination of hypertension and diabetes mellitus. Our results showed that the age-adjusted and LDL-adjusted Lp-PLA2 level was significantly higher in the DM (+) and HTN (−) subgroups and in those with each condition (namely, DM, HTN, overweight and MetS).
The present study has some limitations. First, this was a cross-sectional study based on routine health examinations of a general population; thus, the results cannot prove a causal relationship between Lp-PLA2 and overweight status. Second, only body weight was measured, and no lean mass body fat percentage, or metabolically healthy obesity were assessed, all of which reflect obese lean mass. Third, our study focused on a physical examination population and may have selection errors due to the inclusion of patients with serious health issues, and thus, may not represent the general population. Last but not least, we used we used Lp-PLA2 mass which had stable results and good repeatability rather than Lp-PLA2 activity. In conclusion, our findings suggest that Lp-PLA2 is associated with central overweight status, diabetes mellitus, hypertension, and MetS in adults less than 50 years of age.
Conclusion
Lp-PLA2 is associated with sex, central overweight status, diabetes mellitus, hypertension, and MetS in adults less than 50 years of age and the age-adjusted and LDL-adjusted Lp-PLA2 was significantly higher in the DM (+) and HTN (−) subgroups than in the DM (−) and HTN (−) and DM (−) and HTN (+) subgroups.
Footnotes
Acknowledgements
We thank the staff in the Health Management Center of Chang Gung Hospital for data collection assistance.
Author Contributions
Y.-H.C. and W.-C.L. analyzed and interpreted the patient data and were major contributors in writing the manuscript. Y.-C.C and W.-C.Y. interpreted the analyzed data. W.Y., H.-Y.H., and X.-X.J. assisted with data collection. Project administration: J.-Y.C., Supervision: J.-Y.C.; Y.-H.C. and W.-C.L. had equal contribution to the present study as co-first authors. J.-Y.C. as corresponding author. All authors read and approved the final paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from Institutional Review Board of Chang-Gung Memorial Hospital (XMCGIRB2020030) and was conducted in accordance with the guidelines laid down in the Declaration of Helsinki in 2013.
Informed consent
The study was approved by Institutional Review Board of Chang-Gung Memorial Hospital (XMCGIRB2020030), so informed consent was not sought for the present study.
Trial registration
The authors declare that no funding was received, so it is not applicable.