
Abstract
Background
Computerized tomography-guided transthoracic needle biopsy (CT-TTNB) plays an important role in the diagnostic work-up of lung lesions. The literature reports varying results on complication rates, severity of complications, and diagnostic yield.
Purpose
To evaluate CT-TTNB as a radiological outpatient clinic procedure and explore diagnostic yield and complication rates.
Material and methods
Between January 2017 and October 2019, a total of 559 patients underwent CT-TTNB. Patient records and CT scans were retrospectively reviewed and patient characteristics, lesion characteristics, biopsy procedure, and per- and post-procedural complications, as well as pathological diagnosis, were registered.
Results
Of 559 patients included, 511 had biopsies performed. Thereby, 48 biopsies (8.6%) were discontinued because of patient compliance issues and/or the occurrence of pneumothorax before the biopsy was performed. The overall pneumothorax rate was 49.2% (n = 275 of 559 patients). Insertion of a drainage catheter was needed in 85 of the 275 patients with pneumothorax. Parenchymal bleeding was seen in 26.5% of the patients and haemoptysis in 5.5%. No cases of bleeding or haemoptysis required intervention or admission. Small mean lesion size and increased distance from pleura to the lesion were associated with a higher occurrence of complications. A conclusive pathological diagnosis was obtained in 278 of 511 (54.4%) biopsies. No patients were re-admitted after the two-hour observational period in the radiological department.
Conclusion
CT-TTNB as an outpatient clinic procedure is feasible but has a moderate diagnostic yield and relatively high complication rates for minor complications.
Keywords
Introduction
With the advancement of computerized tomography (CT) scans, the implementation of low-dose CT, and the upcoming era of lung cancer screening programs, there has been an increase in the number of detected lung lesions. 1 The potential incidental finding of lung lesions on CT scans has led to an increased chance of early detection and detection of smaller lesions than previously. Since lung cancer is the most common cause of cancer death worldwide with approximately 1.80 million annual deaths, it is crucial to identify and characterize lung lesions as either benign or malignant. 2
The Fleischner Society guidelines from 2017 state that the key goal of nodule management is to reduce the number of unnecessary diagnostic evaluations in patients with a <1% chance of having lung cancer. 3 However, implicit in this statement, is the notion that individuals with a ≥1% probability of lung cancer should undergo further diagnostic evaluation. To overcome this challenge, the Fleischner Society as well as the national lung cancer group presented guidelines and recommendations for invasive diagnostics and follow-up that are individually dependent on patient and nodule characteristics.3,4
An endobronchial biopsy is generally preferable for histopathological examination due to the lower risk of complications when compared to transthoracic biopsies. Additionally, endobronchial biopsies (e.g. endobronchial ultrasound (EBUS) and endoscopic ultrasound (EUS)) can in some cases provide both diagnosis and ensure accurate N-staging, which is not possible using the transthoracic approach. 5 For peripheral lung lesions, ultrasound or CT-guided transthoracic needle biopsy (CT-TTNB) is more often used. 6 Previous studies have found CT-TTNB to provide a definitive pathological diagnosis in 64.6% to 98.6% of the biopsies.7,8 The two most common complications of CT-TTNB are pneumothorax and parenchymal lung bleeding, with 18.1%–44% and 14.0%–51.1% risk, respectively.9,10 Both biopsy accuracy and management of complications seem integral considering the increasing number of biopsy procedures, more attempts to biopsy smaller lesions than before, and the increase in both age and comorbidities in patients referred for biopsy.
This study aims to evaluate the diagnostic yield and complication rates in our institution where CT-TTNB is performed as an outpatient procedure.
Methods
Study design and setting
The study was a retrospective study carried out at the Department of Radiology at Odense University Hospital, Denmark for 32 months, from January 2017 to October 2019. The study was conducted and reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE guidelines). 11
The study was carried out in accordance with the Helsinki Declaration and was approved by the Danish Protection Agency with registration number 19/44304.
Participants
All patients undergoing CT-guided transthoracic needle biopsy for a CT-verified lung lesion suspicious of malignancy were eligible for inclusion in the study.
All patients were seen in the respiratory outpatient clinic. The respiratory physicians assessed whether the patients fulfilled the criteria of referral to CT-TTNB: the patients must have a valid lung function test with Forced Expiratory Volume in 1 second (FEV1) >30% or >1 L. If the patients were treated with anticoagulation medication or thrombocyte inhibitors, these were paused or bridged depending on the type of medication, estimated glomerular filtration rate (eGFR), and/or INR according to national guidelines. 12
Patients having more than one procedure performed during the study period were only included in the first procedure.
