
Abstract
Background
Uterine cavity pathology may affect the endometrium or myometrium, resulting in distortion of the uterine cavity, and is responsible for 2%–5% of infertility. The methods for its assessment usually involve imaging modalities like pelvic ultrasonography, often transvaginal-(TVS), and hysterosalpingography-(HSG), with hysteroscopy-(HSC) as the gold standard. However, HSC is not readily available in resource-poor-settings.
Purpose
To determine and compare the diagnostic accuracy of TVS and HSG in detecting uterine cavity pathology using HSC as a gold standard.
Materials and Methods
A cross-sectional analytical study of consenting infertile women for evaluation of the uterine cavity using transvaginal-ultrasonography, hysterosalpingogram, and hysteroscopy. The primary-outcome-measures were the sensitivity, specificity, and accuracy of TVS and HSG in detecting uterine cavity abnormalities using HSG as the gold standard.
Results
Eighty-eight participants were analysed for this study. The lesions confirmed on HSC were intrauterine-adhesions (43.1%), endometrial polyps (14.8%), submucous fibroids (18.2%), intrauterine-septum (13.6%), and cavity distortion (14.8%). The overall sensitivity with TVS was 57.7%, with a specificity of 97.6%, a positive-predictive-value (PPV) of 88.2%, and a negative-predictive-value (NPV) of 88.2%, giving a percentage-accuracy of 88.2%. In comparison, HSG had a sensitivity of 72.1%, a specificity of 99.4%, a PPV of 97.4%, and an NPV of 92.0%, giving an overall accuracy of 92.9%. The detection rates of TVS and HSG in this category were: fibroids (97.7% vs 89.8%; p = .0004) and adhesions (73.9% vs 87.5%; p = .0002), respectively.
Conclusion
HSG appears to be the superior modality for detection of obliterative uterine cavity pathologies, while TVS is better suited for myometrium and endometrial lesions.
Keywords
Introduction
Infertility remains a common cause of marital disharmony, especially in developing countries where a high premium is placed on childbearing. It is the failure of a couple to conceive (regardless of cause) after 1 year of unprotected intercourse. 1 The incidence of infertility varies in the different regions of the world, being highest in the so-called infertility belt of Africa. 2 In contrast to an average prevalence rate of 10%–15% in developed countries, the prevalence of infertility has been highly variable in sub-Saharan Africa, ranging from 5%–46%. 2
Uterine abnormalities remain one of the major causes of female infertility. The development of the müllerian ducts determines the normal anatomic configuration of the uterus, fallopian tubes, cervix, and upper vagina. Uterine abnormalities may be associated with impaired implantation or with pregnancy waste and premature delivery. These factors could be congenital or acquired abnormalities that may affect the endometrium or myometrium, resulting in distortion of the uterine cavity, and are responsible for 2%–5% of infertility cases.1,3 The full spectrum of congenital-müllerian abnormalities varies from total absence of the uterus and vagina (Rokitansky-Küster-Hauser syndrome) to defects such as bicornuate, septate, and arcuate uteri. Acquired pathologies like submucosal and intramural fibroids affect 25%–50% of women, mostly of African descent, and can cause distortion of the cavity and compromise the blood supply. Intrauterine adhesions occur due to endometritis associated with a traumatic delivery, dilatation and curettage in termination of pregnancy, an intrauterine device, or any instrumentation of the endometrial cavity with partial or total obliteration of the cavity. 4 Intracavitary lesions are implicated as causes of infertility, and their removal may increase fertility. Overall, pregnancy rates of 50%–78% in previously infertile women have been reported after hysteroscopic polypectomy.
