
Abstract
Fetal magnetic resonance imaging (MRI) has become a valuable noninvasive method for evaluating congenital anomalies of the fetus and can serve as an important adjunct to the prenatal ultrasound, particularly where the ultrasound is unable to exclude or detect fetal abnormalities. This pictorial review will describe the utilization of three-dimensional fast imaging employing steady-state acquisition (3D-FIESTA) in various clinical entities, specifically at 3T, and how to generate clinically valuable information.
Keywords
Introduction
Fetal magnetic resonance imaging (MRI) has become a valuable noninvasive method for evaluating congenital anomalies of the fetus and can serve as an important adjunct to the prenatal ultrasound, particularly where the ultrasound is unable to exclude or detect fetal abnormalities. Fetal MRI enhances diagnostic confidence and accuracy, which also provides reliable clinical information.1–3 However, MRI has known susceptibility to motion artifacts, which is challenging for fetal MRI. While other sequences have been incorporated, Single-shot T2-weighted (SST2W) sequence is the predominantly utilized sequence for fetal MRI examinations. 4 Additional sequences used in standard fetal MRI assessment include: 2D steady-state free precession, spoiled gradient echo T1, diffusion-weighted imaging, and susceptibility weighted imaging for body imaging. Fetal brain studies incorporating a wider variety of MRI techniques have been reported over the past decade,5–9 while use in other anatomic areas have been less reviewed. 3
Three-dimensional fast imaging employing steady-state acquisition (3D-FIESTA, General Electric Healthcare, Waukesha, WI USA) provides high spatial resolution and excellent details based on the T2-T1 ratio of the tissues. Although 3D-FIESTA has been introduced for assessing fetal brain anatomy and pathology, 9 the diagnostic utility for further fetal congenital anomalies is less well described. The 3D-FIESTA sequence in fetal body MRI offers several advantages, including excellent tissue contrast, a large field of view, and multiplanar imaging capabilities. This technique is useful for evaluating fetal position, fetal ossification (e.g., skull and thoracic cage), as well as in complicated conditions such as oligohydramnios, maternal obesity, and the presence of bowel gas artifacts. However, there are significant limitations to the use of 3D-FIESTA in fetal body imaging. These include susceptibility to motion artifacts, prolonged acquisition time, and limited availability in clinical practice.
3D-FIESTA fetal imaging can be performed using both 1.5T and 3T MRI systems; however, significant differences exist between the two field strengths. A study by Victoria, et al demonstrated higher scores for visualization of fetal anatomic structures in fetuses images at 3T versus 1.5T. 10 Nonetheless, 1.5T MRI remains the more commonly utilized modality at present. 11 Although 3T MRI has higher signal-to-noise ratio and spatial resolution, fetal 1.5 and 3T MRI examinations were found to have equivalent specific absorption rate (SAR) and specific energy dose (SED) in one study. 12 In addition, 3T MRI is more susceptible to motion and fluid-wave-related artifacts yet diagnostic interpretation is not limited. 10
This review focuses on 3D-FIESTA imaging applied to fetal body MRI examinations, specifically at 3T, and how to generate clinically valuable information. We believe this may be of value for institutions such as ours that have only 3T magnets available at their sites.
MR protocol
Example sequence parameters for fetal MRI.

MRI: magnetic resonance imaging, 3D-FIESTA: three-dimensional fast imaging employing steady-state acquisition, FOV: field of view, mm: millimeters, TR: repetition time, TE: time to echo, ms: milliseconds, Hz: Hertz, s: seconds.
Different MRI manufacturers implement variations of the balanced steady-state free precession (SSFP) sequence under different commercial names, with minor differences in protocol parameters. These include FIESTA by GE Healthcare, TrueFISP by Siemens Healthineers, and Balanced FFE (Fast Field Echo) by Philips Healthcare. Protocol parameters may vary; for example, the Field of View (FOV) commonly ranges from 300 to 400 mm to cover the entire fetal body, but can be reduced for targeted imaging of smaller anatomical regions.
