
Abstract
Background
Sacroiliac joint (SIJ) disorders are among the most common causes of chronic low back pain. Imaging-guided SIJ injections are widely used as an early diagnostic tool, with corticosteroid often added to provide a therapeutic component. Evidence of factors predicting the therapeutic outcome of these injections remains scarce.
Purpose
To evaluate the effect of SIJ osteoarthritis and other potentially relevant demographic, imaging, and procedural factors on the patient-reported therapeutic outcome of imaging-guided SIJ injection.
Material and methods
This retrospective single-center study included 101 patients who underwent specialist-referred imaging-guided SIJ injection between 2010 and 2023. Medical records and procedural reports were reviewed to collect relevant patient information, and associated SIJ MRIs and CT scans were reanalyzed for osteoarthritis, sacroiliitis, and bone marrow edema by an experienced musculoskeletal radiologist. The association of demographic, imaging, and procedural factors with the therapeutic injection outcome was assessed using logistic regression modeling.
Results
Of 101 patients who underwent an imaging-guided SIJ injection, 72 (71.3%) met the inclusion criteria. The mean age was 52.2 (SD 14.2) years, and 30 patients (41.7%) achieved a positive therapeutic response. Increasing age was significantly associated with a lower likelihood of a positive outcome, with the probability decreasing on average by 9.4% for each additional year of age (OR 0.91 [95% CI 0.84–0.99]). Neither SIJ osteoarthritis grade nor other demographic, imaging, or procedural factors showed a significant association with injection outcome.
Conclusion
Increasing age was significantly associated with a lower likelihood of achieving a positive therapeutic SIJ injection outcome, while SIJ osteoarthritis grade showed no association.
Introduction
The sacroiliac joints (SIJs) are two specialized weight-bearing joints between the sacrum and the ilium, usually formed within sacral segments S1–S3. SIJs are complex structures that continue their development in the first decades of life and undergo many physiological changes during life, for example, in pregnancy and aging. 1 The SIJ is syndesmotic in its posterosuperior area with the rest of the joint (approximately two-thirds) being a true synovial joint. 2 Further structural and biomechanical stability is provided by multiple adjacent ligamentous and muscular structures. 3 The SIJs receive complex and abundant innervation from the ventral and dorsal lumbosacral nerve roots,3–7 and connections exist between SIJs and adjacent neural structures, such as L5 epineural sheath and the lumbosacral plexus. 7
The SIJ is a recognized source of low back pain (LBP), and pain originating from it is commonly referred to as SIJ dysfunction, which may occasionally be accompanied by radiculopathy. The prevalence of SIJ dysfunction is frequently cited to range between 15% and 30% among LBP patients,3,8 positioning it as one of the leading causes of chronic LBP. Among intra-articular etiologies of SIJ dysfunction, osteoarthritis and spondyloarthropathy are considered the most prevalent. 3 Extra-articular etiologies are also recognized. Although the presence of multiple positive SIJ provocation tests may serve as a clinical indicator of SIJ-related pain, SIJ injections are regarded as an early-stage confirmatory tool.3,9 In addition to anesthetic agents used for diagnostic purposes, corticosteroids may be added to the injectate to potentially prolong the therapeutic effect, thereby introducing a therapeutical component to the procedure. 10
A prospective case series study demonstrated that among non-spondyloarthropathy patients with SIJ dysfunction confirmed rigorously by diagnostic SIJ injections, approximately one-third did not show a therapeutic response to corticosteroid SIJ injection. 11 This finding suggests that certain clinical or radiological factors may influence the therapeutic outcome and could serve as clinically significant biomarkers. However, to date, very few studies have systematically investigated the potential predictors of treatment success following therapeutic SIJ injections. The present study aims to evaluate the most common clinical and radiological factors that may affect the efficacy of imaging-guided therapeutic SIJ injections.