Assessment of the uterine cavity and fallopian tube patency is a standard practice in the baseline infertility workup. 3 More so, there is increasing demand for assisted reproductive technology such as intrauterine insemination and in vitro fertilisation-embryo transfer, and the normalcy of the uterine cavity plays a vital role in the success of these procedures as the ultimate destination of the resultant gestation. The methods for assessing the uterine cavity usually involve imaging modalities such as pelvic ultrasonography, often TVS, HSG, and pelvic magnetic resonance imaging (MRI) by radiologically delineating the outline and continuity of the endometrium. However, HSC is considered the gold standard tool for assessing and determining the outline, structure, and definitive abnormalities within the uterine cavity, with the additional benefit of operative treatment and correction of some of these problems through its minimal access point of view. This is also complemented by the laparoscopic approach. A combination of these methods would usually be required while evaluating an infertile patient. 5
The application of the methods for uterine structure and cavity assessment is subject to their availability and affordability, especially in the developing world. Pelvic ultrasonography and HSG have long stood as baseline investigative modalities during fertility evaluation of patients in resource-poor settings, with the more recent introduction of technically demanding though minimally invasive hysteroscopic and laparoscopic procedures. However, HSC is not readily available to a larger portion of the population due to the cost of the equipment and the procedure, as well as the skill to perform it, and there is still reliance on the radiological modalities in ruling out intracavitary abnormalities. But can they confirm or exclude the presence of lesions within the uterine cavity or reliably adjudge the adequacy of the cavity for fertility? And if so, how well do they measure up to hysteroscopic evaluation?
This study therefore aimed to determine and compare the accuracy of TVS and HSG in detecting uterine cavity abnormalities, justifying their relevance as a singular tool or in combination, and using HSC as the gold standard.
Materials and methods
Study design
This was a cross-sectional analytical study.
Study setting
The study was carried out at Nnamdi Azikiwe University Teaching Hospital (NAUTH) in Nnewi, Nigeria, between August 2019 and March 2020.
Study population
This was conducted among infertile women who presented to the gynecologic clinic of NAUTH following informed written consent.
Inclusion criteria
All women with infertility who presented to the clinic and gave their consent were included in the study.
Exclusion criteria
Those excluded from the study were patients with possible pregnancies at the time of evaluation, women with pelvic inflammatory disease at the time of evaluation, women with active vaginal bleeding, women with gynaecological cancers, women with cervical stenosis, adverse reactions to anaesthesia, and those who refused to give consent.
Recruitment of participants and data collection
The participants were recruited from gynaecology-endoscopy subspecialty units. Following history-taking and evaluation of the inclusion and exclusion criteria, eligible patients were counselled for the study by the researchers, and written consent was obtained. A structured proforma was designed that was used to capture the biodata of the patients, clinical features, TVS findings, HSG findings, and HSC findings.
Sample size determination
According to the study by Ugwu et al., 6 the institution’s incidence of infertility was found to be 5.5%. The minimum sample size was calculated using the formula N, where N sample size, Z standard normal deviation at 95% confidence interval, which is 1.96, d degree of precision set at 0.05, P proportion of the target population, and Q = alternate proportion (1-P). Using a prevalence rate or proportion of infertility among patients of 5.5%, according to a study by Ugwu et al., 6 which provided for a 10% attrition rate, the minimum sample size was 88 participants.
Procedure
Having counselled participants on the details of the procedure. The TVS was scheduled at a convenient time. This was performed using a 5.0 MHz transvaginal probe of the LOGIQTM V2 (2015) ultrasound system, a product of GE Healthcare (General Electric Company) with factory calibrations for gynaecological examinations rendered in a two-dimensional (2D) plane. The patient was asked to void before the procedure. She was then asked to lie on the examination couch with her lower limbs flexed at the hips and knees, with the legs apart. Coupling gel was applied at the tip of the probe, and a latex condom was rolled over the length of the probe from its tip. The gel was again reapplied on the tip after this. The probe was gently inserted into the vagina and pushed into the anterior fornix, against the cervix and the anterior surface of the uterus. This presented a sagittal view of the uterus and its cavity, and a horizontal sweep was also done (see Figure 1). Details of interest, including the cervix, the endometrial cavity (endometrial strip continuity, thickness, and length), and myometrial to intracavitary masses, can be ascertained in this view. The probe was rotated 90° anticlockwise, and a vertical sweep was also done. The probe is then angled towards the left and right iliac regions to assess the adnexal structures. The findings were recorded. Transvaginal sonogram showing the long axis of the uterus and endometrial lining.
