
Abstract
Ectopic pancreas within the mesentery is rare. In this case report, a 61-year-old man with an ectopic pancreas within the jejunal mesentery for over 20 years developed chronic pancreatitis that progressed to acute exacerbation. Our computed tomography (CT) performed for acute abdomen assessment suggested acute appendicitis or Meckel’s diverticulitis. However, a CT scan taken 20 years ago revealed a structure indicative of an ectopic pancreas in the mesentery, and further imaging findings taken 10 and 4 years ago confirmed progression to chronic pancreatitis. Furthermore, we found a pancreatic stone confined in the luminal structure that corresponded to the main pancreatic duct; this stone eventually caused acute exacerbation. In summary, we report a case of mesenteric ectopic pancreas that showed typical findings of progression and acute exacerbation of chronic pancreatitis on CT.
Introduction
Ectopic pancreas is a pancreatic tissue anatomically and hemodynamically located outside the normal pancreatic site. It appears as a submucosal lesion usually situated in the gastrointestinal tract, such as the stomach, duodenum, or jejunum. 1 Although it is generally asymptomatic and observed incidentally, it may be complicated by bleeding, intestinal obstruction, intussusception, pancreatitis, pseudocyst formation, and tumors (cancer and neuroendocrine tumors).2–5
Ectopic pancreas rarely occurs outside the gastrointestinal tract, and occurrence within the mesentery, as in the present case, is rare. 6 Although bleeding, acute pancreatitis, and cancer reportedly occur in the ectopic pancreas within the mesentery, chronic pancreatitis progressing over a long period of time and causing further acute exacerbation has never been reported.7–9
Herein, we report a case of mesenteric ectopic pancreas with chronic pancreatitis that progressed and resulted in acute abdomen caused by acute exacerbation, showing a typical course as confirmed by computed tomography (CT).
Case report
A 61-year-old man presented with abdominal pain in the hospital. Given a history of acute pancreatitis four times in the past, we suspected pancreatitis as well. Thus, the patient was thoroughly examined. The patient’s medical history included type 2 diabetes, hypertension, and dyslipidemia. Until 2 years ago, he had been smoking 40 cigarettes per day for 20 years, but he was currently in the process of quitting smoking. Four years ago, his daily alcohol intake was 350 mL of beer and one cup of shochu, but recently he had been drinking only one glass of shochu per day and had not drink alcohol for 5 days. There was no confirmed family history of pancreatic disease. Blood tests showed a mild increase in inflammatory response but no increase in pancreatic enzymes.
Contrast-enhanced CT was performed, revealing a luminal structure with calcification in the right lower abdomen and an increased fat concentration in the surrounding area, suggesting an acute inflammation (Figure 1, arrow). In addition, the adjacent intestine exhibited edematous wall thickening (Figure 1, arrowhead). We initially considered acute appendicitis, but given that this luminal structure branched from the small intestine and the appendix appeared normal, we ruled out acute appendicitis. Contrast-enhanced computed tomography (CT) image (coronal image, late phase). Luminal structures with calcification are observed in the right lower abdomen (arrow), and edematous wall thickening in the adjacent intestine (arrowhead).