Materials and methods
This retrospective single-center study included all patients who underwent an imaging-guided SIJ injection at Oulu University Hospital between 2010 and 2023. The study was approved by the regional medical research ethics committee of the Wellbeing Services County of North Ostrobothnia (approval number 226/2023), and the requirement for informed consent and ethics committee approval were waived. The study was carried out in accordance with the Declaration of Helsinki, and patient consent for publication of clinical images was obtained. Patients were referred for the procedure based on clinical suspicion of SIJ dysfunction, as determined by the referring specialist physician through clinical testing and magnetic resonance imaging (MRI) and/or computed tomography (CT) evaluation. For this study, patients were identified from the local PACS using the SIJ injection procedure code. Study exclusion criteria were: (1) a history of major pelvic trauma or other competing sources of pelvic pain (e.g., deformity not attributable to typical SIJ anatomical variations 12 or degenerative/inflammatory SIJ changes, or malignancy), (2) prior SIJ surgery, (3) absence of relevant imaging data (MRI or CT) within 1 year of the injection, (4) bilateral SIJ injections or concurrent injections at other anatomical sites (e.g., nerve root), and (5) lack of explicit documentation in the local electronic medical records regarding the therapeutic outcome of the injection.
Medical records were reviewed to collect clinical data, including age, sex, body mass index (BMI, recorded within 2 years of the injection), and whether SIJ arthrodesis was performed following the injection. A board-certified fellowship-trained musculoskeletal radiologist with 11 years of experience evaluated the available associated MRI and/or CT scans for signs of SIJ osteoarthritis in all patients, and for sacroiliitis and SIJ bone marrow edema (BME) in the majority of patients with MRI data (65/72 [90.3%]), blinded to patient demographic and therapeutic outcome data. SIJ osteoarthritis was graded as none, mild (with small osteophytes and/or mild joint space narrowing), moderate (with distinct osteophytes and/or joint space narrowing and/or subchondral bone marrow edema), or severe (advanced progression of the same osteoarthritis changes resulting in SIJ destruction). In cases where MRI and CT scans were available with conflicting osteoarthritis grades, the higher grade was used for analysis. Active sacroiliitis was defined as the presence of active inflammation on MRI, characterized by periarticular BME that is considered highly suggestive of sacroiliitis. Chronic sacroiliitis was defined as the presence of structural lesions such as fat metaplasia, subchondral sclerosis, erosions, or ankylosis, which do not meet the MRI definition of active sacroiliitis but are regarded as chronic changes.13,14 Cases demonstrating both active inflammation and chronic structural lesions were recorded as having concurrent active and chronic features.
All SIJ injections were performed using a routine posterior approach with the patient in the prone position by board-certified musculoskeletal radiologists or musculoskeletal radiology fellows. Fluoroscopy was used for image guidance, and cone-beam CT (CBCT) was employed when necessary to assist with needle placement (Figure 1), using Philips Allura Xper FD 20 (Koninklijke Philips N.V., Amsterdam, the Netherlands). The procedure was performed in a sterile fashion. After local anesthesia of the skin and subcutaneous layers with 5–10 mL of 10 mg/mL lidocaine, a 21-gauge Chiba needle was advanced into the inferior third of the SIJ with either fluoroscopic and/or CBCT guidance. In fluoroscopy-guided procedures, the correct intra-articular needle position was confirmed by contrast agent injection. A hand-operated Luer-lock syringe without pressure control was used to inject a target volume of 2 mL of a 1:1 mixture of methylprednisolone 40 mg/mL and ropivacaine 2 mg/mL, without significant injection resistance. Procedural equipment was in active use, underwent scheduled maintenance, was also used for other procedures, and was not replaced during the study period. Injection-related details were extracted from procedural reports and included the composition of the injectate, the imaging modality used, the needle position as assessed from intraoperative images (i.e., evidence of arthrogram), and the volume of the injectate. The therapeutic response to the SIJ injection, defined as significant patient-reported pain relief lasting at least 1 week after the injection,
10
was collected from the electronic medical records and served as the primary outcome of the study. A 1-week post-procedural outcome assessment is routinely performed at our hospital for SIJ injections and is documented in the electronic medical records, and therefore this time point was selected for the study. (a) CBCT image (prone) shows the injection needle (white arrow) in the sacroiliac joint space. As the CT image confirms the correct needle location, contrast agent is not needed. (b) Fluoroscopic image obtained during a sacroiliac joint injection shows the placement of the injection needle (white arrow) in the inferior aspect of the sacroiliac joint. Injected contrast agent is seen as a linear opacity (white arrowheads) away from the injection needle tip in the sacroiliac joint, confirming intra-articular needle position. Patient consent for publication was obtained. S: sacrum; I: ilium.
