
Abstract
Orofacial clefts are common congenital defects whose prevalence differs between geographical regions and ethnic groups. The inheritance is complex, involving the contribution of both genetic and environmental factors. The involvement of genes belonging to the folate pathway is still matter of debate, with strong evidences of association and conflicting results. After demonstrating the contribution, for a sample from the Italian population, of common mutations mapping on three genes of the folate pathway, our group tried to unravel their contribution in independent sample studies with different ethnicity. In the present investigation a set of 34 triads with oral cleft from Nassiriya, Iraq, has been genotyped for rs1801133 of MTHFR, rs1801198 of TCN2, and rs4920037 of CBS polymorphisms. Association analysis evidenced a decreased risk of cleft for children carrying the 667G allele at TCN2 gene (P = 0.02). This evidence further supported the relationship between polymorphisms of folate related genes and oral clefts, and outlined the relevance of studying populations having different ethnicity.
Introduction
Embryogenesis is a delicate process, which involves a succession of steps with a perfect timing of activation/inhibition of gene expression and pathways’ contribution. Every perturbation in this intricate network of signaling/factors from genetics or from environment can result in a congenital defect. Neural tube defects could be, at least partially (70%) prevented by administration of folic acid (4 mg/day) during periconceptional period. 1 In fact, folate metabolism plays a pivotal role during early stages of embryo development and, over the years, great efforts have been spent to try to elucidate its role. Recently, De-Regil’s et al. 2 group reviewed literature with the aim of assessing whether periconceptional oral folate supplementation, besides neural tube defect, could prevent other birth defects; but as regard of clefting, no certain conclusions were obtained. However, based on evidences of an effective correlation, in the last few decades, researchers spent much energy with the aim to unravel whether the preventive effect of folate supplementation can be due to a compensation of some impaired activities of folate-related gene products. In particular, studies have been focused on genes of methionine and one-carbon pathways and their potential relationship with orofacial clefts (OFCs).
Among OFCs, cleft of the lip with or without cleft palate (CL/P) is the most common, with a prevalence close to one per 1000 at birth, 3 while cleft of the palate only (CPO) is rarer, ranging from 1 to 25 per 10,000 newborns. 4 The prevalence of both forms of cleft varies depending on ethnic origin.5,6 OFC arises from a combination of genetic and environmental factors. For instance, folate deficiency, possibly caused both by insufficient dietary intake and by missense mutations at methylenetetrahydrofolate reductase (MTHFR) gene, responsible for its metabolism, results in elevated homocysteine levels. Maternal hyperhomocysteinemia has been demonstrated being a risk factor for having offspring with nonsyndromic orofacial cleft (nsOFC). 7 A recent meta-analysis 8 confirmed a significant association between MTHFR C677T polymorphism and nsOFC. Other genes involved in folate pathway have been seen associated with an increased risk of cleft occurrence. Among these, besides MTHFR, transcobalamin 2 (TCN2), and cystathionine beta-synthase (CBS). Our group found association for all of them in an Italian sample of nonsyndromic cleft of the lip with or without cleft palate (nsCL/P).9 –11 Then, in order to verify the involvement of the same three polymorphisms (rs1801133 of MTHFR, rs1801198 of TCN2, and rs4920037 of CBS), our group investigated an independent sample of different ancestries, however with discordant results. 12 In fact, 677T allele of MTHFR gene seemed to decrease the cleft risk when considering child genotype, in the Asian population genotyped for those polymorphisms.
In the present work, an additional independent sample study, from Nassiriya, Iraq, has been investigated for the three polymorphisms above mentioned, with the aim to unravel the complexity of genetic contributions to cleft, considering ethnic and geographical differences.
Materials and methods
Sample study
This family based association study was performed with 34 nsOFC patient–parents triads enrolled at Nassiriya, Iraq, and having Arabian ethnicity and ancestry from that region. The sample study included 29 nsCL/P and five nsCPO triads. The ratio of male to female in probands was 1:1.13. A team of clinicians performed the OFC diagnosis and excluded additional birth malformation or metabolic diseases. A detailed interview excluded families whom may be subjected to know or suspected clefting agents, such as phenytoin, warfarin, ethanol, and smoking. Three enrolled family was excluded because they did not meet one or more described criteria. The study was approved by the local ethics committees, and it complied with the Helsinki Declaration’s Ethical Principles for Medical Research Involving Human Subjects. Written informed consent was obtained from all patients and parents. Peripheral venous blood samples (4 ml) were collected and conserved in ethylenediaminetetraacetic acid (EDTA). Then, DNA was extracted using the GenElute™ Blood Genomic DNA Kit (Sigma) and quantified by a Nanodrop spectrophotometer (Thermo Scientific).