Biopsy procedure
The biopsy procedure and patient care were managed as an outpatient clinical procedure at the Department of Radiology. Patients met in the radiological outpatient clinic and were welcomed and informed by a radiographer.
A total of five experienced interventional thoracic radiologists with at least 2 years of experience and between 100 and 1.500 procedures performed the CT-TTNB procedure.
No systemic sedation or anaesthesia was used. The procedure was guided using helical scans with a Siemens Somatom Flash CT scanner (Siemens Healthcare GmbH, Erlangen, DE) with the placement of a radio-opaque grid over the lesion to determine the percutaneous entry point. The safest and most appropriate pathway to the lesion was determined, preferably with the patient in a supine position and, if possible, with the avoidance of needle pathways through fissures and interlobular spaces. ‘SeeStar’ (AprioMed, AB, Uppsala, Sweden) was subsequently used to plan, guide, and maintain needle direction during the biopsy procedure. The biopsy area was disinfected and draped, and local anaesthetics (1% lidocaine) were administered to the entry site. Following the insertion, a CT scan was performed to confirm the correct needle position.
Biopsies were performed as fine needle aspiration biopsies (FNAB) with a 20-gauge biopsy needle (Franseen, Argon, Athens, USA) or using tissue core needle biopsies (CNB) with an 18-gauge biopsy needle (Semi-automatic Guillotine Needle, Delebio, Italy) dependent of the operator.
No pathologists were available at the operation theatre and thereby no rapid on-site cytological evaluation (ROSE) was performed. A post-procedural CT scan was performed immediately after the biopsy to rule out acute complications. If complications occurred, severity and clinical symptoms were assessed and managed according to local instructions in the department, but the radiologist decided, for example, if intervention was required or if the patients should be referred to the respiratory department for closer follow-up.
If the patient had no or minor complications not requiring treatment, the patient was kept in the radiological outpatient clinic for a two-hour observational period ending with a conventional chest X-ray. If nothing abnormal was detected, if a small but stable pneumothorax was detected, or if a proven minor haemorrhage was asymptomatic, the patient was discharged.
Variables
Data regarding the lesions were collected from the Picture Archiving and Communications System (PACS) in axial reconstructions from CT scans taken during the biopsy procedure. Lesion or mass size was defined as the maximum measured diameter. Lesion location was noted. Lesion or mass position was assessed and categorized into three zones (peripheral-, middle-, and central third) and needle depth was measured as the distance from the skin (puncture site) to the centre of the lesion.
Patient data were collected from the Radiology Information System (RIS) and electronic patient records.
Per- and post-procedural complications were recorded: type of complication (pneumothorax, bleeding, infection, and haemoptysis) and scored according to the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Quality Assurance Document and Standards for Classification of Complications scale
13
: • CIRSE 1: Complication during the procedure which could be solved within the session; no additional therapy, no post-procedure sequelae, no deviation from the normal post-therapeutic course. • CIRSE 2: Prolonged observation including overnight stay (<48 h); no additional post-procedure therapy, no post-procedure sequelae. • CIRSE 3: Additional post-procedure therapy or prolonged hospital stay (>48 h) required; no post-procedure sequelae. • CIRSE 4: Complication causing permanent mild sequelae (resuming work and independent life). • CIRSE 5: Complication causing permanent severe sequelae (requiring ongoing assistance in daily life). • CIRSE 6: Death.
Only complications requiring contact or admission to the hospital were noted since data from general practitioners was not possible to retrieve.
The total number of biopsies taken from each patient and the type of biopsy needle used (fine needle aspiration biopsy (FNAB) or core needle biopsy (CNB)) were also registered.
Histopathological information about general diagnosis (malignant, benign, or inconclusive) and type of specific diagnosis were also collected. An inconclusive result was generally given when biopsy material was insufficient, biopsy material did not represent the lesion assessed by the pathologist, or the pathologist could not definitely determine the exact pathology.
