
Abstract
Cerebellar abscess is a reported complication of chronic suppurative otitis media (CSOM) and is life threatening at times. It usually develops by direct spread of CSOM through the bony erosion in the petrous bone or by thrombophlebitis of the sigmoid sinus. However, an alternative pathway of infection transmission from the petrous bone to the cerebellum through the anatomical bridge of the cranial nerves has possibly not been described before. A 63-year-old female patient with CSOM and cholesteatoma developed ataxia and right facial palsy. Computed tomography (CT) showed bone erosion of the right petrous bone suggesting middle ear infection. Post-contrast MRI revealed an enhancement of swollen 7th/8th nerve complex, suggesting neuritis, and cholesteatoma in the right petrous bone. It also showed ring enhancing lesion in the cerebellar peduncle of the same side suggesting brain abscess. Surgical intervention was performed emergently and pus aspirated. She also underwent mastoidectomy and removal of cholesteatoma later by the otolaryngology team and finally got better. This case illustrates that CSOM can cause cerebellar abscess by spreading infection via anatomical bridge of the cranial nerves without direct invasion from the temporal bone or thrombophlebitis of sinus.
Introduction
Brain abscess is one of the well-known complications of chronic suppurative otitis media (CSOM). Other more common intracranial complications are meningitis and dural venous sinus thrombosis, mainly sigmoid sinus.
Despite the decrease in the incidence of intracranial complications of CSOM due to wide use of radioimagings and intravenous antibiotics, incidence of cholesteatoma seems to have remained static leading to intracranial complications.1–3 Brain abscess formation is more commonly encountered especially if CSOM is associated with cholesteatoma.1,4,5 Cholesteatoma is a common complication of CSOM occurring in more than one third of cases. 8 It erodes bone in the petrous bone leading to development of communication between middle ear and intracranial space and formation of brain abscess.3,4,6–8
Direct spread of infection through the bony defect in Tegmen plate and/or Trautmann’s triangle is a common mode. Another mode involves the development of thrombosis of sigmoid sinus which can lead to the spread of infection to adjacent area of cerebellar hemisphere. Yet another mode of infection transmission, which is the rarest one, is via the normal anatomical pathways of the 7th/8th nerve complex.
CSOM leading to labyrinthitis, erosion of fallopian canal, and thus facial nerve palsy is one of the common complications of CSOM.9,10 However, it is not common for the infection to spread to posterior fossa through the 7th/8th nerve complex leading to abscess formation in the cerebellar peduncle near the root entry or exit zone of brain stem.
Here, we present an interesting case of otogenic cerebellar abscess, possibly reported for the first time, in which the infection was transmitted from middle/inner ear via 7th/8th cranial nerves leading to abscess formation around these nerve roots in cerebellar peduncle.
Case presentation
A 63-year-old female patient who was a known case of right sided CSOM with cholesteatoma and hearing loss presented in the emergency department with gait difficulty and ataxia. She also had right ear discharge, hearing loss, and right facial palsy of lower motor neuron type, House-Brackman Grade IV. Symptoms suggested suppurative labyrinthitis. She was fully conscious without focal neurological deficits and signs of meningeal irritation.
