
Abstract
Ganglioneuromas are rare tumors arising from retroperitoneal and posterior mediastinal sympathetic nerves. Intracranial trigeminal nerve ganglioneuromas are even more rare, with only seven cases reported to date. We present a case of a 65-year-old male with a right-sided throbbing headache type and blindness in his right eye. Magnetic resonance imaging revealed an ill-defined mass lesion in the middle-cranial fossa, with a few areas having a reduced apparent diffusion coefficient and multiple microhemorrhages. Piecemeal debulking of the tumor was achieved by performing a right-middle craniotomy via the pterionic and sub-temporal approach. The detected histological features matched those of a ganglioneuroma (maturing type) of the trigeminal nerve.
Keywords
Introduction
Ganglioneuromas (GNs) are rare benign tumors originating from neural crest cells, typically from sympathetic nerves of the peripheral nervous system and adrenal glands. The occurrence of GNs within the intracranial region is rare, with only seven documented cases of GNs arising from the trigeminal nerve to date.
Case history
A 65-year-old male was admitted to the Neurology Department of our institution with the symptoms of a right-sided throbbing headache type, progressive diminution of vision in his right eye, tinnitus, hearing loss in his right ear, and swaying to the right side while walking that had been experienced for 3 years. On examination, the patient was afebrile, and his vital signs were within normal limits. On neurological examination, diminished sensation on the right half of his face and complete blindness in his right eye, and conductive hearing loss in right ear (Rinne’s test negative) were observed. All other functions were within normal ranges.
Computed tomography (CT) scans demonstrated a lobulated heterogeneous, predominantly hypodense mass in the right Meckel’s cave and middle-cranial and pterygomaxillary fossa. The lesion extended into the right sphenoid sinus and suprasellar cistern. Erosion and destruction of the adjacent bones including the clivus, sella turcica, and sphenoid and petrous parts of the temporal bone were noted (Figure 1(a)–(c)). (a)–(c) Images of the brain of a 65-year-old male with a trigeminal ganglioneuroma. Axial CT sections of brain in parenchymal and bone windows (a), (b) and sagittal section in the same (c) demonstrating a hypodense lesion in the middle-cranial fossa resulting in erosion of the right petrous temporal bone (white arrow) and Sella turcica and upper part of the clivus (black arrow).
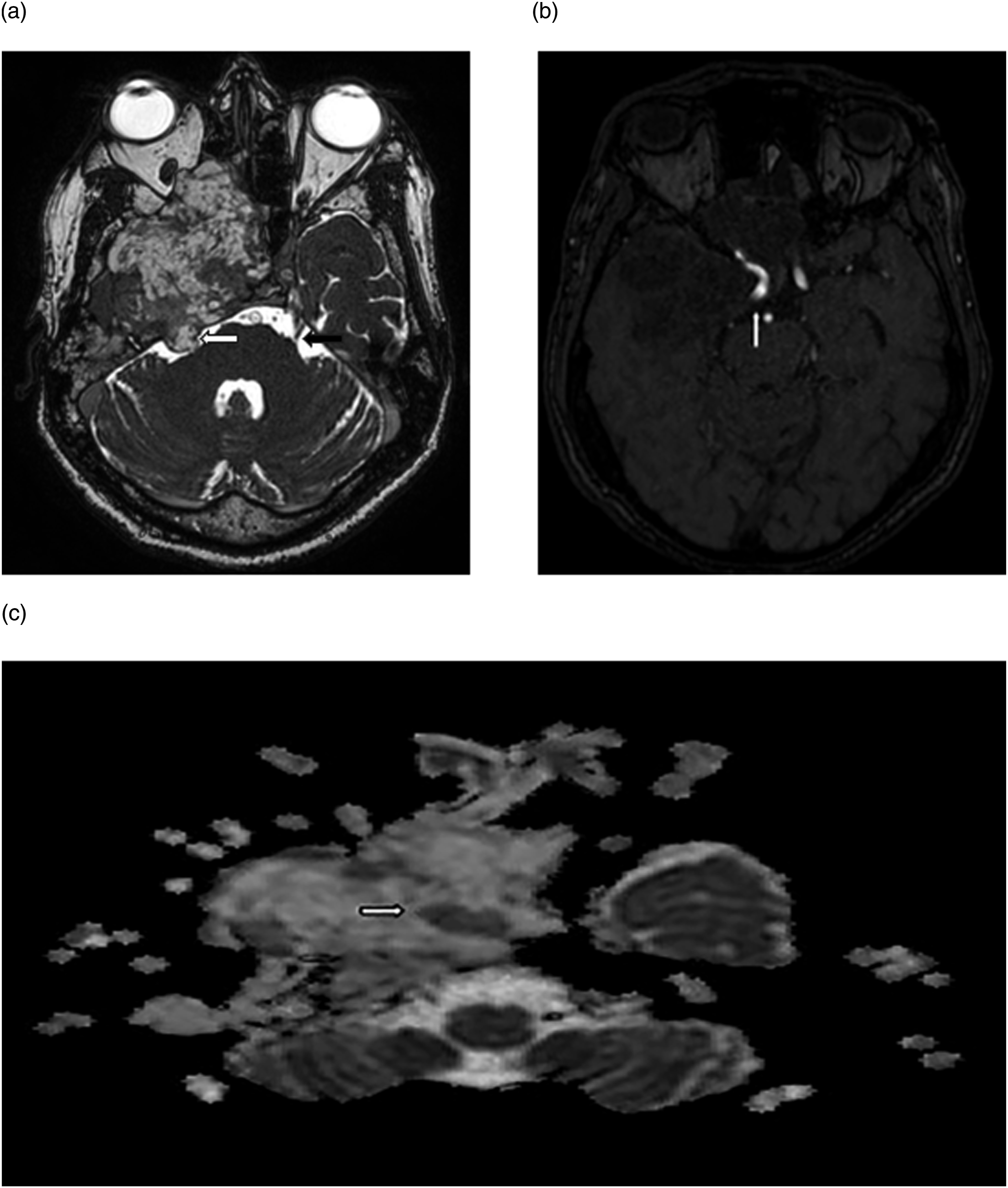
Magnetic resonance imaging (MRI) showed an ill-defined heterogeneous lobulated mass in the middle-cranial fossa and in the base of the skull where the mass was spreading anteriorly into the anterior cranial fossa and the ethmoid sinuses, medially into the sphenoid sinus and suprasellar cistern, and inferiorly into the pterygomaxillary region. On T2-weighted (T2W) images the lesion was heterogenous, and predominantly hyperintense, and hypointense on T1-weighted (T1W) images and on contrast, heterogeneous avid enhancement was noted. Multiple areas showed micro hemorrhaging on susceptibility-weighted imaging (SWI) (Figure 2 (a)–(f)). Balanced fast-field echo revealed a small tail of the lesion extending into the cerebellopontine angle cistern, and the trigeminal nerve was visualized. On magnetic resonance angiography (MRA), the encasement and medial displacement of the right internal carotid artery was noted. On diffusion-weighted imaging (DWI) scans, only a few areas of hyperintensity were observed, with the corresponding regions exhibiting a decreased apparent diffusion coefficient (ADC) (Figure 3(a)–(c)). Based on clinical and imaging findings, a differential diagnosis of Meckel’s cave tumor invasive trigeminal schwannoma and trigeminal ganglioneuroma was considered. (a)–(f): Axial magnetic resonance imaging (MRI) T2W images (a)–(c), T1W images of the brain with (a) and without (b) intravenous contrast, and SWI images of the brain demonstrating heterogeneous, predominantly cystic, lobulated hyperintense mass in the right Meckel’s cave and middle-cranial fossa (white arrows) causing encasement of the right internal carotid artery (black arrow in a), compression of the right-optic nerve (black arrow in b), and extension into the right-middle ear cavity (black arrow in c). On contrast heterogenous enhancement noted (d), (e), with areas of tiny susceptibility effects (white arrows in f) suggestive of microhemorrhages. (a)–(c): Axial balanced fast-field echo images (a), MRA maximum-intensity projection (b) and ADC (c) images of the brain demonstrating a heterogeneous mass in the right-middle-cranial fossa with a small tail of the lesion from the right trigeminal nerve in the cerebellopontine angle cistern (white arrow) in image (a) and unaffected left trigeminal nerve (black arrow), encasement of the internal carotid artery (ICA) by the mass (white arrows in b) and areas of reduced ADC (c) suggestive of restricted diffusion within the mass.
As the tumor was extensive, a right-pterionic craniotomy was planned with burr holes in the right temporal and parietal bones and debulking of the tumor was performed. A soft to firm encapsulated tumor was noted just beneath the temporal lobe, a cruciate incision was made over the tumor capsule, and central debulking was performed. Tumor was noted encasing the right internal carotid artery, with the tail of the tumor extending along the trigeminal nerve which was separated to the maximum extent and debulking with piecemeal extraction of the tumor was performed. Immediate postoperative period was uneventful, and the patient was stable. The specimens were sent for histopathological examination, which demonstrated intersecting neural cells in fascicles and mature ganglion cells with schwanion stromal background. The specimen was strongly positive for synaptophysin and schwanion background and confirmed the diagnosis of ganglioneuroma (maturing type) of the trigeminal nerve (Figure 4(a)–(d)). Unfortunately, the patient expired on the 10th postoperative day due to an unexpected sudden myocardial infarction. (a)–(d): Hematoxylin and eosin-staining images (a), (b) of the operative specimen reflecting intersecting fascicles (white arrow in a) and mature ganglion cells (white arrow in b). Immunocytochemistry examination with synaptophysin (c) and S100 (d) showing strong positivity.