The HSG was done in the preovulatory phase of the menstrual cycle, observing the 10-day rule. Pre-procedure oral diclofenac 50 mg was given. Approximately 5–10 mL of a water-soluble contrast medium (Pielograf) was introduced under fluoroscopy guidance into the uterine cavity after placing a Spackman’s cannula through the cervical os. Digitalized spot radiographs were systematically obtained, including an underfilled view of the uterus to detect small endometrial lesions, an early filled view of the fallopian tubes, both anteroposterior and oblique projections of the entire genital tract showing the spill of contrast material at the peritoneum, and if there is loculated spillage, a delayed radiograph. Filling defects and uterine wall irregularities were the two main outcome measures. The findings were recorded. See Figures 2(a) and (b). Hysterosalpingogram showing filling defects due to submucous fibroid (a) and narrowed cavity with endometrial polyp (b).
Following clinical evaluation, a TVS scan, and a HSG, the patients were scheduled for diagnostic HSC. This was usually done in the immediate postmenstrual phase. However, for amenorrhoeic women, it was done at any convenient time. Misoprostol (100 ug) was given sublingually a night before the procedure in the nulliparous women to aid cervical os dilatation. It was done in the gynaecology suite of the main theatre, usually under general anaesthesia, as we also did laparoscopy and dye testing in the same setting on a number of the patients. A 5.5-mm diagnostic hysteroscope sheath was used under fluid distension with 0.9% normal saline. The patient is placed in a semi-lithotomy position with routine perineal cleaning and draping. The hysteroscope is assembled and checked for proper functionality. With Sim’s speculum applied, the hysteroscope is inserted into the vagina under direct vision and advanced towards the cervix. With fluid distension initiated, it is gently pushed through the external Os into the cervical canal and then further into the uterine cavity. There was a systematic survey of the cervical canal, cervical os, and uterine cavity, including the fundus, the anterior and posterior walls, and the lateral walls. The tubal ostia were then examined.