Statistical analysis
Statistical analysis was performed as univariate chi2 and Fischer’s exact test for categorical variables and Wilcoxon Rank Sum test for continuous variables. Lesion size was divided into three groups with the cutoff being <1.5 cm, 1.5-3 cm, and >3 cm and sub-group analysis was performed. p-values <0.05 were considered statistically significant. Statistical analyses were performed using STATA/IC 16 (StataCorp LP, College Station, TX, USA)
Results
Patient inclusion and demographic
Patient-, lesion- and procedure characteristics (n = 559).
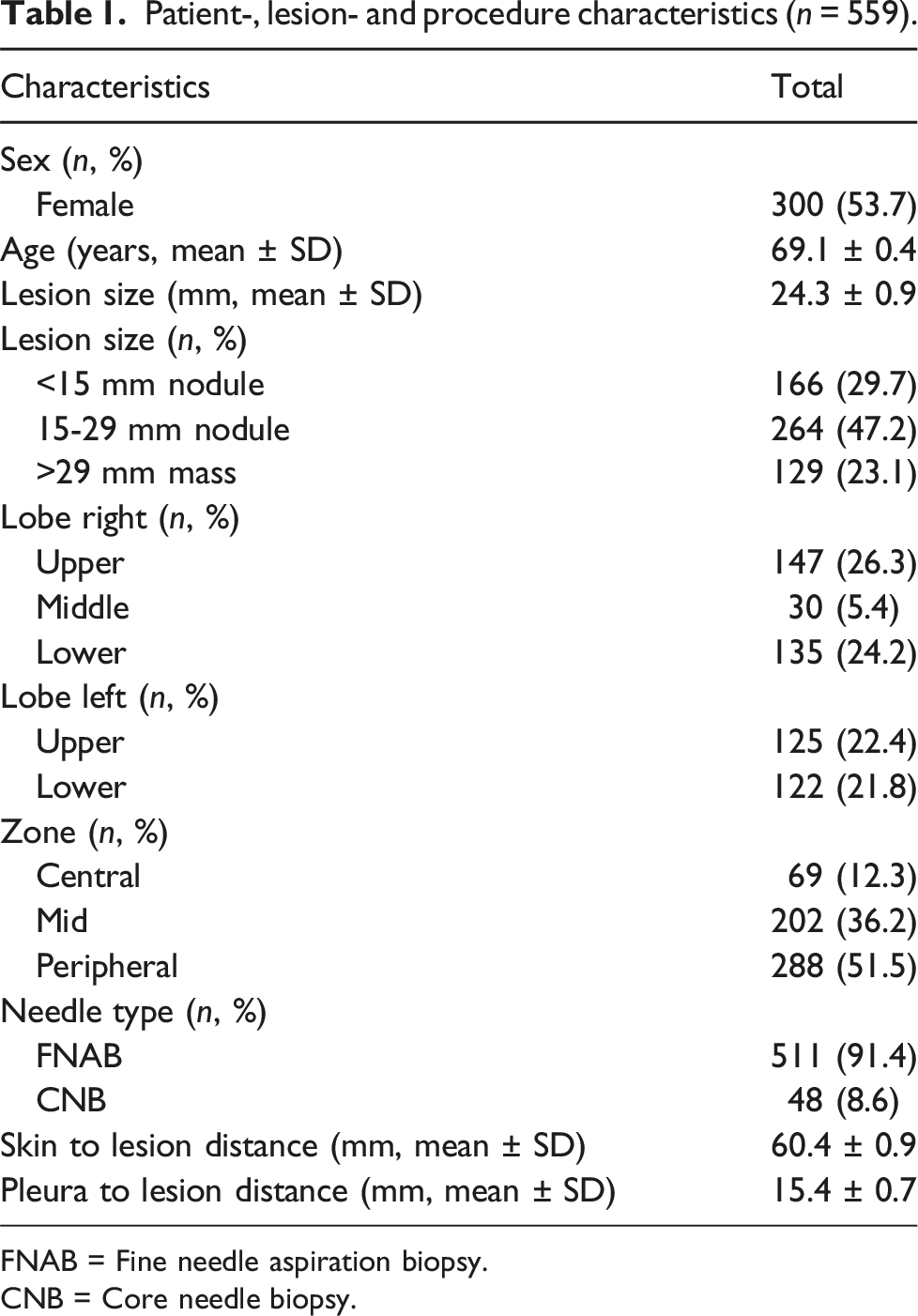
FNAB = Fine needle aspiration biopsy. CNB = Core needle biopsy.
