
Abstract
Background
Extensor Carpi Ulnaris (ECU) tendinosis, a frequent cause of chronic wrist pain, requires prompt diagnosis to prevent disability. This study demonstrates the use of convolutional neural networks (CNNs) for automated detection and segmentation of the ECU tendon and tendinosis in 2D axial wrist MRI.
Purpose
To develop a CNN for the automated detection of ECU tendon and automatic delineation of tendinosis in 2D wrist MRI. The study serves as a proof-of-concept, demonstrating the feasibility of automating the segmentation of musculoskeletal structures in wrist MRI and offering an efficient solution for detecting tendinosis.
Material and Methods
In a retrospective analysis of 1081 patients undergoing wrist MRI imaging, 46 patients exhibited tendinosis. Two deep learning-based methods for segmenting the ECU tendon and T2 hyperintense lesions indicative of tendinosis from 2D axial wrist MRI series were developed and compared in this study. Both methods were trained and evaluated over all 46 patients using Dice score as the main evaluation metric.
Results
The mean ECU tendon segmentation Dice score ranged from 0.61 to 0.64 (± 0.27 to 0.31). Tendinosis detection yielded a Dice score of 0.38 for both the threshold method (±0.19) and the CNN (±0.22). A Dice score > 0.50 indicated successful detection, with our methods achieving a detection rate of 72–76%.
Conclusion
The developed CNN effectively detected and segmented the ECU tendon in 2D MRI series. Tendinosis was detected with comparable accuracy using both signal intensity thresholding and the trained CNN method.
Introduction
The extensor carpi ulnaris (ECU) tendon, integral for wrist extension and ulnar deviation, is susceptible to tendinosis, stemming most commonly from repetitive use or degeneration. Proposed reasons for tendinosis include mechanical overload and microtrauma, pathological responses (Prostaglandin E2 and inflammatory cell infiltration), and aging process of tendon stem cells.1,2
ECU tendinosis significance lies in its potential to cause chronic pain and impair wrist function. Prompt diagnosis is crucial to avoid long-term disability, especially in populations engaged in repetitive wrist motions.
Treatment strategies for ECU tendinosis involve conservative approaches, including rest, physical therapy, and corticosteroid injections. Surgical options can be entertained in persistent cases of tendinosis where co-compartment release could prove beneficial. 3 In cases of concurrent subluxation or instability, sub-sheath repair or reconstruction has shown good post-operative outcomes.1,4 MRI imaging plays a pivotal role in diagnosing and determining the treatment course, including assessing candidacy for surgical procedures.
MRI findings in tendinosis are distinctive, showing tendon thickening or thinning and T2 hyperintense lesions. 5 These lesions are associated with disorganized collagen fibers and increased water content. 6 While the significance of T2 hyperintense lesions is debated—appearing in both asymptomatic and symptomatic 7 patients, and sometimes linked to peripheral TFCC tears 8 —this study focuses on T2 hyperintense lesions as a marker of tendinosis. 9
In the realm of wrist MRI, advancements are observed in areas such as cartilage segmentation and segmentation of bone marrow edema. Additionally, there is notable presence of studies focusing on automated detection of osteoarthritis and rheumatic diseases. Artificial intelligence in tendon segmentation, identification, and detection of pathologic changes has been done before in musculoskeletal MRI, in the form of quantifying tenosynovitis 10 in wrist MRI, knee ACL tear identification, 11 quadriceps and patellar tendon mapping, 12 Achilles’ tendon tear mapping, 13 peroneal tendon mapping, 14 shoulder rotator cuff tendon tear identification, 15 and gluteal tendinopathy mapping. 16
In the current literature, the segmentation of ECU tendon and possible associated tendinosis are not well represented. This study is a proof-of-concept where we trained a convolutional neuronal network (CNN) to automatically identify and segment the ECU tendon and additionally to delineate tendinosis.
Materials and methods
We conducted a retrospective study of the electronic medical records in a tertiary hospital. All primary MRI imaging studies with a unique patient (n = 1081) aged >15 years who underwent at least a finger, wrist, or hand imaging referred by a hand surgeon or resident from Töölö University Hospital in Helsinki between January 2016 and June 2017 were included in the study (Fig. 1). The patients were all over 15 years old, as the selected hospital only treated older patients; younger patients are directed to a children’s hospital. Study inclusion flow chart.
From the dataset, we identified 4% (n = 48) with prominent high T2 or PD fs signal within the tendon constituting tendinosis. The material consisted of 23 males, 23 females, with a mean age of 45.43 years (±14.58).
Orientation of study data were 76% (n = 35) with the phalanges pointing superiorly, 20% (n = 9) with phalanges pointing inferiorly, and 2% (n = 1) were oblique and 2 % (n = 1) were horizontal. Also, in 93% (n = 43), the axial series was oriented as having the palmar side pointing toward the superior edge of the image, and in 7% (n = 3), the volar side pointed inferiorly. FOVs of the studies consisted of only the wrist in 87 % (n = 40), wrist and palm in 7% (n = 3), whole hand in 4% (n = 2), and wrist and distal antebrachium in 2% (n = 1). Each study was imaged either with a GE Optima 430 1.5T or Sigma HDxt 1.5T MR scanner. Routine clinical axial, sagittal, and coronal MRI 2D sequences were used including coronal and sagittal T1, PD with fat saturation, gradient-echo T2, and axial PD and PD with fat saturation. From the studies, only axial proton density fat-saturated or T2 fat-saturated series were segmented and trained.