Spectrum of anomalies
Chest anomalies
MRI plays a crucial role in evaluating congenital diseases that affect fetal lung, which appears hyperintense on T2W images. 13 In addition, fetal MRI allows the evaluation to assess the extent of the associated disorders with the remaining normal lung parenchyma. 14 Total fetal lung volumes can be calculated in MRI, which is more accurate compared to ultrasound and helps predict the prognosis of the fetus. 15 MRI provides salient information for prenatal counseling, delivery team plan, and postnatal care with respect to chest anomalies. 14
Congenital high airway obstruction sequence (CHAOS)
Congenital high airway obstruction sequence is an extremely rare congenital anomaly with characteristic imaging features, consisting of enlarged lungs, flattened or inverted diaphragms, and hydrops fetalis.
16
This pathology increases perinatal morbidity and mortality rates of the fetus which is life-threatening without fetal intervention.
17
MRI findings in fetuses with this condition dilated airway, enlarged lung volumes, hyperintense T2 lung signal, flattened or inverted diaphragms, and ascites. 3D-FIESTA offers better visualization of the airway structures and anatomical details (Fig. 1). Ex utero intrapartum treatment (EXIT) procedure to secure and stabilize airway in fetuses has been reported in several studies.17–21 MRI assesses more information of the fetus with a large field of view, which can be utilized for fetal surgical intervention planning.
22
Sagittal (a, b) and coronal (c) 3D-FIESTA on 3T MRI showing a fetus with congenital high airway obstruction sequence (CHAOS). The fetus has dilated airway (black arrow), markedly enlarged lung volumes with increased signal (L), inverted diaphragms (white arrow), and marked ascites (A).
Congenital diaphragmatic hernia (CDH)
CDH is a rare congenital anomaly that affects the fetal lung, causing pulmonary hypoplasia and pulmonary hypertension, with an incidence of 1:3,000. 13 There is a wide range of mortality rates in patients with CDH based on severity of the disease, from 10% in mild degree to more than 90% in the most severe degree. Additionally, morbidity rates increase in neonates with CDH.13,23,24 Fetal MRI is a key imaging in evaluating lung volume, assessing anatomical structures, and predicting prognosis of the fetus. 3D sequences may potentially provide higher accuracy in lung volume measurement as noted in prior prenatal ultrasound comparisons of 2D to 3D lung volume calculations.25,26 Consequently, the 3D-FIESTA sequence may be valuable for the detection of abnormalities and preoperative planning.
Pleural effusion
Fetal pleural effusion is a rare abnormality, resulting from an excessive amount of fluid collection in the pleural cavity between visceral and parietal pleura. The reported incidence of this condition ranges from 1/10,000 to 1/15,000.27–29 The etiology of fetal pleural effusion is still unclear. It can occur unilaterally or bilaterally as an initial symptom of hydrops fetalis, but it can also occur in association with other abnormalities without hydrops fetalis or represent an isolated abnormality.
30
Fetal MRI can evaluate pleural effusion and its pressure effect to the adjacent lung parenchyma and mediastinal structures, which allows consideration of fetal intervention when needed.
29
Furthermore, fetal MRI can determine if there are any other structural anomalies of the fetus (Fig. 2). 3D imaging may be of utility for assessment of pleural effusion when considering possible fetal intervention and targeting chest tube placement. Coronal 3D-FIESTA on 3T MRI showing a 23-week fetus with hydrops fetalis and right pleural effusion (arrow), causing right lung collapse (L) and mediastinal shift. Fetal intervention was considered in this case and thoracic drain placement was performed.
Hepatobiliary anomalies
Fetal hepatic pathology, particularly hepatic masses, can be prenatally diagnosed by imaging. MRI has advantages over ultrasound in detection of subtle lesions and evaluation of abdominal masses and their relationship to the adjacent organs. 31 Single-shot fast spin-echo (SSFSE) sequence depicts water-containing structures well. Solid tumors in the abdomen or pelvis are less well evaluated by SSFSE due to its inferior T2 contrast. 31 Nonetheless, 3D-FIESTA sequence provides superior T2-weighted contrast and enables multiplanar reformatting with reduced partial volume averaging, thereby optimizing lesion identification. 32 Thus, this MRI technique has been applied in various anatomical regions.32–35
Congenital hepatic mass
Hepatic lesions presenting in the prenatal period are uncommon.36,37 The most common primary hepatic tumors are hemangioma (60.3%), mesenchymal hamartoma (23.2%), and hepatoblastoma (16.5%).