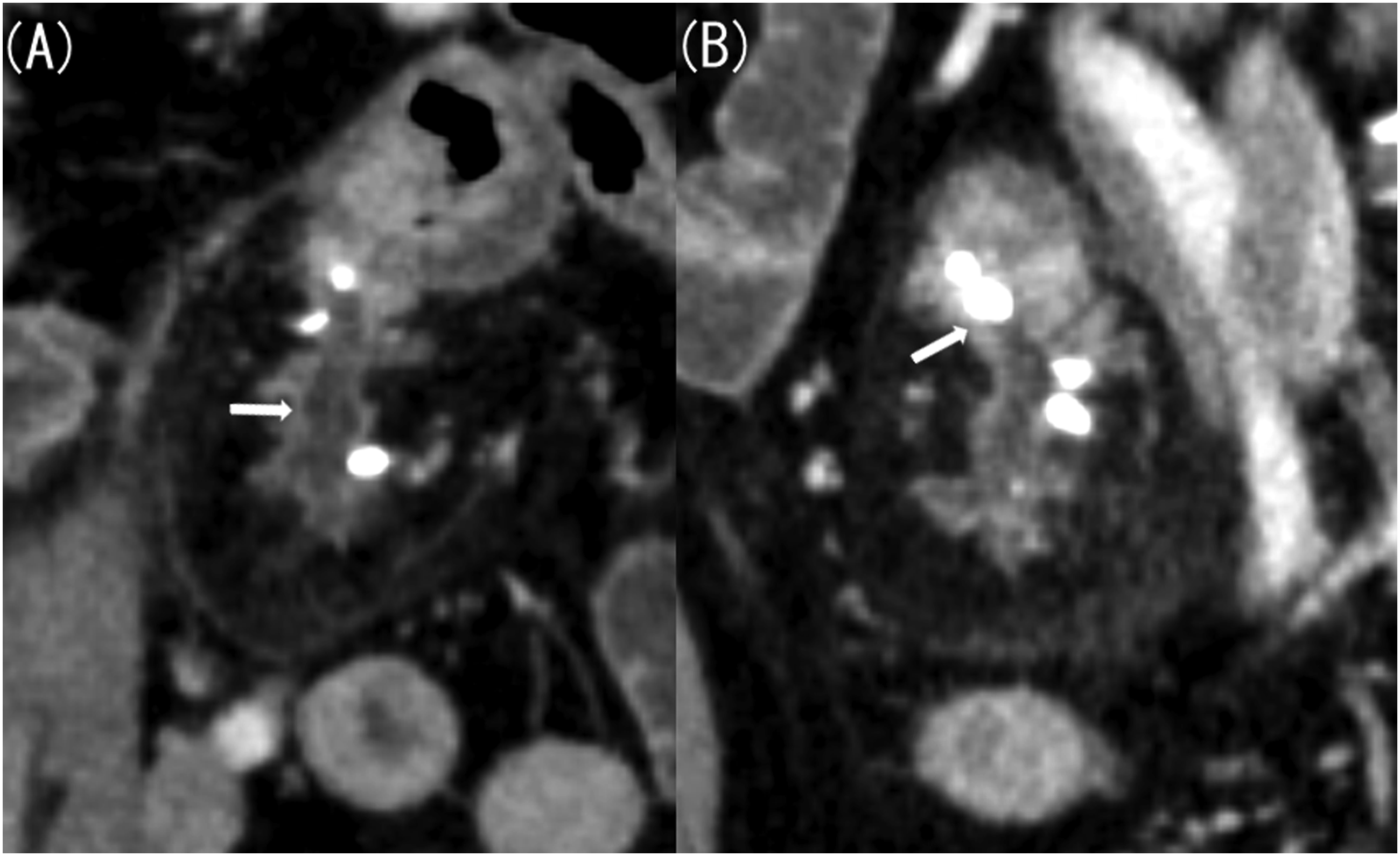
Next, we considered Meckel’s diverticulitis and confirmed the presence of Meckel’s diverticulum on previous CT scans. Contrast-enhanced CT performed 20 years ago revealed a 4 cm-long and 1.5 cm-wide lobulated structure in the left mesentery of the pelvis, resembling the pancreas (Figure 2(a)). CT scan performed 10 years ago showed that this structure had shrunk, appearing similar to an atrophied pancreas (Figure 2(b)). In a CT scan taken 4 years ago, it had further shrunk, with numerous calcifications (Figure 2(c)). The imaging findings were similar to a pancreatitis progressing to a chronic type observed in original pancreas. Additionally, the CT scan taken this time revealed dilatation of the luminal structure that corresponded to the main pancreatic duct (Figure 3(a)) and a stone being confined to the small intestine side (Figure 3(b)). This image finding indicated an acute exacerbation caused by pancreatic stone incarceration that typically occurs in chronic pancreatitis. The location of this structure was in the lower left abdomen on the CT scans taken 20 and 10 years ago, in the left abdomen on the CT scan taken 4 years ago, and in the lower right abdomen on the CT scan taken this time. A CT scan taken 20 years ago showed signs of acute pancreatitis of the native pancreas, including swelling and increased fat concentration in the surrounding area. However, there has been no change in size or shape of the native pancreas since the CT scan taken 10 years ago. (A) Contrast-enhanced computed tomography (CT) image taken 20 years ago (axial image, late phase). (B) Contrast-enhanced CT image taken 10 years ago (axial image, late phase). (C) Contrast-enhanced CT image taken 4 years ago (axial image, late phase). Contrast-enhanced CT taken 20 years ago revealed a pancreas-like lobulated structure measuring 4 cm-long and 1.5 cm-wide located in the left mesentery of the pelvis (A, arrow). Contrast-enhanced CT taken 10 years ago showed that the structure had shrunk, resembling an atrophied pancreas (B, arrow). Additionally, contrast-enhanced CT performed 4 years ago showed that the structure had further shrunk, with numerous calcifications (C, arrow). (A) Contrast-enhanced computed tomography (CT) image taken this time (coronal image, late phase). (B) Contrast-enhanced CT image taken this time (sagittal image, late phase). Compared with the CT result obtained 4 years ago, the luminal structure corresponding to the main pancreatic duct was dilated, with a stone confined to the small intestine side.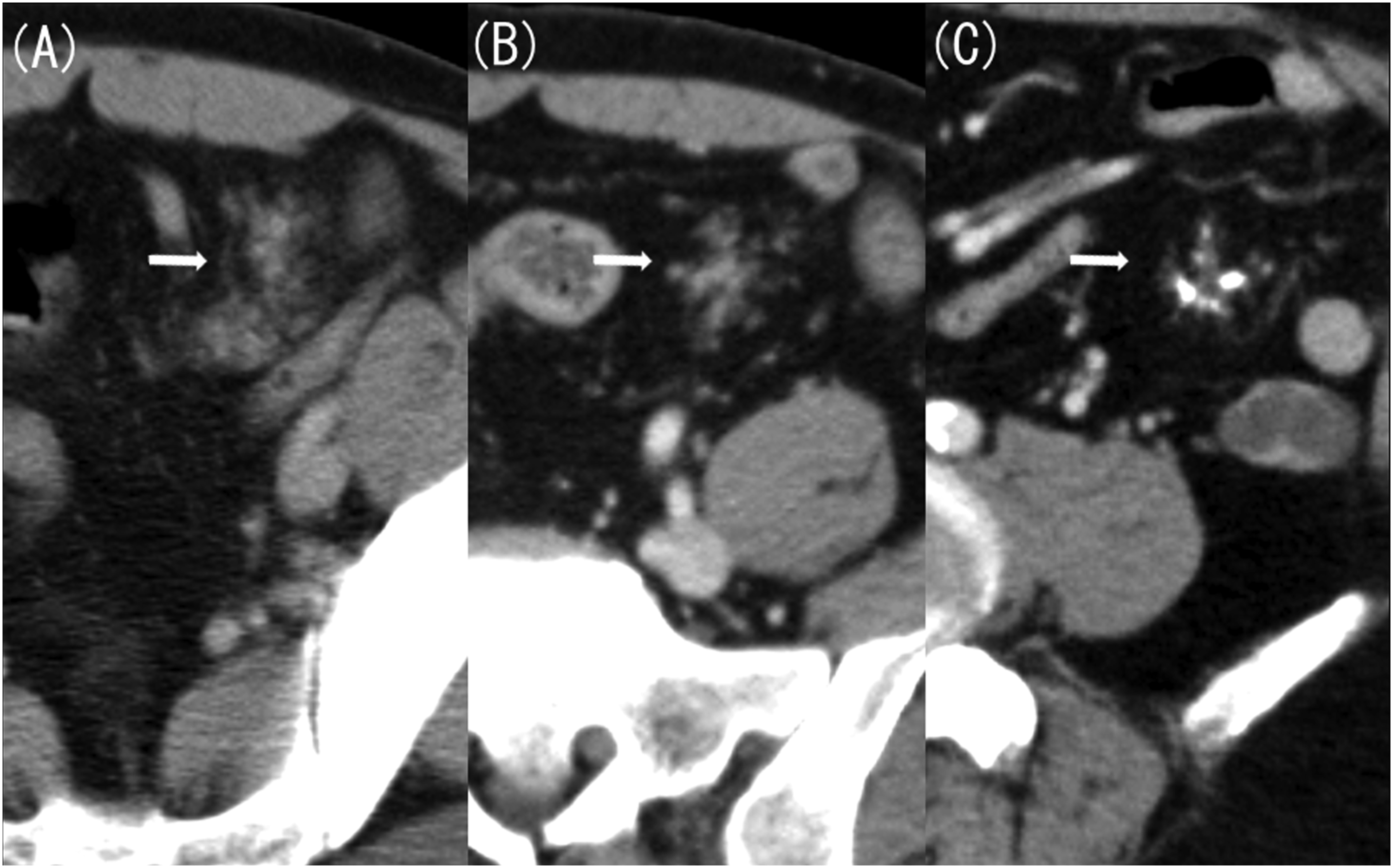
Magnetic resonance cholangiopancreatography (MRCP) taken 10 years ago also confirmed this structure. MRCP clearly depicted the luminal structure that could not be identified on contrast-enhanced CT (Figure 4(a) and (b)). (A) Magnetic resonance cholangiopancreatography (MRCP) image taken 10 years ago. (B) Contrast-enhanced computed tomography (CT) image taken 10 years ago (coronal image, late phase). MRCP clearly depicts luminal structures (A, arrow), but such structures cannot be identified on contrast-enhanced CT (B, arrow).