Genotyping
Three single nucleotide polymorphisms (SNPs) were analyzed in the study. These common variants map on three genes of the folate pathway previously found associated with nsCL/P: the rs1801133, rs1801198, and rs4920037 of the MTHFR, TCN2, and CBS, respectively. Genotyping of patients and parents was performed by specific TaqMan SNP genotyping assays (assay-on-demand ID: C___1202883_20, C___325467_10, and C___1605440_1) with a 7500 Sequence Detection System (Life Technologies) following the manufacturer’s protocol.
Statistical analysis
The Hardy–Weinberg equilibrium for genotype distribution, in both proband and parent groups, was examined using Pearson’s χ2 test with a significance threshold of P < 0.05.
Association analysis was performed on a Microsoft Windows platform by the PLINK v1.07 software. 13 The family based association analysis was performed by the transmission disequilibrium test (TDT) that examined allele transmission from heterozygous parents to the affected probands. 14 The odds ratio (OR) was used to evaluate the level of association; this corresponds to the ratio M1/M2, where M1 denotes the number of transmissions of the reference allele from heterozygous parents to affected offspring and M2 the number of times that the allele was not transmitted. 15
Family based association was analyzed with the whole sample to maximize the power of the study. Then, the nsCL/P and nsCPO samples were analyzed separately in order to avoid that genetic heterogeneity could mask association signals.
Results
Three common polymorphisms of folate pathway genes were investigated for association with nsOFC in a sample of the Iraqi population. The quality control of genotyping process approved the molecular data, indeed no Mendelian errors were detected and patients and parents genotype frequencies respected the Hardy–Weinberg equilibrium law.
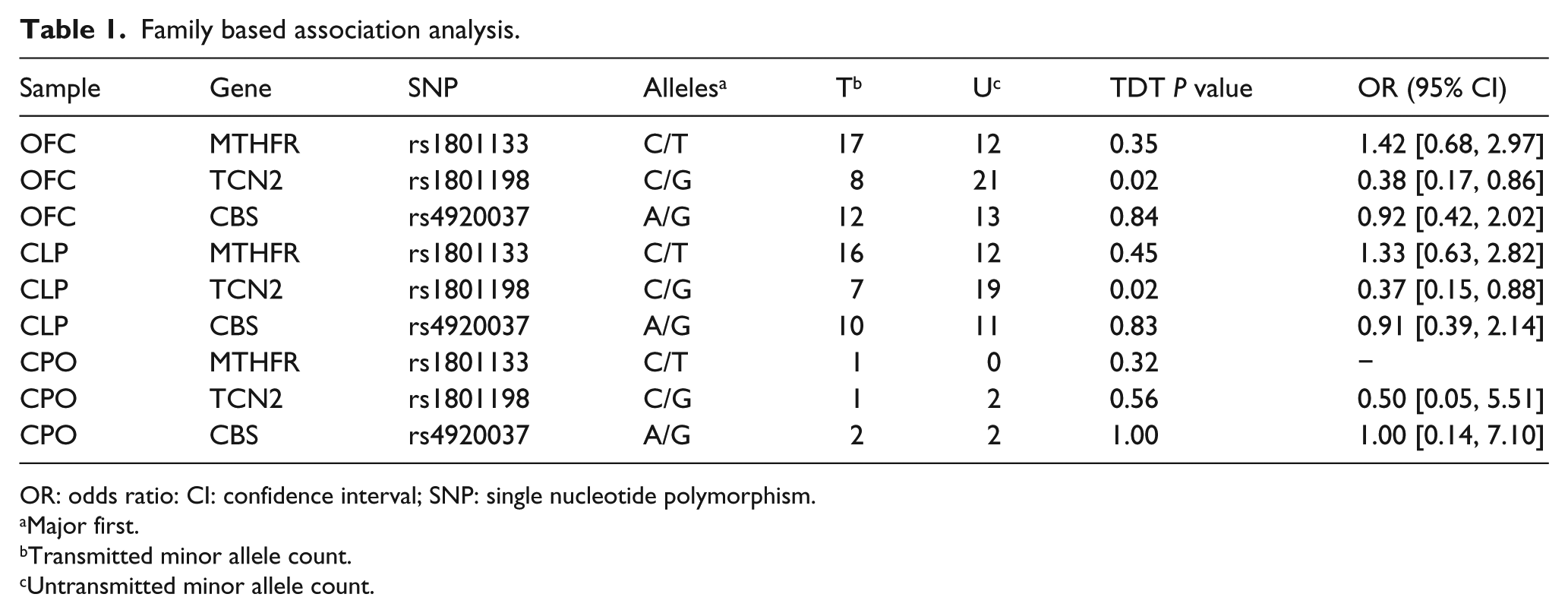
The TDT used to perform family based association study showed that the alleles of MTHFR and CBS were transmitted from heterozygous parents to patients accordingly with the Mendelian expectation, indicating no association with the malformations (Table 1). On the other hand, the variant allele of TCN2 rs1801198 was significantly undertransmitted to OFC patients (P = 0.02). The minor allele rs1801198-G of TCN2 reduced the risk of OFC, with a calculated OR of 0.38 (95% CI = [0.17, 0.86]). Evidence of association with TCN2 was confirmed for the nsCL/P group alone, but not for nsCPO, although this could be related to the small sample size.
Family based association analysis.
OR: odds ratio: CI: confidence interval; SNP: single nucleotide polymorphism.
Major first.
Transmitted minor allele count.
Untransmitted minor allele count.
Discussion