38
Hepatic hemangiomas are benign vascular tumors involving the liver with two types, consisting of infantile hepatic hemangioma (IHH) and congenital hemangioma (CH), based on the clinical course. IHH is far more common while CH is rare.
39
IHH has three distinct forms of presentation as focal, multifocal and diffuse.
40
CH demonstrates three patterns including rapidly involuting congenital hemangioma (RICH), non-involuting congenital hemangioma (NICH), and partially involuting congenital hemangioma (PICH).
41
Therefore, imaging plays a key role in the diagnosis and follow-up of this condition. Mesenchymal hamartoma is the second most common benign hepatic tumor in the pediatric population.
42
This pathology is rare and has a variety of imaging findings; however, its prognosis is favorable if treated correctly.
43
Hepatoblastoma is the most common primary hepatic malignancy in children. Patients present with hepatic mass and 50% of cases demonstrate calcification within the mass.
44
MRI is a useful diagnostic tool to differentiate between solid and cystic masses with additional abilities to characterize soft tissue and intralesional components. Congenital hepatic cyst is a rare hepatobiliary malformation, usually unilocular and asymptomatic fluid-filled lesion. Most congenital hepatic cysts develop during late pregnancy; thus, diagnosis can be made if a third-trimester scan is performed.
45
3D-FIESTA imaging provides excellent tissue contrast with thin-slice, multiplanar reconstructions, and maximum intensity projections with 3D rendered reformations, improving visualization (Fig. 3). Axial (a, b) and sagittal (c, d) 3D-FIESTA on 3T MRI showing a fetus with hepatic cystic mass (M), demonstrating claw sign (white arrows) of the liver (L). Note that the hepatic cyst shows an internal septation (black arrows).
Genitourinary tract anomalies
The fetal genitourinary tract is composed of the fetal kidneys, ureters, bladder, and internal and external genitalia. Anomalies of these structures are common and can be detected by prenatal imaging. Although ultrasound is an outstanding tool for detecting fetal genitourinary tract anomalies, it is limited under some circumstances such as oligohydramnios or large maternal body habitus. 46 The fetal urinary system is well visualized by MRI, especially in the cases where ultrasound is limited. Fetal MRI is also a useful adjunct that improves diagnostic accuracy of genitourinary tract anomalies and detects associated malformations of other organs such as pulmonary hypoplasia. 47 In female fetuses, Mullerian duct anomalies have important implications for future reproductive health. MRI helps to characterize features of the uterus, adnexa, and vagina as well as associated urinary tract anomalies to guide clinical management. 48
Female genital anomalies
In general, the T2W MRI sequence is one of the best methods to characterize uterine fundal contour and internal indentation of the endometrial cavity.
49
Characterization of these features is key in the diagnosis of Mullerian duct anomalies.
50
Additional information of the cervix, vagina, adnexa, and ovaries is also provided. However, evaluation of complex anomalies with standard 2D sequences can be challenging. 3D-FIESTA can be helpful given the volumetric acquisition and ability to perform multiplanar reformats in these cases. Further, hydrocolpos and hydrometra can be well evaluated on 3D-FIESTA imaging (Fig. 4). In addition, assessment of the urinary tract anomalies can be promptly identified in the same study.
49
(a) Sagittal single-shot T2-weighted (SST2W) image showing hydrometrocolpos (arrows) with a good resolution image. (b and c) Sagittal 3D-FIESTA images at 3T showing hydrometrocolpos (arrows) with motion artifacts. (d) Prenatal ultrasonography showing hydrometrocolpos. BL = urinary bladder. Vg = vagina. Ut = uterus.