All demographic, procedural, and radiologic data were assessed for normality using visual inspection and the Shapiro–Wilk test. Data were presented as means ± standard deviations (SDs) for normally distributed continuous variables, medians with interquartile ranges (IQRs) for non-normally distributed continuous variables, and frequencies with percentages for categorical variables. Group comparisons between patients with positive and negative therapeutic outcomes following SIJ injection were performed using Student’s t-test for normally distributed continuous variables, Mann–Whitney U test for non-normally distributed continuous variables, and chi-squared test for dichotomous variables. A logistic regression model was fitted to evaluate the association between SIJ osteoarthritis grade and other potential demographic, imaging, and procedural factors with the therapeutic response to the SIJ injection. SIJ osteoarthritis grades were dichotomized into two categories: none/mild and moderate/severe. The additional variables included in the logistic regression analysis were sex, age, BMI, imaging modality used for SIJ osteoarthritis assessment, injectate composition, and intraoperative imaging modality. The overall occurrence of sacroiliitis was very low (3/65 [4.6%] among patients with evaluable MRI data), and therefore it was not included in further analyses. Likewise, the distribution of SIJ BME prevalence was highly congruent with the none/mild and moderate/severe osteoarthritis grades (0/38 [0%] and 25/27 [92.6%], respectively, among patients with MRI data available). Thus, BME was not included in the statistical modeling. Results were reported as estimates with standard errors, and odds ratios (OR) with 95% confidence intervals (CI). Statistical analyses were conducted using IBM SPSS Statistics, version 29.0.0.0 (IMB Corp, Armonk, NY), and a p-value <.05 was considered statistically significant.
Results
Of the 101 patients who underwent an SIJ injection during the study period, 29 (28.7%) were excluded for reasons detailed in Figure 2. Consequently, 72 (71.3%) patients who underwent the procedure were included in the analysis, with a mean age of 52.2 (SD 14.2) years and a male-to-female ratio of 17 to 55 (23.6%/76.4%). No statistically significant differences in baseline demographics were observed between patients with a positive versus negative therapeutic response to the injection (Table 1). Study flowchart with exclusion details. SIJ; sacroiliac joint. Demographic and clinical characteristics of the total study population and subgroups by therapeutic outcome. aIf both MRI and CT were available with discordant osteoarthritis grades, the higher grade was included in the analysis. bCT or intraoperative CBCT. BMI; body mass index, CBCT; cone-beam computed tomography, CT; computed tomography, MRI; magnetic resonance imaging, SIJ; sacroiliac joint.

The majority of patients (N = 65; 90.3%) had MRI scans available for analysis, of which 49 (75.4%) also had accompanying CT images. Seven patients (9.7%) had only CT images available. In total, 40 patients (55.6%) demonstrated none or mild SIJ osteoarthritis, while 32 patients (44.4%) showed moderate or severe osteoarthritis findings. Sacroiliitis was rare in this cohort, with only three patients (4.2%) exhibiting chronic sacroiliitis. The imaging modalities and findings are summarized in Table 1.
Procedural characteristics of the total study population and subgroups by therapeutic outcome.