Folate role in processes leading to the face morphology during early embryo development is still matter of debate. The observation that maternal use of folate antagonists strongly increases the risk of OFCs has endorsed the hypothesis that folate-related metabolism and correlated genes may be involved in the oral cleft etiology. 16 Many attempts have been made in order to shed light on potential involvement of genes implicated in folate metabolism, although, they have not always led to the same conclusions. 17 Our group contributed to the cause with findings supporting association with cleft for at least three genes, namely MTHFR, CBS, and TCN2.9 –11 However, due to the genetic heterogeneity and geographic variation in prevalence, the validation of association data needs to be confirmed in independent sample studies, with different ancestry and ethnicity.
The present study aimed to verify the involvement of three folate-related genes in OFC onset in a sample study from Iraq. A family based association study was carried out with 34 OFC cases recruited in Nassiriya. The association between rs1801133 at MTHFR and cleft was not confirmed in Iraqi sample, despite a number of studies reporting correlation. 8 In this regard, Rai 8 carried out a meta-analysis on 76 studies investigating the MTHFR polymorphism rs1801133, also named C677T, in patients with nsCL/P. The author subgrouped the analysis taking into account the ethnicity of sample studies enrolled from 14 different countries for the 22 eligible, and he found a strong association adopting different models. CBS polymorphisms have been less investigated than MTHFR and in the literature, few manuscripts are available. In particular, the polymorphism rs4920037 was genotyped by Goffinet et al. 18 with no evidence of association, and by our group, finding a significant association in an Italian population, 11 not confirmed with an Asian sample study. 12 In the present study, we genotyped the same polymorphism that emerged nonassociated with OFC in the Iraqi sample.
Finally, the rare allele at rs1801198 (G) of TCN2 was significantly undertransmitted to both OFC and CLP probands, appearing as a protective genetic factor in this population. Interestingly, Marini et al. 19 reported that the same TCN2 allele increased the risk for affected offspring in Californian women with low folate intake. Even in the Italian population investigated by our group, the rs1801198 variant increased the risk of cleft. 10 This may indicate the rs1801198-G as neutral polymorphism reporting the effect of a still unrecognized causative variant.
This finding confirms the variability of the genetic causes among different populations worldwide, making further validations for candidate genes involvement necessary.
Footnotes
Acknowledgements
We are indebted to the families participating in the study for their invaluable contribution, as well as to all the personnel involved in clinical data and specimen collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.