Ureterocele
Ureterocele is the ballooning of the distal ureter into the bladder, urethra, or both.
51
This congenital anomaly can lead to recurrent urinary tract infections or obstruction which can cause permanent damage to the kidneys. Management is variable and related to other factors such as the location of the ureterocele, vesicoureteral reflux (VUR), the age of the patient, single or duplex collecting system, and function of the kidney.
52
Early detection in the prenatal period and proper treatment after birth can prevent serious complications.
53
Fetal MRI delivers anatomical structural details including insertion of the ureter which can aid in postnatal treatment planning. Ureteroceles appear as cystic structures which are well visualized on 3D-FIESTA imaging (Fig. 5). Curved planar 3D-FIESTA on 3T MRI showing a fetus with right hydronephrosis, hydroureter, and ureterocele (arrow). RK = right kidney.
Cloacal exstrophy
This malformation is also known as the omphalocele, exstrophy, imperforate anus, and spinal defects (OEIS) complex, with the incidence of 1:250,000 to 1:400,000 per live births.54,55 The etiology is unknown. The failure of cloacal separation leads to persistent cloaca, rudimentary hindgut, and imperforate anus, which also causes characteristic bowel and bladder exstrophy of the fetuses. MRI is an excellent modality for diagnosing this entity and to evaluate associated malformations. 54 The improved spatial resolution and superior tissue contrast provided by 3T MRI contribute to more effective evaluation of the fetal anatomy. 56 Therefore, the 3D-FIESTA sequence may serve as a useful tool for identifying abnormalities and optimizing preoperative planning.
Musculoskeletal anomalies
Fetal MRI can depict musculoskeletal abnormalities not limited by fetal position or degree of ossification. Prior studies describe MRI in diagnosis of fetal anomalies, assessing associated congenital malformations, and providing therapeutic management.57–59 3D-FIESTA imaging can be used as an adjunct to other promising sequences for fetal MRI.
Clubfoot
Clubfoot or talipes equinovarus is a congenital deformity of the foot, affecting 1–3 per 1,000 live births.60–62 It can be unilateral or bilateral involvement63,64 as well as isolated or syndromic disease.
65
Clubfoot affects bones, muscles, joints, tendons, and blood vessels, leading to abnormal positioning of the foot and ankle. Radiologic features consist of adduction and supination of the forefoot, heel varus, and plantar flexion of the forefoot and ankle (Fig. 6(a)). Severity of disease varies from mild to severe, which can cause serious consequences if left untreated. As the 3D-FIESTA sequences are volumetric, they can be converted into surface rendered files (Fig. 6(b)) which can also subsequently be used in augmented or virtual reality displays or 3D printed. (a) 3D-FIESTA on 3T MRI showing a fetus with a clubfoot (arrow). (b) 3D-FIESTA on 3T MRI showing a screenshot of a surface rendered model which can also subsequently be used in augmented or virtual reality displays or 3D printed.
Other anomalies
Conjoined twins
Conjoined twins, a rare condition, refer to twins that are physically connected. The incidence is approximately 1 per 50,000–200,000 births.
66
Sixty percent of cases are stillborn,
67
depending on severity and complications. Prenatal MRI, especially 3D-FIESTA sequence, allows tissue characterization, informs management options, and predicts prognosis of the conjoined twins (Fig. 7). Additionally, MRI may support preoperative planning for separation if appropriate including use of augmented or virtual reality tools or creation of 3D printed models. Coronal 3D-FIESTA on 3T MRI showing conjoined twins along with banding artifacts (dotted arrows), which occasionally degrades the 3T fetal MRI. Of note, the fetal airway is well seen (solid arrow).
Fetal cervical teratoma
Fetal teratomas are rare congenital tumors,68–70 containing all three germ cell layers. A cervical teratoma is a very rare tumor arising in the neck which can lead to high morbidity and mortality rates as these tumors tend to enlarge and compress the airway and impair fetal swallowing.71,72 As a result, a fetus develops airway obstruction and polyhydramnios which can be fatal. On imaging, cervical teratomas appear as solid or mixed solid-cystic neck masses (Fig. 8). Fetal MRI displays the anatomy and provides additional information of tumor extension for management planning such as Ex utero intrapartum treatment (EXIT) procedure.