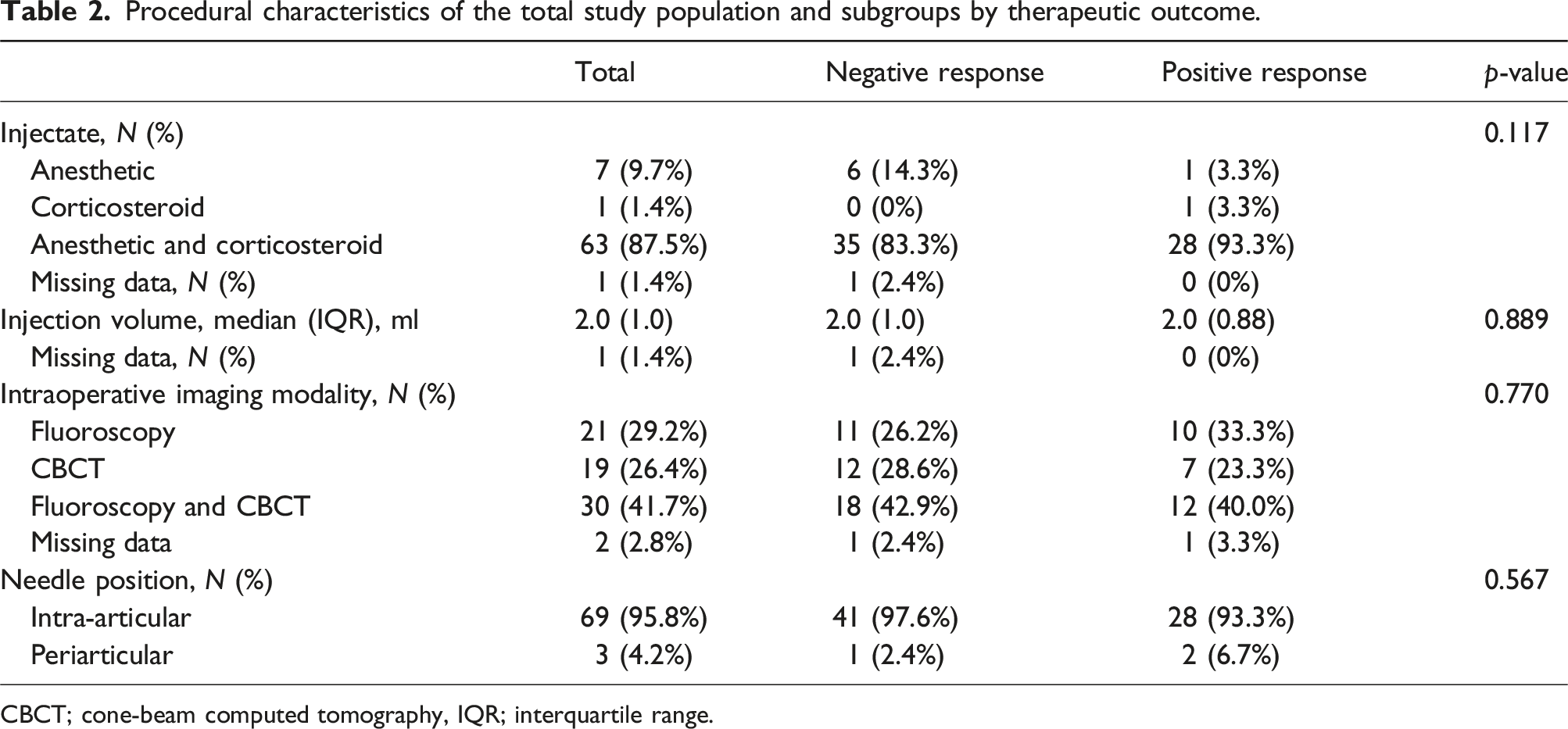
CBCT; cone-beam computed tomography, IQR; interquartile range.
Multivariate logistic regression analysis of factors associated with therapeutic SIJ injection outcome.