Diagnoses and diagnostic yield
The overall diagnoses of the obtained biopsies were distributed as follows: 226 of 511 patients (44.2%) received a malignant diagnosis (intention-to-treat (ITT): 222 of 559 = 40.4%), 52 of 511 patients (10.2%) received a benign diagnosis (ITT: 52 of 559 = 9.3%), and a total of 233 (45.6%) pathology results were inconclusive (ITT: 233 of 559 = 39.9%).
The patient flowchart, distribution of histopathological diagnoses, and next step for discontinued and inconclusive answers are shown in Figure 1. Of the 233 inconclusive histopathological results, 173 (74.2%) were due to the quality or quantity of the biopsy material. Patient flowchart, pathological distribution, and next step for discontinued and inconclusive biopsies. VATS = video-assisted thoracic surgery, ENB = endobronchial navigation bronchoscopy, Radical EBUS = radical endobronchial ultrasound, EBUS = endobronchial ultrasound, Diagnosis = Diagnosis was established based on biopsy from another organ system or in multidisciplinary consensus without further invasive procedures, Ended = patient ended without further invasive diagnostic procedures either based on the patient’s wish or multidisciplinary consensus.
Patients with inconclusive results had various pathways for further diagnostics: patients (30.6% of the 281 inconclusive and non-obtained biopsies had renewed CT-TTNB performed.
Complications
Of all 559 patients, 275 (49.2%) had a procedure-related pneumothorax. Of these, 85 patients needed acute drainage equivalent to 30.9% of 275 patients with pneumothorax. The pneumothoraces were detected immediately on the post-procedural control CT in most of the cases (248 of 275 cases, 90.2%). The remaining 27 (9.8%) were detected in the 2-h observational period following the biopsy, either by scheduled chest X-ray or by clinical manifestation of symptoms of respiratory distress, none of these needed acute intervention but were managed with an extended observational period and an extra chest X-ray to ensure that the pneumothorax was not increasing in size. None of the patients who left the radiological outpatient clinic following the observational period was re-admitted due to complications related to the biopsy procedure.
CIRSE classification of complications.

Hospitalization time ranged from 1 to 17 days, with a mean of 1.2 days for patients hospitalized with complications. None of the included patients died during hospitalization for complications or within the 7 days follow-up.
Risk factors for complications
Description and statistics on complications of pneumothorax and drainage insertion.

Bold equals p-value below 0.05 assigned as significant.
Risk factors for parenchymal bleeding and haemoptysis.

All data is N (%) or Mean ± SD.
Bold equals p-value below 0.05 assigned as significant.
Discussion
The current study demonstrated that CT-TTNB has a moderate diagnostic yield of 54.4% along with a relatively high risk of complications. Our findings demonstrate that CT-TTNB can be effectively performed as an outpatient clinic procures without any readmissions but careful considerations should be given to patient selection, such as considering alternative endobronchial options.
Previously published studies on the diagnostic yield of CT-TTNB have reported a slightly higher diagnostic yield ranging from 64.6 to 67.6%, compared to the 54.4% yield found in this study. These studies mostly involved larger mean lesions ranging from 31.0 to 41.4 mm whereas our study reported a mean lesion size of 24.3 mm.10,14–16 There is supporting evidence that the number of inconclusive biopsies increases significantly as a result of minor lesion size.17–19 This may explain the number of inconclusive biopsies in this study.
In our institution, there was also frequent use of other diagnostic methods for biopsy procedures like ENB, radial EBUS with biopsy, and ultrasound-guided transthoracic needle biopsy. This could potentially change the study group and patient selection compared to other studies because it could decrease the total number of CT-guided biopsy procedures, increase the number of smaller lung lesions and subsequently decrease the number of ‘easy to hit’ lesions.
Another possible explanation for the number of inconclusive biopsies is the very high percentage of fine needle biopsies in this study. Most of the patients underwent fine needle biopsy, which has been found to have a significantly decreased accuracy compared to core needle biopsy.16,20,21
Additionally, in this study and in our institution, we do not use rapid on-site cytological evaluation (ROSE) during the biopsy procedure. Today, there is an increasing number of studies and subsequent institutions using ROSE in the CT-theatre suite that evaluates the material before ending the session,22,23 thus improving diagnostic yield but also histopathological evaluation performed by trained pulmonologist. 24 In line with this finding, another study raises concerns that it is more difficult for the pathologist to give a benign diagnosis compared to a malignant from cytological material from the fine needle biopsy, since the pathologist can only examine cytopathology and not histopathology from the material. 25 In summary, a greater proportion of core needle biopsies or the use of ROSE when using fine needle biopsy would probably be beneficial to the diagnostic yield of future biopsies.