The observed pathologies were categorised appropriately. See Figure 3(a) and (b). Myometrial abnormalities were categorised as submucous fibroids; endometrial abnormalities as polyps or cysts; cavity distortion (e.g. synaechia and stricture), or nonspecific asymmetry; and tubal abnormalities as ostial or proximal tubal obstruction. The findings were recorded. Diagnostic hysteroscopy showing intrauterine septum (a) and submucous fibroid (b).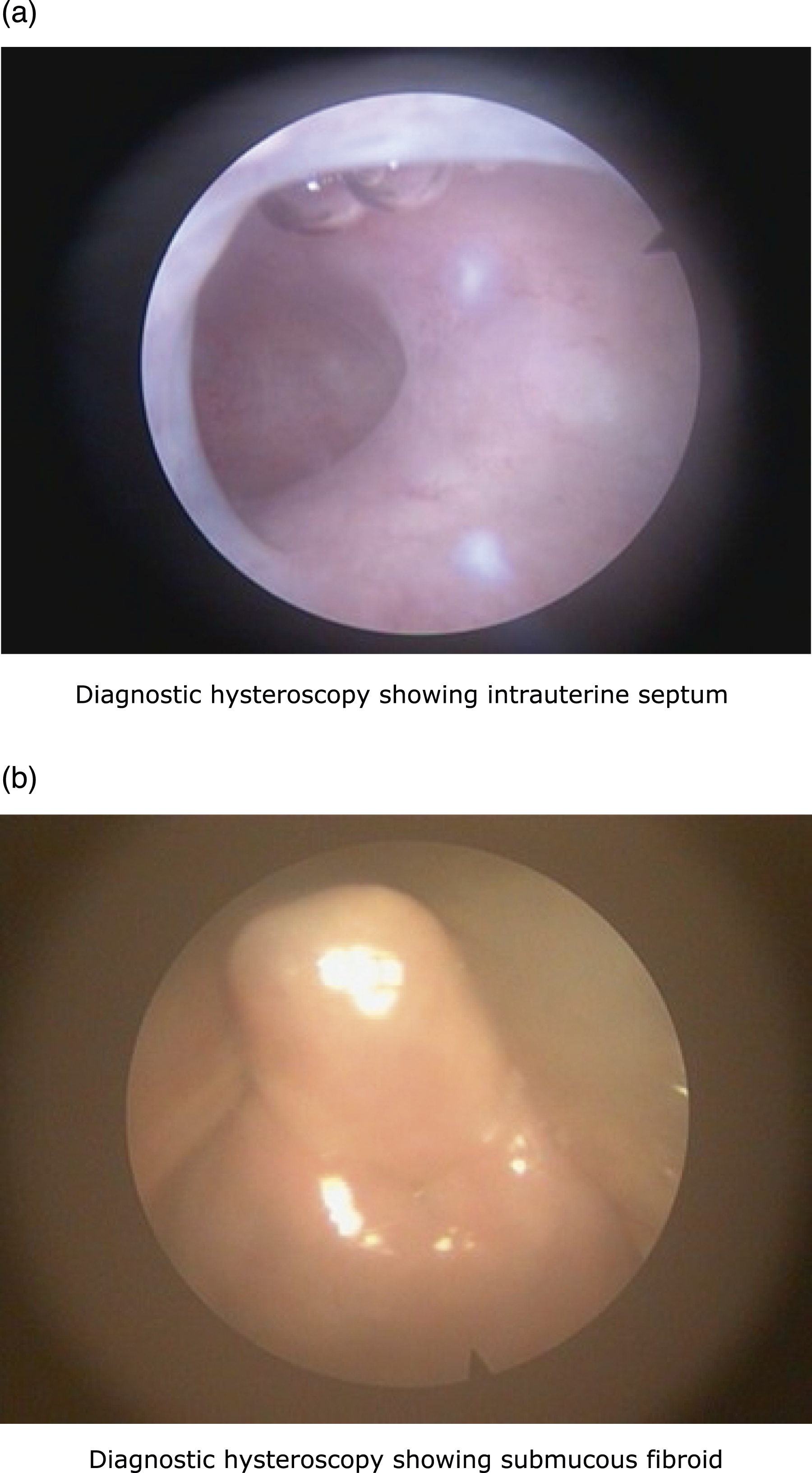
These three procedures were performed on all the women included in the study. The order of recruitment was based on the sequence of presentations. However, the timing of the procedures was convenient, and the sequence was mostly as stated.
Data analyses
The data was processed and analysed using Software Package for Social Sciences (SPSS) version 26. The data was statistically represented by the terms range, mean, standard deviation (+SD), and percentages. The abnormalities were categorised, and for each abnormality, the frequency of detection by each modality (TVS, HSG, and HSC) was tabulated with hysteroscopy as the gold standard. Measures of accuracy used include sensitivity, specificity, positive predictive values, negative predictive values, and percentage accuracy. The Pearson chi-square test and Fisher exact test were used for tests of significance, where a p-value of <0.05 was considered significant at a 95% confidence interval.
Result
A total of 99 patients were assessed for eligibility during the study period. Three of the women did not give consent. One was excluded due to ultrasound features suggestive of chronic pelvic inflammatory disease with a tubo-ovarian abscess. One of the women could not have HSG done due to acquired cervical stenosis, and two of the women could not have HSC due to anaesthetic complications. Five other women were too lost to follow-up. Hence, 11 women were excluded from this study. Therefore, 88 successfully completed all three of the procedures, and their data was used for data analysis. The recruitment and evaluation of the women lasted approximately 8 months. Figure 4 shows a flow diagram describing how the participants flow through. Flowchart of study participants.