72
3D-FIESTA demonstrates improved depiction of the airway structures and finer anatomical details, which may support a more accurate assessment of this condition. Multiplanar 3D-FIESTA on 3T MRI showing a fetus with a large solid-cystic mass of teratoma (M) arising from the neck. This sequence demonstrates a distinct lesion with superior tissue characterization.
Cleft lip
Cleft lip and palate are a common congenital anomaly in the orofacial region.
73
They can be isolated or associated with other deformities. A cleft lip is the result of developmental failure in palatal shelves of the maxillary processes.
74
There are different types of cleft lip and palate, including isolated cleft lip, cleft lip and palate, and isolated cleft palate. The patients with these anomalies require surgery to correct the deformity and achieve normal function. Fetal MRI has been applied in the prenatal diagnosis of orofacial clefts due to its potential to improve detection rate.75,76 A meta-analysis demonstrated the benefits of MRI in cases of fetuses at risk for orofacial clefts given its excellent sensitivity and good to excellent specificity for diagnosing cleft palate.
77
Thus, prenatal MRI can be performed as a complementary tool in fetuses at risk of cleft lip and palate by prenatal ultrasound (Fig. 9). 3D-FIESTA on 3T MRI showing a fetus with cleft lip.
Esophageal duplication cyst
Esophageal duplication cysts are rare congenital anomalies of the gastrointestinal tract in children.
78
These can cause respiratory distress in infancy and childhood, but it often remains asymptomatic in adults.
79
MRI has advantages in localizing the lesion within the mediastinum and improved visualization of abdominal extension.
80
The water content of the cyst is hyperintense on T2W images (Fig. 10). As such, fetal MRI can provide a useful adjunct in antenatal diagnosis, counseling, and preoperative planning if needed (Fig. 11). Sagittal 3D-FIESTA on 3T MRI showing a tortuous, distended, tubular, fluid-filled structure in the posterior mediastinum (arrows). This structure shows peristalsis on ultrasound. No feeding vessel was identified. Esophageal duplication cyst was the primary consideration. 3D-FIESTA on 3T MRI demonstrating 3D rendered model of an esophageal duplication cyst.

Placenta