In concordance with current evidence, the present study found that pneumothorax and parenchymal bleeding are the most frequent complications of CT-TTNB. The vast majority of pneumothorax occurrences were diagnosed during or immediately after biopsy on the post-procedural control CT scan. However, a minor number of patients (9.8%) were diagnosed with pneumothorax during the four-hour observational period of this study. Following this study, another study was conducted at our institution examining patients with continuous lung ultrasound every 30 minutes during the now two-hour observational period. 26 This study did not find pneumothoraces that increased in size during the observational hours and concluded that patients with no or minor symptoms and a small pneumothorax did not have the need for intervention after being transferred from the CT theatre to the observational room. This could aid a more conservative treatment strategy for asymptomatic or nearly asymptomatic pneumothoraces in line with newer studies on spontaneous pneumothorax.27,28
We identified pneumothorax in almost half of the patients. This may seem slightly high as compared to the pooled mean of 25.9% (range 4.3% to 52.4%) found in a recent systematic review and meta-analysis by Huo et al. 18 However, several other studies have reported pneumothorax rates ranging from 44 to 62%.29,30 Recently, Elshafee et al. reported a pneumothorax rate of 44% in a German population, similar to the one in this study. 9 The occurrence rate of pneumothorax found in this study may be attributed to the risk factors found associated with pneumothorax. It has been established, in both this study and in several other studies that small lesion size is associated with a higher occurrence of pneumothorax.14,15,31–34 Other studies with lower rates of pneumothorax (14.4 to 23.1%) reported mean lesion sizes between 31 and 52 mm.14,16,32
Also, the pleural drainage insertion rate of 15.2% found in this study was within the range 0%–18.6% as reported by others, 32 including another Danish study by Vagn-Hansen et al. who found a similar rate of approximately 15%. 35 Immediate procedure-related bleeding 148 of 559 patients (26.5%) and haemoptysis 31 patients of 559 (5.5%) were both well within the rate established by other studies, 1.4%–51%10,36 and 0.4%–23.4%,14,37 respectively.
We acknowledge that the study has some limitations. First, the study has a retrospective design which in itself leads to several limitations of residual confounding and risk of bias. Additionally, all patients and data were retrieved from one single institution. That said, the number of included patients is high and to our knowledge, this is the first study to present CT-TTNB as a radiological out-patient clinic procedure where the patient is not admitted to a respiratory department or ward.
We registered data on post-procedural complications up to 1 month after the procedure. This means that if any complication arose later than the given time period it would not be included in the data of this study, however, when assessing complications of surgery or invasive procedures, 30 days are normally used.
Evidence shows correlation between pneumothorax and the presence of pulmonary emphysema.10,18,38 However, information about the presence of emphysema was not recorded in the data available. Likewise, information about other risk factors related to the biopsy technique was not noted in this study because data was not available in the databases. These factors include variables needle size or number of needle passes, which were all based on the operators’ considerations. Contrary to lesion- and patient properties, these variables could be modified in order to lower the risk of complications and therefore a prospective cohort could further explore the effect on complication rates.
As mentioned, the increasing number of thoracic CT scans will probably lead to more incidental findings and subsequently more biopsies needed. Since the endobronchial approaches are proven to have a lower complication risk, it is crucial that multidisciplinary team decisions on whether to perform endobronchial or transthoracic biopsy are made. The Fleischner Society has established evidence-based guidelines on follow-up regimes for specific patients so that not all patients need biopsy. 39 Additionally, results from the first lung cancer screening programs are now being published which in the future and over time can change the management of the incidental pulmonary lesions.40,41
In conclusion, the results of current study suggest that CT-TTNB has a moderate diagnostic yield and a quite high complication rate but low rates of major complications needing more intervention than pleural drainage. CT-TTNB is a feasible procedure to handle in a radiological outpatient clinic with a two-hour observational period but considerations on patient selection must be done.
Footnotes
Acknowledgements
The author group would like to thank all the patients involved in the project as well as all the radiographers involved in the radiological outpatient clinic at Odense University Hospital for observing and taking care of the patients and aiding to research projects.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.