Biosocial characteristics of the women.

Clinical characteristics of the women.

Frequency of pathologies diagnosed.

Overall detection of uterine cavity findings.

Comparison of TVS and HSG detection rates.

TVS: Transvaginal Ultrasonography, HSG: Hysterosalpingography, PPV: Positive Predictive Value, NPV: Negative predictive value.
Discussion
The principal finding in this study is that HSG has an overall better accuracy than transvaginal TVS in the detection of uterine cavity pathologies. We found the overall accuracy of HSG to be 92.9%, the sensitivity 72.1%, the high specificity 99.4%, the PPV 97.4%, and the NPV 92.0%, while the overall accuracy of detection with TVS was calculated at 88.2%, with a sensitivity of 57.7% and a specificity of 97.6%, a positive predictive value of 88.2%, and a negative predictive value of 82.8% in diagnosing abnormal uterine cavity findings, which included submucous fibroids, polyps, intrauterine adhesions, septa, and other distortions of the uterine cavity. Despite the fact that this study has shown that both TVS and HSG are able to detect decent percentages of uterine cavity pathologies during fertility assessment of women, HSC assessment revealed additional findings that were not diagnosed with either TVS, HSG, or both.
Furthermore, our results indicate that HSG is the superior modality for the detection of obliterative pathologies of the uterine cavity, such as adhesions and septations, while TVS is better suited for myometrial and endometrial lesions. This was similar to the findings documented by Phillips et al. 7
Pelvic ultrasonography is usually the first-line imaging tool to assess the uterus and its cavity. Its detection of intracavitary pathologies is observer-dependent as well as dependent on the display resolution, among other device specifications. The findings in this study are comparable to those by Loverro et al. 8 and had an accuracy agreement of 86%, as TVS showed a sensitivity of 84.5%, a specificity of 98.7%, a positive predictive value of 98.0%, and a negative predictive value of 89.2%. Conversely, Vitner et al. 9 found a higher sensitivity of 98% for detecting uterine cavity abnormalities, but specificity was low, at 53%.
HSG represents a different approach to the uterine cavity. An advantage of HSG is its provision of indirect evaluation of not only the uterine cavity but also the fallopian tubes. Patient discomfort, use of contrast mediums, and ionising radiation are drawbacks of the technique. Previous studies investigating the diagnostic value of HSG yielded conflicting results, and taking HSC as the gold standard in the diagnosis of intracavitary pathologies, these studies showed highly variable results: sensitivity 21%–98%, specificity 15%–85.2%, PPV 28.6%–69.9%, and NPV 83.7%–95%, with a reported agreement range between 43% and 73%.10–13 We found the overall percentage accuracy to be 92.9%, the sensitivity 72.1%, the high specificity 99.4%, the PPV 97.4%, and the NPV 92.0%.
Diagnostic HSC can even be performed in an office setting as a short procedure with direct visualisation of the cervical canal, uterine cavity, and tubal ostia, and sometimes gives the opportunity to intervene in the diagnosed pathology without remarkable patient discomfort. In this study, however, we performed our diagnostic HSC in the gynaecological theatre and employed the use of general anaesthesia in most of the procedures.
Other findings in our study demonstrated that 56.82% of the women had primary infertility and 43.18% had secondary infertility. The proportion of women with primary or secondary infertility was found to be comparable with other studies.14,15 The abnormal uterine findings were 79.31% in women with secondary infertility and 74.68% in women with primary infertility. Although the abnormal findings were more common in women with primary infertility, the difference was not statistically significant (p value = .291). Ibinaiye et al. 16 also did not find a significant difference between the two groups (p value = .077).
In the present study, TVS found an abnormal cavity in 37.5% of women, while HSG showed an abnormal uterine cavity in 51.1%, and 76.1% of the women had abnormal uterine cavity findings on HSC. The high rate of abnormalities confirmed on HSC is similar to 61.1% by Ajayi et al. 17 in the south-west; 70.4% by Blinded for Anonymity et al. 18 in the south-east; and Okohue et al., 19 who reported 77.0% among infertile women in south-south Nigeria.