The use of placental MRI has become increasingly common, particularly for assessing suspected cases of placental adhesive disorders, generally referred to placenta accreta.
81
Although placental disorders are uncommon, they can cause significant maternal and fetal morbidity and mortality. Placental MRI serves as an important diagnostic tool that complements fetal ultrasound (Fig. 12). 3D-FIESTA on 3T MRI demonstrating a surface rendered model of the placenta.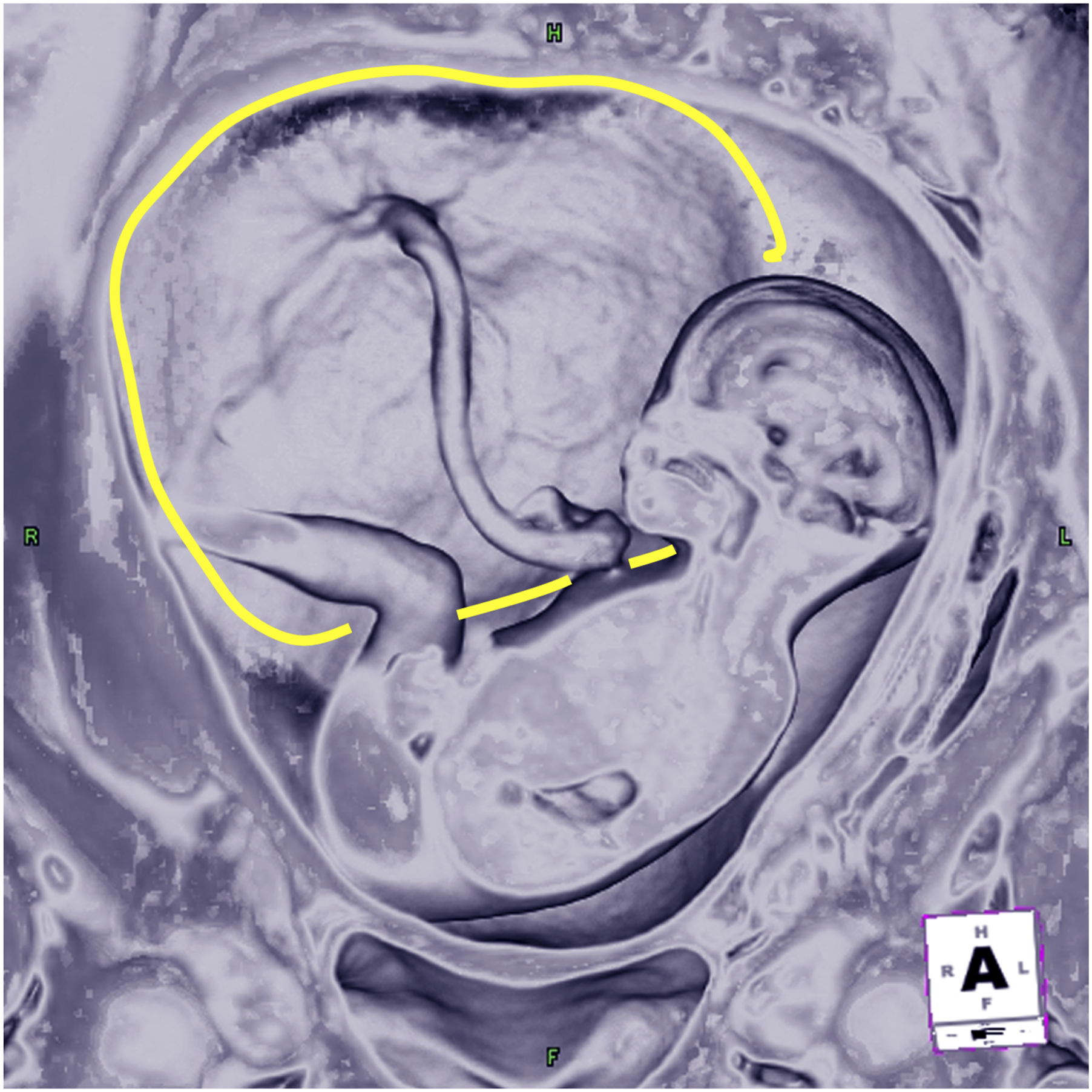
Special considerations
3D-FIESTA imaging is limited in cases of vigorous fetal movement, particularly since maternal sedation is not performed in the United States. A single study has described the use of valium for fetal MRI in the United States. Potentially if management would be impacted based on fetal MRI findings, discussion with the clinical team and a risk/benefit analysis should be conducted to determine need for maternal anxiolytics. 82 While the sequence can be performed at both 1.5 T and 3.0 T, special consideration should be made at 3.0T for standing wave artifacts/dielectric effect in cases of polyhydramnios. If available, imaging at 1.5T is preferable in these instances. In all, this sequence may be most successful in older fetuses with less vigorous fetal motion. While there are no definite recommendations on when to initiate this MRI sequence, its short acquisition time makes it feasible to perform at different stages of the imaging session.
Conclusion
3D-FIESTA imaging is a useful adjunct in fetal MRI examinations. The sequence holds potential to aid in assessment of complex anomalies that would otherwise require multiple multiplanar acquisitions with the added ability to create 3D volume-rendered reformations. This sequence allows high spatial resolution and excellent details depending on tissue contrast, which generates valuable information for diagnostic utility and clinical prognosis; moreover, this sequence provides greater options for prenatal counseling and postnatal management. While not a replacement to traditional sequences, we believe this sequence provides a useful clinical adjunct to standard sequences for fetal MRI.
Footnotes
Acknowledgments
Ethical considerations
The ethical approval was performed under UCSF IRB number 18-25412 for retrospective correlation of imaging with other clinical parameters.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.