On the basis of these imaging findings, we diagnosed the patient with acute exacerbation of chronic pancreatitis with mesenteric ectopic pancreas. According to the imaging findings and the fact that this male patient had not consumed alcohol for 5 days, we considered pancreatic stone incarceration as the cause of the acute exacerbation of chronic pancreatitis.
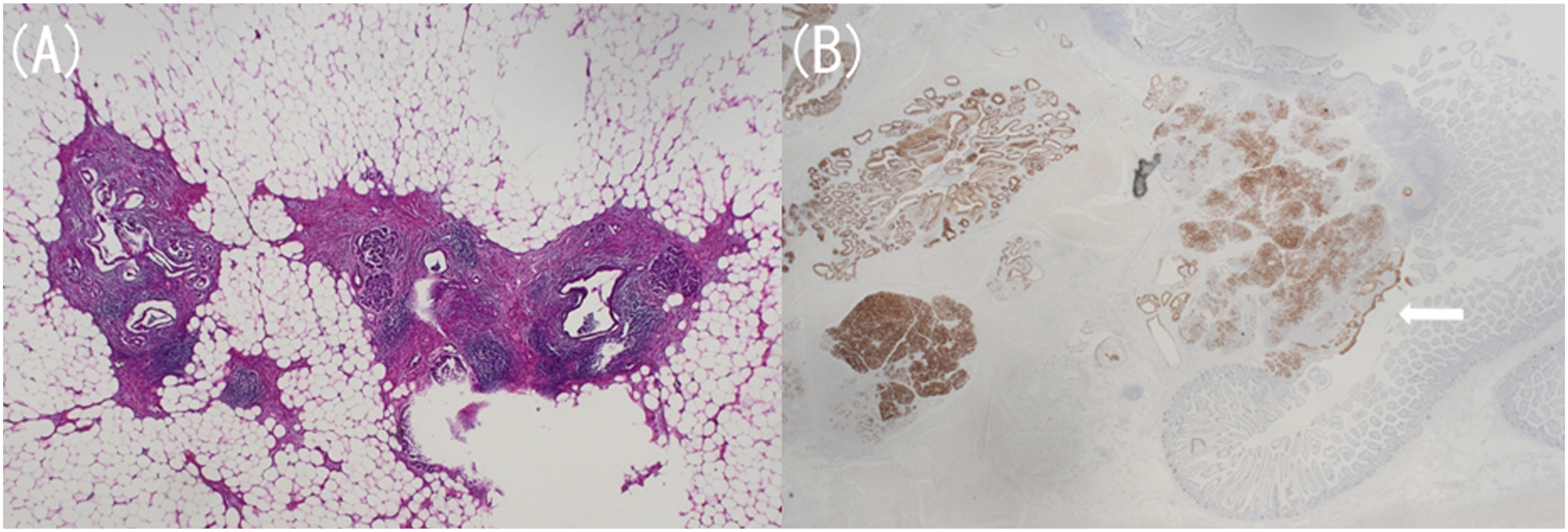
Subsequently, we performed a laparoscopic partial small intestine resection. A camera port was placed in the umbilicus using the open access technique, and the abdominal cavity was observed. A mass was located in the small intestine mesentery 50 cm from the Treitz ligament, and a small laparotomy was performed to remove the small intestine from the abdominal cavity. After confirming that there were no other lesions, we resected the mass measuring 5.4 × 5.0 × 3.5 cm, with the jejunal mesentery as the main site (Figure 5). The mass was not adhered to the surrounding area, and the surgery took 1 h and 30 min. In this site, histopathological findings revealed Heinrich’s type 2 ectopic pancreas, which was composed of ducts and acinar cells, and confirmed chronic and acute pancreatitis (Figure 6(a) and (b)). There were no complications after the surgery, and the patient was discharged 1 week later. The patient has been followed up for 2 years, but the pancreatitis has not recurred. Resected specimen. A mass measuring 5.4 × 5.0 × 3.5 cm was found in the jejunal mesentery. Pathological examination with hematoxylin and eosin staining at low magnification (A) and MUC1 staining (B). According to the Heinrich classification, this ectopic pancreas belonged to type 2, consisting of pancreatic acinar cells and ducts, with findings of pancreatitis (a). Pancreatic acini and ducts are stained within the jejunal mesentery and under the jejunal mucosa, and the pancreatic ductal epithelium is exposed in part of the small intestinal mucosa (B, arrow).
Discussion
Ectopic pancreas refers to an ectopic pancreatic tissue that is anatomically and hemodynamically distant from the original pancreas. Clinically, it is usually asymptomatic and is often discovered incidentally during unrelated surgery, imaging tests, or autopsies. 95.6% of ectopic pancreases are solitary, and multiple ectopic pancreases are extremely rare. 10
Pathologically, ectopic pancreas is pathologically classified into three types according to the Heinrich classification. 11 Type 1 includes the overall normal pancreatic parenchyma with ducts, acinar cells, and islets of Langerhans; type 2 also includes ducts and acinar cells but no Langerhans islands; and type 3 only consists of ducts.