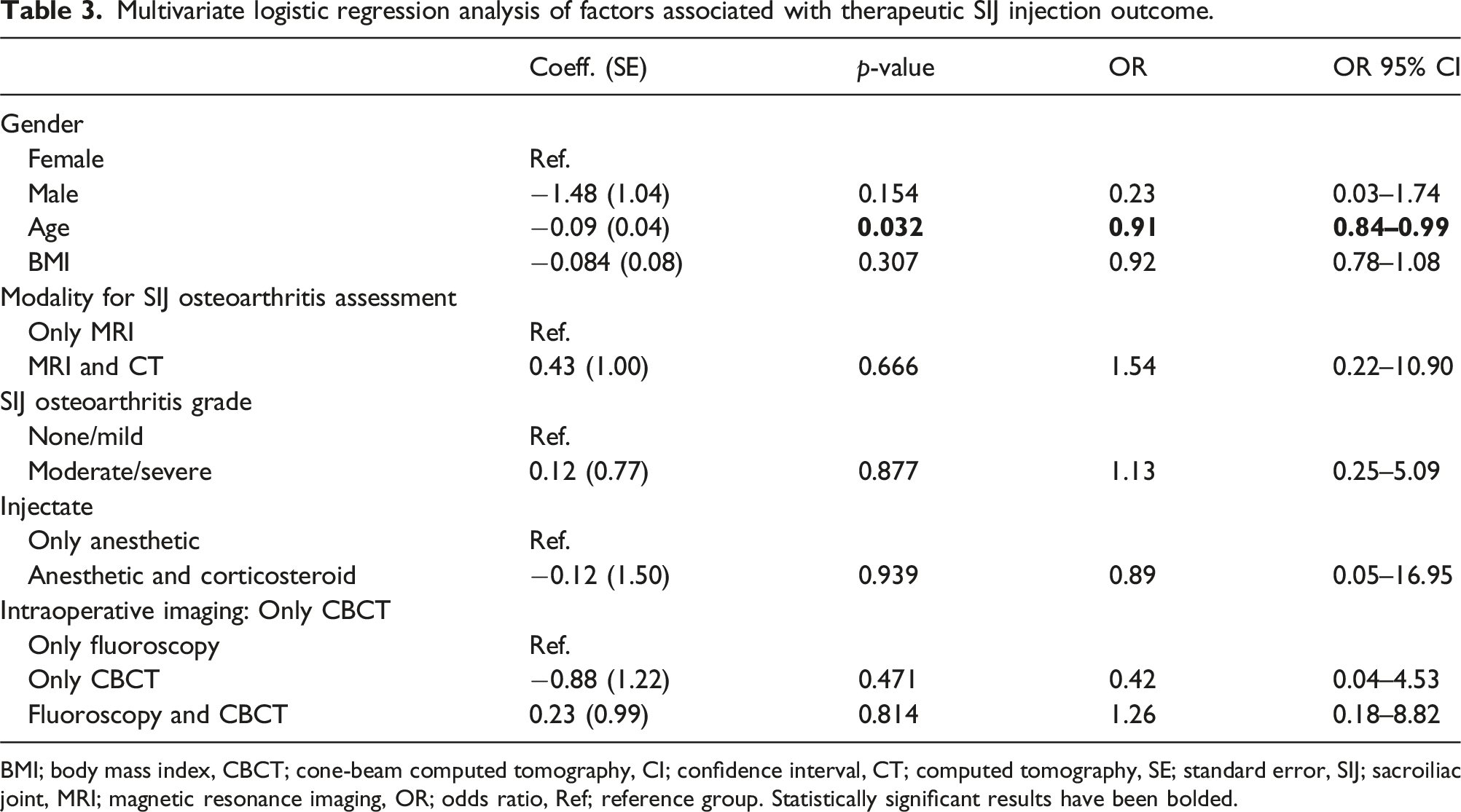
BMI; body mass index, CBCT; cone-beam computed tomography, CI; confidence interval, CT; computed tomography, SE; standard error, SIJ; sacroiliac joint, MRI; magnetic resonance imaging, OR; odds ratio, Ref; reference group. Statistically significant results have been bolded.
Discussion
The primary aim of this study was to evaluate the impact of SIJ osteoarthritis on the therapeutic outcome of SIJ injection, defined as significant pain relief at 1 week, in a retrospective cohort of patients with clinically suspected SIJ dysfunction. In addition, the influence of other potentially relevant demographic, imaging, and procedural factors on injection response was analyzed. The analysis revealed no association between SIJ osteoarthritis grade and the therapeutic injection outcome. Among the other factors, age was the only significant predictor, with increasing age associated with a higher probability of a negative injection outcome. These findings suggest that radiologic evidence of SIJ osteoarthritis alone may not be a reliable predictor of short-term therapeutic response to SIJ injection in patients with SIJ dysfunction.
Earlier evidence on the association between radiologic SIJ osteoarthritis changes and the outcome of therapeutic SIJ injection is scarce. Savran Sahin et al. reported that short-term response to a combined corticosteroid and anesthetic SIJ injection does not differ between patients with low-grade and high-grade osteoarthritis, which is in line with the findings of the present study. 15 Together, these findings support earlier research indicating that degenerative SIJ changes, such as joint space narrowing and osteophyte formation, are commonly observed in asymptomatic individuals and are not more prevalent or advanced in patients with clinically suspected SIJ dysfunction compared to asymptomatic controls.16,17 Eno et al. reported that among asymptomatic individuals with a mean age comparable to that of the present cohort, approximately one-third exhibited greater than mild radiologic SIJ osteoarthritis changes, and 68% showed some degree of degeneration in at least one SIJ. 16 Taken together with prior studies, our results from this symptomatic cohort are consistent with the view that radiologic SIJ osteoarthritis changes may often reflect age-related asymptomatic degeneration rather than serving as reliable biomarkers for SIJ therapeutic injection outcome.