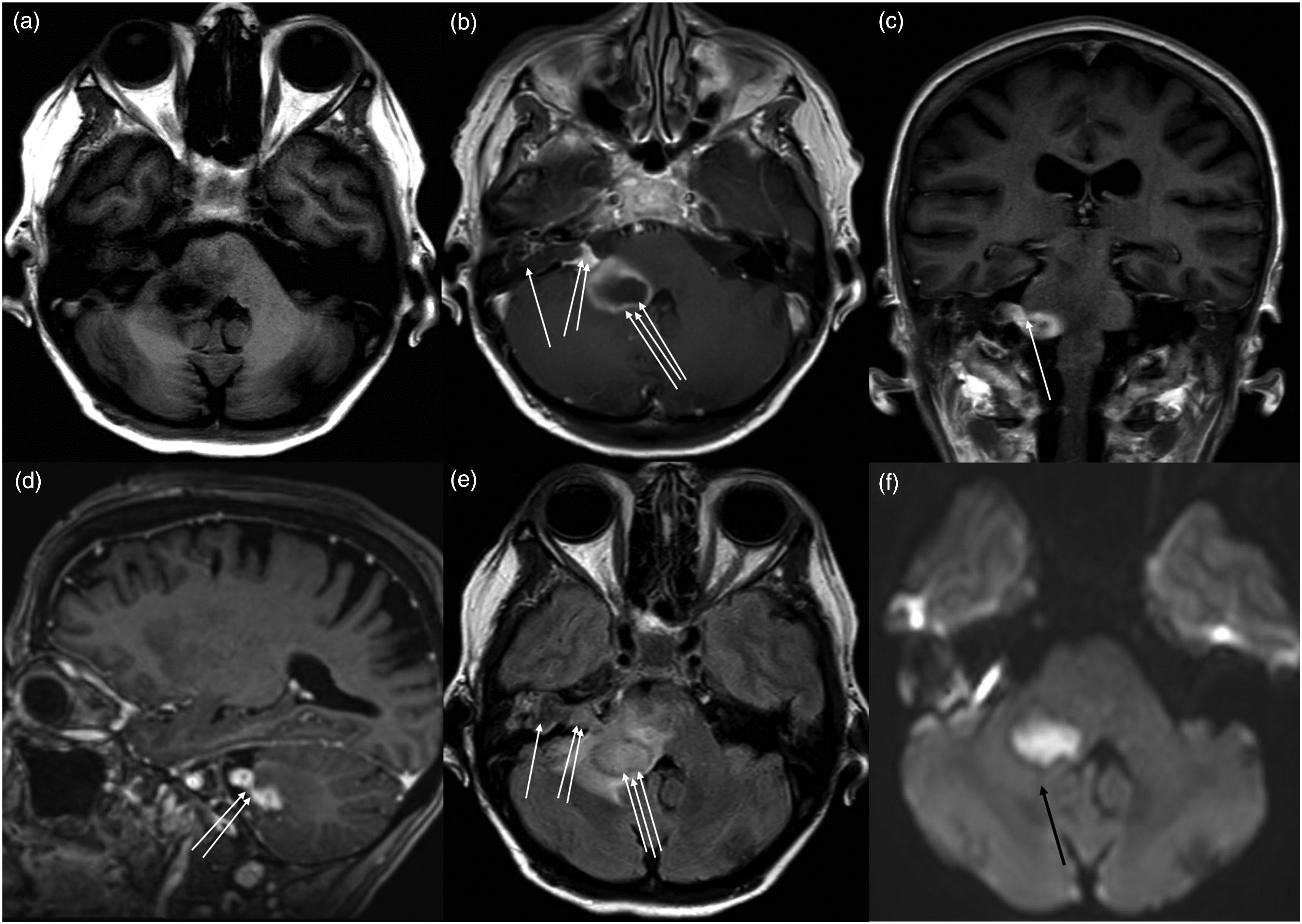
Computed tomography (CT), plain and contrast, showed diffuse ill-defined mild hypodensity around the area of right cerebellar peduncle with narrowed fourth ventricle and mild hydrocephalus. Bone window revealed bone erosion in the right petrous bone inner ear area (Figure 1). However, no bony defect was noted in Tegmen plate or Trautmann’s triangle. Preoperative magnetic resonance imaging (MRI) images (Figure 2) showed peripherally enhanced cystic lesion (19 × 21 × 22 mm3) in the right cerebellar peduncle mildly compressing the fourth ventricle. They also showed a marked enhancement of swollen 7th/8th nerve complex and an isointense minimally peripherally enhancing cystic lesion in petrous apex suggesting cholesteatoma. All the T1W contrast images of axial, coronal, and sagittal sections showed contiguous connection between cholesteatoma, 7th/8th nerve complex, and cerebellar abscess involving the adjacent area of brain stem, root entry, and exit zones. It suggests neuritis of these cranial nerves and spread of infection through their route. T2-weighted (T2W) and FLAIR images showed edema surrounding the cystic mass lesion extending up to brain stem. There was no evidence of venous sinus thrombosis in radio images. CT scan of head bone, window of axial section showing hypodense lesion in the right petrous bone suggesting bone erosion and cholesteatoma formation indicating middle and inner ear infection (arrow). Preoperative MRI images showing minimally peripherally enhanced cholesteatoma (one arrow) within the petrous bone, markedly enhanced 7th/8th nerve complex (two arrows) and the right cerebellar peduncular abscess (three arrows) contiguous with each other: (a) T1W axial section, (b) T1W axial section contrast image, (c) T1W coronal section contrast image, (d) T1W sagittal section contrast image, (e) FLAIR axial image, and (f) DWI image showing right cerebellar peduncular abscess (black arrow).