Discussion
Ganglioneuromas are benign, well-encapsulated, and differentiated tumors composed of ganglion cells of the peripheral nervous system. These tumors commonly derive from sympathetic autonomic ganglia and are generally located in the posterior mediastinum and retroperitoneum, but they also involve adrenal crest cells. 1 An intracranial origin of ganglioneuromas is relatively rare, with only a few cases reported in the literature. These rare tumors typically arise from the trigeminal nerve and are detected in Meckel’s cave and the middle-cranial fossa, cerebellopontine angle, middle ear, and the internal auditory canal. 2
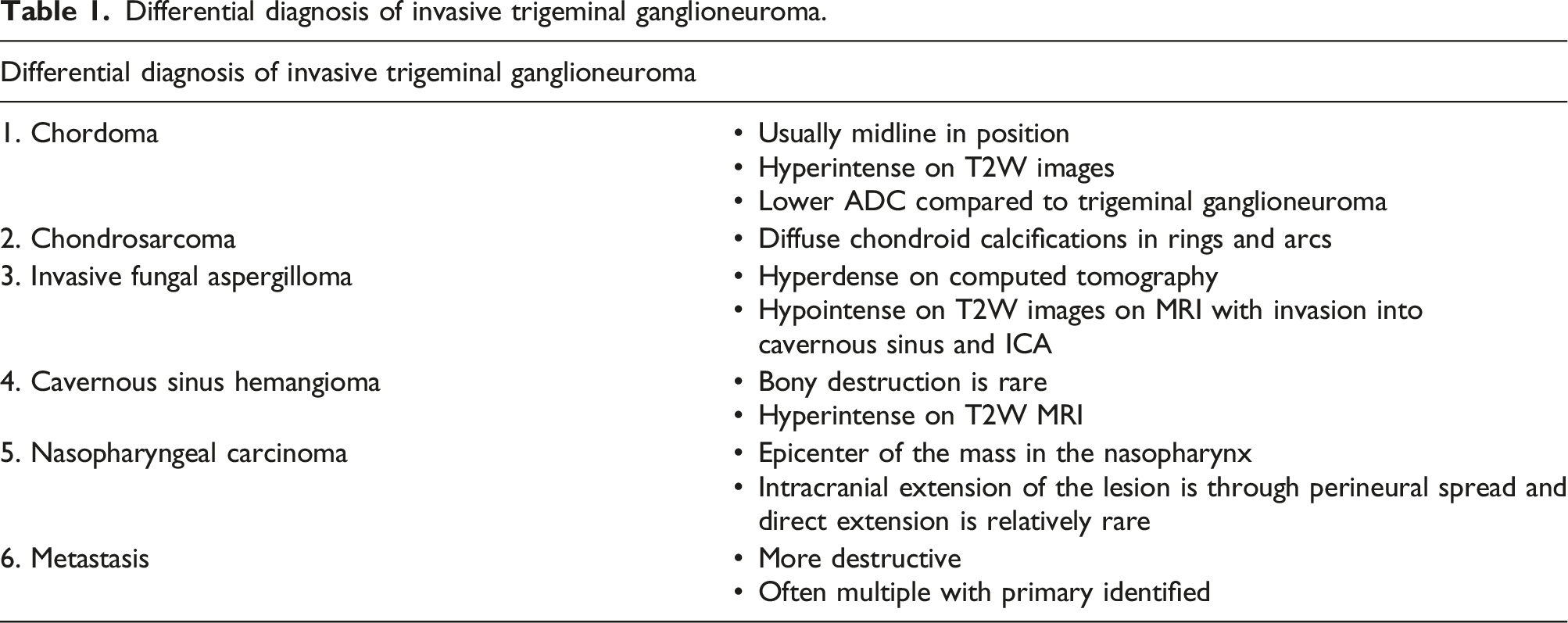
Differential diagnosis of invasive trigeminal ganglioneuroma.
Review of the literature describing the previous reported case reports.

Invasive trigeminal ganglioneuromas are well-localized tumors that may originate in the cerebellopontine angle cistern, Meckel’s cave, or middle-cranial fossa along the course of the trigeminal nerve. These tumors may promote erosion and destruction of bones adjacent to the skull base. Therefore, differentiation of the masses of the skull base and middle-cranial fossa should be considered during imaging examinations.
Footnotes
Acknowledgments
None
Author contributions
Conceived and designed the analysis: RKN, data collection: KA, contributed data/analysis tools: PN, performed the analysis: RKN, and wrote the paper: RKN.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.