Considering the categories of abnormalities detected, intrauterine adhesions were the most common findings confirmed on HSC, and this is similar to previous works in Nigeria.17,18,20 These adhesions could be caused by infectious or iatrogenic trauma to the basal layer of the endometrium, causing scarring of the endometrium as well as obliteration of the cavity. The common precipitating events include dilatation and curettage for pregnancy-related events, uterine surgeries such as myomectomy, and caesarean sections. 21 TVS had a lower accuracy in detecting it at 73.9% in this study, while HSG had 87.5% accuracy. The presence of intrauterine adhesion on ultrasonography is usually inferred by an incontinuous or non-distinct endometrial strip on ultrasonography. A thinned-out appearance of endometrium was, in some cases, a misdiagnosis of these adhesions. The false-negative findings on HSG were attributable to mild intrauterine adhesions, which were seen on HSC. The reproductive consequences of intrauterine adhesions include recurrent miscarriages, infertility, an increased risk of ectopic pregnancy, abnormal placentation, and preterm labour. 22
In the detection of intracavitary masses, that is, submucous fibroids, with TVS, we found accuracy levels of 93.8% and 94.4%, representing both high sensitivity and specificity. On ultrasound, submucosal fibroids are typically seen as broad-based, hypoechoic, well-defined, solid masses with shadowing. Submucosal fibroids typically have an overlying layer of the echogenic endometrium, which helps confirm their sub-endometrial location and helps distinguish them from endometrial polyps, which are localised overgrowths of the endometrium, which may be single or multiple. The true incidence of endometrial polyps in the general population is uncertain because many of them are asymptomatic and discovered during routine evaluation of infertile women. The overall accuracy of 97.7% shows a characteristic advantage of TVS in ruling out sizable myometrial masses abutting or occupying the uterine cavity. HSG, on the other hand, has a lower sensitivity of 56.3% and 53.8%, despite a high calculated accuracy for submucous fibroids and polyps at 89.8% and 92.1%, respectively. Rotation of the uterus, air bubbles, mucus, or blood clots in the cavity can contribute to false positive findings on HSG, as the radiographs are representations of a singular plane view of the uterine cavity. The orientation of the uterus, such as marked anteflexion of the uterus, may hide the uterine septum, whereas endometrial polyps, submucous myoma, and focal intrauterine adhesions can be missed owing to excessive injection of contrast medium into the uterine cavity, especially with smaller masses that are less than 1 cm. Similar findings were inferred in studies by Babacan et al. 23 The mechanisms through which polyps cause infertility are postulated to include inflammatory endometrial responses, endometrial cavity distortion, irregular endometrial bleeding, interference with endometrial receptivity, and obstruction of sperm transport. 24
Uterine anomalies can be seen as variations of Mullerian dysgenesis. Though some may pose no consequence to fertility, others may manifest as factors contributing to subfertility. The proposed classification by Buttram and Gibbons (1979) as revised by the American Society of Reproductive Medicine seems to be the most widely accepted and used worldwide. 25 The classes tend to be grouped by structural similarities and descriptions; however, this is not comprehensive as certain rare varieties are still not captured within it. One limitation of this classification is that it does not specify the diagnostic methods or criteria that should be used to diagnose the anomalies, and as a result, this is solely based on the subjective impression of the clinician performing the test. The European Society of Human Reproduction and Embryology (ESHRE) and the European Society for Gynaecological Endoscopy (ESGE) established a CONgenital UTerine Anomalies (CONUTA) Working Group (2012), which further proposed modifications to the classification based on uterine anatomical deviations deriving from the same embryological origin. 26
In this study, certain cavitary distortions were found, which included the uterine septum, arcuate uterus, bicornuate uterus, and unicornuate uterus. TVS showed low sensitivity (33.3%) in detecting intrauterine septum, as without distending the uterine cavity, it is more subjective in determining the variety of distortion, especially if the outer body of the uterus is not involved in the anomaly. HSG performed significantly better in displaying septations of the uterine cavity, with a sensitivity of 66.7% and an accuracy rate of 95.5%. They both showed excellent specificity, yet HSG gave superior accuracy and predictive values.