Neurosurgical evaluation was done and an emergency surgery was planned. External ventricular drainage was placed in the right frontal horn to address impending hydrocephalus. Cerebrospinal fluid (CSF) showed subtle pleocytosis (12/mm3) but negative culture. A Burr hole was made in the right suboccipital region and image-guided needle aspiration was done which revealed pus confirming brain abscess. Pus culture was also negative. Her cerebellar dysfunction improved significantly following the surgery. She underwent subsequent radical mastoidectomy by the otolaryngology team after a few days. She got completely cured afterward with residual hearing loss (Figure 3). Postoperative MRI images about 6 weeks after surgery showing resolved brain abscess in the right cerebellar peduncle: (a) T1W axial section contrast image and (b) FLAIR axial image.
Discussion
Intracranial complications of CSOM, mainly brain abscess, are still prevalent especially if associated with cholesteatoma.2,11 They are, most of the time, due to transmission of infection through bone erosion/defect and sigmoid sinus thrombosis.
Among cerebellar abscesses, involvement of cerebellar peduncle and cranial nerves root entry and exit zones seems much rarer and is possibly not yet reported. Here, we reported a rare case where the abscess was in the right cerebellar peduncle, infection being transmitted via cranial nerves route. We strongly believe that the infection was transmitted from middle ear to cerebellum through 7th/8th nerves and this is because the patient did not have signs of meningitis. Moreover, she had cholesteatoma in the middle ear suggesting chronic infection. In addition, previous literature suggests that 7th/8th nerves can be involved in CSOM causing facial palsy as in our case.
Seven H et al. reviewed 780 patients of CSOM and varieties of brain abscesses. However, they did not mention specific locations of cerebellar abscess and the mechanism of infection spread to posterior fossa. 4 They found that more than 93% of patients with brain abscess secondary to CSOM had cholesteatoma with granulation tissues and most of them had dural plate and sinus plate defects. This finding suggests that cholesteatoma is vital for the otogenic brain abscess formation and infection often spreads through the direct pathway after bone erosion. Many other case reports, series, and reviews have also shown the same findings.4,5,11,12
In most cases of otogenic cerebellar abscess, there is bony defect in Trautmann’s triangle over the sigmoid sinus leading to its thrombosis and abscess formation in its vicinity. 4 However, in rare cases, infection transmission to cerebellum can occur via cochlear fistula.13,14 Even rarely can the infection transmit through the route of cranial nerves like in our case.
Our case developed an abscess secondary to CSOM and cholesteatoma near the brain stem which is a rare location. Moreover, MRI has clearly shown the inflamed nerves, 7th/8th complex, connecting cholesteatoma, and posterior fossa suggesting infection transmission via these nerves. Our case developed suppurative labyrinthitis first which led to the inflammation of adjacent cranial nerve leading to facial nerve palsy. Finally, the infection transmitted to the posterior fossa via the infected cranial nerves forming abscess around the nerve roots. Lack of meningitis and sterile CSF rule out the possibility of retrograde infection transmission from brain to inner ear.
Several reports have presented the same pathological process of cerebellar abscess formation,10,13,14 but in their cases, cranial nerve involvement was not evident and abscess was in the cerebellar hemisphere. However, in our case, there was isolated involvement of cranial nerves resulting in abscess formation in an atypical location correlating well to the infection transmission mechanism, as we described. Contiguous appearance of cholesteatoma, cranial nerves, and abscess in MRI strongly supports. Moreover, absence of bony defect (Trautmann’s triangle defect) and sigmoid sinus thrombosis excludes other possible modes of infection transmission.
William K Karlsson described similar pathogenesis in three cases of brain abscess caused by Listeria monocytogenes where trigeminal nerve was involved. 15 This supports our hypothesis of cranial nerves bridging the infection transmission. However, in our case, no organism was isolated from abscess or CSF.
Therefore, ours’ is a report worthy case in which the infection got transmitted to cerebellar peduncle via cranial nerves.
In conclusion, otogenic brain abscess is not a new phenomenon, and various modes of infection transmission are already well known. However, infection transmission from middle/inner ear to brain via the route of cranial nerves, namely, 7th/8th nerve complex is yet another unusual mode which was seen in our case. As a result, cerebellar abscess developed in cerebellar peduncle near the nerve roots. This mode of infection transmission was possibly not reported before.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.