Ectopic pancreas rarely occurs in the mesentery, and when it does exist, it often occurs in the jejunal mesentery. There have been no previous reports of multiple ectopic pancreases occurring in the mesentery, and no other ectopic pancreases were identified in our case. In cases of mesenteric ectopic pancreas without complications, surgery requirement is controversial, but the patient needs to be followed up. 12 Very rarely, bleeding, acute pancreatitis, and cancer may occur; if any of these complications occur, treatment is required.7–9
In the absence of complications, imaging diagnosis may be possible according to morphological characteristics. Mesenteric ectopic pancreas has an elongated shape with a large long-to-short axis ratio of approximately 3.0 on average. 13 Generally, it touches the outside of the intestine, becomes thinner as it moves away from the intestine, and has a conduit-like structure inside. 13 The enhancement pattern of mesenteric ectopic pancreas on contrast-enhanced CT is considered to be inconsistent because the components are different, as shown in the Heinrich classification. 13 On magnetic resonance imaging (MRI), the mesenteric ectopic pancreas is isointense to the pancreas on all sequences and has characteristically high T1 signal intensity. 14 MRCP excellently visualizes ducts, thereby useful when ducts are not clearly shown on CT.13,14
Currently, no follow-up case of chronic pancreatitis in mesenteric ectopic pancreas has been reported. However, imaging findings such as calcification, pancreatic stones, pancreatic duct dilatation, and pancreatic parenchyma atrophy, which are typical of chronic pancreatitis, may be observed, as in our case. Furthermore, acute exacerbation occurs when a pancreatic stone becomes incarcerated in the pancreatic duct, resulting in imaging findings indicating acute inflammation, such as a dilated pancreatic duct and an increased concentration of the surrounding fat.
In our case, CT showed no evidence of chronic pancreatitis in the native pancreas, suggesting that progression to chronic pancreatitis in the mesenteric ectopic pancreas is caused by factors other than heavy alcohol drinking. However, the cause was unknown because the course of chronic pancreatitis caused by mesenteric ectopic pancreas has not yet been investigated.
In conclusion, the complications of mesenteric ectopic pancreas rarely occur, but they can be diagnosed through imaging. Correct image diagnosis by diagnostic radiologists is crucial for prompt treatment planning.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.