Manual segmentation
The axial series of each study were manually segmented using 3D Slicer 5.4.0 17 by the radiologist (MH). The ECU tendon was segmented fully in the field of view, right until its insertion in the 5th metacarpal base. Tenosynovitis was noted in 11% of cases (n = 5), and in 2% (n = 1) of cases, pulsation of nearby artery caused high signal artefact in the ECU tendon, but neither finding was included in the segmentation.
Tendinosis was segmented as a separate entry. High signal areas caused by artefacts (mostly golden angle or pulsation) were delineated. An example segmentation is illustrated in Fig. 2. Example of manual segmentation. Left: Radiologist segmented axial slice of PD FS series. Right: Corresponding unsegmented slice.
Automatic segmentation
Two different methods, visualized in Fig. 3, for automatic segmentation of ECU tendon and tendinosis were experimented. In the first (1) method, 2D V-Net model was used for segmenting both the ECU tendon and tendinosis slice by slice. The architecture of the model followed the MONAI version 0.8.0 implementation of the one proposed in a previous study.
18
In the architecture, 2D convolutional layers replaced their 3D counterparts, the number of convolution layers was slightly different than in the previous study, batch normalization and dropout was applied and exponential linear units were used instead of parametric linear units. The architecture is visualized in more detail in Fig. 4. The model predictions were post-processed by removing all but the largest ECU tendon prediction in terms of z-axis length. All tendinosis predictions outside the largest prediction were also removed. Two methods used in this study for segmentation of ECU tendon and tendinosis. In the first, 2D V-Net segments axial wrist MRI-scans slice by slice and produces both 3D ECU tendon (shown in green) and tendinosis segmentation predictions (shown in yellow). In the second, another 2D V-Net creates only ECU tendon prediction and tendinosis is defined based on a thresholding algorithm. The algorithm assigns voxels inside ECU tendon prediction volume as tendinosis voxels based on given intensity percentile and uses erosion operations to smooth the result. The neural network architecture of the V-Net models used in this study. Output dimension n is two with method 2 and three with method 1. Padding is applied to all convolution layers except those with 2 × 2 filters. The bias parameter is not learned in any of the convolutional layers.

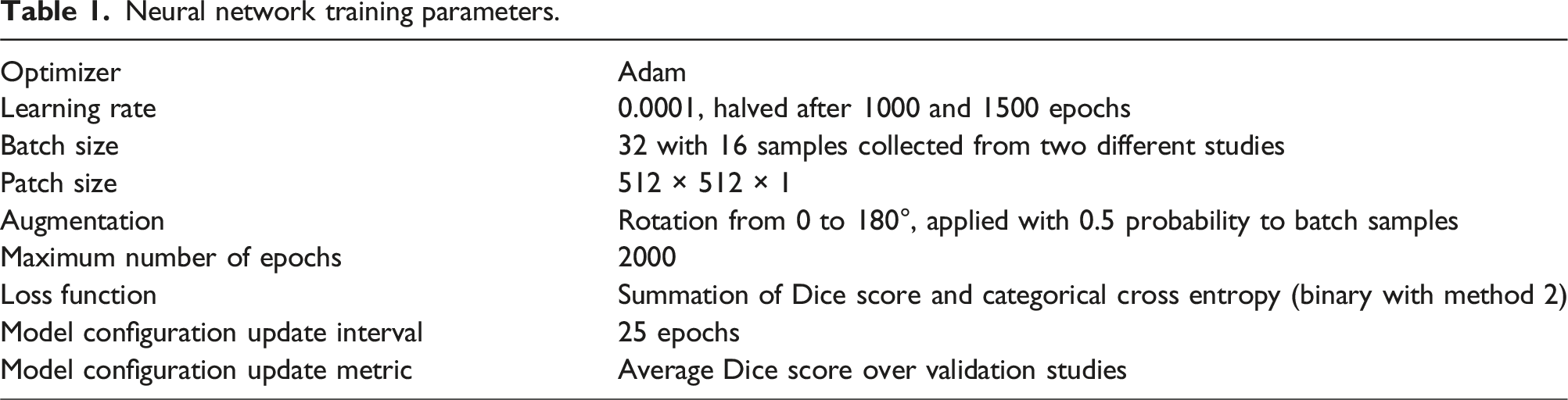
Neural network training parameters.
In the second (2) method, V-Net model was used only to delineate ECU tendon and tendinosis segmentation was created via automatic threshold-based algorithm. The architecture of the model was the same as in the method 1, but output dimensions were 2 instead of 3. The algorithm first eroded the ECU tendon slice by slice with one pixel kernel size. Then, the ECU tendon was segmented based on a given intensity percentile threshold and the voxels above this percentile were determined as tendinosis. Tendinosis predictions of each slice with less than 3 pixels were removed as a smoothing measure. In the method, again 6 V-Net models were trained with the same training setup and otherwise the same architecture, but output channels set to two, as in the method 1. In addition, the post-processing operation of the method 2 was also used to ECU tendon predictions before applying the algorithm.