The SIJ injections in the present study were almost exclusively intra-articular. While our data do not directly identify the anatomic pain source, the lack of an association between SIJ osteoarthritis grade and short-term therapeutic injection response, together with the very low occurrence of sacroiliitis, suggests that the presence of the most common intra-articular pain sources may be insufficient to explain treatment response among symptomatic SIJ dysfunction patients. This interpretation is supported by the study by Borowsky et al., who investigated patients with persistent SIJ region pain treated with either a standard intra-articular injection or a novel technique combining intra-articular and extra-articular injections targeting the posterior sacroiliac ligaments and the lateral branches of the S1–S3 spinal nerves. 18 The novel approach resulted in a significantly higher rate of positive response at 3 weeks, defined as a reduction in pain of 50% or more, compared to the standard intra-articular method (42.5% vs 27.5%, respectively). Although statistical significance is far from demonstrated, two of the three extra-articular injections in the present study population yielded positive patient-reported benefit at the 1-week mark. Overall, our findings raise the possibility that extra-articular contributors may be involved in some patients, although our study did not directly assess these structures.
A number of patients in the present cohort may also have had a more distant pain etiology, despite clinical findings suggestive of SIJ-related pain that led to the decision to request an SIJ injection. In a recent retrospective study, DePhillipo et al. analyzed the final diagnoses of 124 patients, most of whom reported chronic symptoms at baseline, after a mean follow-up of 2.4 years. 19 These patients had initially identified the SIJ as their primary pain source, defined as contributing to at least 50% of the overall pain. The assessed pain sources included the lumbar spine (discogenic or facetogenic pain), SIJ, and hip joints, evaluated through clinical examination, imaging, and diagnostic anesthetic injections. Ultimately, only seven patients (5.6%) were diagnosed with SIJ-originated pain. The most common final diagnosis was LBP, with discogenic pain identified in 75 patients (60.5%). Although our study did not directly evaluate possible extra-articular pain generators, these findings highlight the diagnostic complexity of SIJ region pain and the potential for radiologic SIJ osteoarthritis findings to be clinically insignificant.
Indeed, in the age distribution of the present study, these distant pain generators are more prevalent with increasing age. This well-established association may explain the higher probability of a negative injection outcome among older patients. Specifically, the point prevalence of LBP increases steadily with age, peaking in the eighth decade, while lumbar spine degenerative changes follow a similar trend and have been linked to LBP within the age range of the present cohort.20–22 Likewise, the prevalence of hip osteoarthritis peaks in the sixth decade, with associated disability continuing to rise across the age spectrum. 23
Several limitations are inherent to this study. First, the retrospective design restricted the availability and consistency of data; most importantly, pain NRS values or other standardized outcome measures for the therapeutic injection outcome were not routinely documented in the procedural or medical records, resulting in reliance on more subjective descriptions of treatment response. Second, the distribution of SIJ osteoarthritis grades largely lacked cases at the extremes (none and severe), which may have limited the statistical power of the analysis. Third, the osteoarthritis grading system was designed to be applicable across both MRI and CT to preserve clinical transferability, and therefore a deeper analysis of more localized SIJ imaging features was not possible. Fourth, the study focused solely on the therapeutic outcome of SIJ injections; including an assessment of diagnostic anesthetic responses could have provided a more comprehensive evaluation of the clinical relevance of SIJ osteoarthritis and other contributing factors.
In conclusion, among patients with clinically suspected SIJ dysfunction severe enough to warrant injection-based evaluation, increasing age was significantly associated with a lower probability of achieving a positive therapeutic SIJ injection outcome, while SIJ radiologic osteoarthritis grade showed no predictive value. Further prospective studies are needed to find positive and negative predictive prognostic factors for the SIJ injection outcome.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data available on reasonable request from the authors.