Evaluation metrics
Evaluation metrics consisted of Dice score and detection score. The detection rate was derived from Dice score and had a binary output: 1 if Dice score between predicted and reference segmentation was over 0.5 and 0 otherwise. Mean and standard deviations of these scores were calculated over all combined 46 studies of the test sets of methods 1 and 2.
Results
The mean ECU tendon segmentation Dice score was Successful detection of the same case as in Fig. 2. Left: Successful automatic segmentation. Right: Corresponding unsegmented slice. Unsuccessful prediction. Left: base of MCV has been segmented. Right: Corresponding unsegmented slice.

Regardless of the method used, the results obtained with the trained CNN and the threshold method were comparable.

In the table are shown the percentiles of signal intensity threshold values. The resulting predictions are compared to radiologist-segmented tendinosis, depicted as Dice scores. The optimal threshold for signal intensity was at the 70-75th percentiles.

The breakdown of false positives after post-processing is as follows: In the first method, other tendons were incorrectly identified in 5 out of 6 false positives, with one instance involving the base of the 5th metacarpal (shown in Fig. 6). Additionally, a dorsal metacarpal vein was predicted in one case. In the second method, three false positives involved other tendons, while in one study, no predictions were made.
Discussion
The extensor carpi ulnaris (ECU) tendon, integral for wrist extension and ulnar deviation, can be a source of discomfort and impairment. Biophysical properties such as water content and disorganization collagen fibers 6 of tendons define their T2 signal in MRI. Tendinosis can signify T2 signal increase relating to degeneration and tearing. 8 This makes detecting ECU tendon abnormalities in wrist MRI studies meaningful. Here, we present a method for detecting the ECU tendon and tendinosis using a CNN to generate predictions, along with a secondary approach that employs a CNN for tendon detection and a relative signal threshold method for tendinosis detection. This is a proof-of-concept study, showing that single tendon detection and tendinosis changes can be automatically detected and segmented with reasonable accuracy.
Segmentation of various tendons in the carpal tunnel of the wrist has been done before, 19 our study builds upon this by segmenting a single specific tendon and being able to delineate tendinosis. Segmentation of signal increase in tendons has been done in the supraspinatus tendon 5 , patellar tendon, 20 and the Achilles’ tendon, 21 but not in the wrist—and studies aiming to do both are not well represented in current research.
In our method, the CNN successfully detected the ECU tendon along with tendinosis with respectable precision in 72%–76% of studies. We achieved a mean ECU Dice score of 0.61–0.64 for tendon segmentation and a Dice score of 0.38 for tendinosis detection compared to radiologist-segmented series using both methods. False positives primarily involved the predictions of other tendons, as well as the dorsal metacarpal vein and bony structures. False positives could be reduced by using more consistent FOVs in training data and the orientation of the wrist could be constant, but the inconsistencies in the data represent normal hospital imaging studies that could be seen as a strength of the created algorithm.
In this study, only axial 2D series were used, no coronal or sagittal series were used and no 3D series. Incorporating orthogonal series might improve the results, but because of the orientation of the ECU tendon in wrist MRI, we suggest that the axial plane is representative of the capabilities of CNN automatic segmentation. We recognize that higher field strengths (3T), thinner slices, and optimizing protocol echo times for tendon imaging could further improve the detection of the ECU tendon and associated tendinosis.
One of the limitations of this study was that there were now separate test set, as the methods 1 and 2 were tested via cross validation. However, no hyperparameter tuning for 2D V-Nets of the methods was performed, except for the choice of amount of dropout and rotation augmentation. With the rotation augmentation, we tried to address the variation of location of ECU tendons in the series images and dropout was used to prevent overfitting. 2D V-Nets used otherwise their baseline architectures freely available in MONAI. Other training parameters were chosen based on previous promising results on a different segmentation task. 22 Cross-validation with separate validation and test sets allowed us to use all 46 studies as a combined test set and to ensure that no neural network weight parameters were updated based on the test set studies.
In conclusion, we demonstrated a proof-of-concept method that shows promising results in detecting the ECU tendon and tendinosis in 2D MRI axial series. This type of automatic segmentation of wrist tendinosis does not have representation in current literature, and pairing with accurate tendon segmentation offers new perspectives into the use of CNN in MRI reading that may benefit patient and clinician. This study holds clinical significance as timely detection of ECU tendinosis is important for preventing chronic pain and preserving wrist function. Drawing attention to abnormal findings in MRI imaging aids in diagnosis and avoiding long-term disability, particularly in individuals with repetitive wrist motions. Our research contributes to advancing musculoskeletal MRI techniques, offering a method for automatically detecting both tendon and tendinosis. This is of importance given the role of MRI in guiding treatment decisions.
Footnotes
Acknowledgments
The authors wish to thank the Finnish Computing Competence Infrastructure (FCCI) for supporting this project with computational and data storage resources.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Helsinki University Hospital [MK: Y780024033].