Apart from congenital variations, other cavitary distortions are further contributed to by dense adhesions causing narrowing of the endometrial cavity, which may be a fallout of previous uterine surgeries such as myomectomy. However, an arcuate uterus appeared to be a common finding in seemingly normal cavities. Furthermore, in addition to direct hysteroscopic assessment, a peritoneal cavity laparoscopic approach complements the intracavitary findings to appropriately classify the anomaly.
The strengths of this study include the fact that it is one of the first studies in Nigeria to evaluate the outline comparison between TVS and HSG in this regard. Again, there was blinding of the radiologists who performed the HSG, as they were not privy to the sonographic findings prior to this procedure. Also were the efforts to ensure that all the clients had the three modalities of assessment done on them, as this made for an accurate comparison of detection rates. However, the limitations of this study were that the ultrasonography machine used was setup for two-dimensional (2D) imaging. Recent advancements with the advent of three-dimensional (3D) and even four-dimensional (4D) imaging make it possible to render a virtually constructed image of the uterine cavity. This has been found to significantly improve the detection of intracavitary abnormalities.27,28 Also, there were no additional cost-effectiveness analyses done to further define the roles of these modalities in resource-poor environments.
In conclusion, HSG is found to be an overall superior modality for the assessment of uterine cavity abnormalities when compared with TVS. However, HSG appears to be better for the detection of obliterative pathologies of the uterine cavity, such as adhesions and septations, while TVS is better suited for myometrium and endometrial lesions. The diagnosis of uterine cavity pathologies remains a relevant aspect of assessment for fertility and conception, with identifiable challenges, especially in low-resource settings. Reliance on the available modalities becomes inevitable in excluding significant intrauterine abnormalities, and the assessed modalities have shown encouraging results despite their limitations, with TVS having pre-set machine specifications and requiring a keen sonographic eye and HSG demonstrating filling defects that are position and orientation dependent. Again, the accuracy in diagnosis of the modalities is also interpreter-dependent, as the level of experience does impact the precision in identifying various abnormalities.
Where available and feasible, patients should benefit from evaluation with these modalities. In resource-poor settings and developing countries like ours, where facilities and skills for hysteroscopy may not be readily available, TVS and HSG are valuable tools for uterine pathology evaluation. However, clinical presentation and assessment should serve as a guide to the relevance and applicability of the investigative tool. Further studies would be required on a multi-centre scale to validate our finding and evaluate the cost-effectiveness of uterine cavity abnormality assessment.
Footnotes
Acknowledgements
The authors are grateful to the study participants and the staff of NAUTH Nnewi, Nigeria, that participated in the study.
Author contributions
Ifeanyi O. Okonkwo = Principal investigator was involved in conceptualization and design, manuscript writing, revision and data collection
George U. Eleje = Supervision, manuscript writing, and revision
Chigozie G. Okafor = Manuscript writing and revision, supervision, and data collection.
Nworah J. Obiechina = Supervision, manuscript writing, and revision
Joseph O. Ugboaja = Supervision, manuscript writing, and revision
Chisolum O. Okafor = Supervision, manuscript writing, and revision.
Ikechukwu I. Mbachu = Manuscript writing and revision
Hillary I. Obiagwu = Manuscript writing and revision, data collection, and analysis
Ayodele O. Okwosa = Manuscript writing and revision, data collection, and analysis
Daniel N. Onwusulu = Manuscript writing and revision
Chukwunwendu F. Okeke = Manuscript writing and revision
Chidinma C. Okafor = Manuscript writing and revision, data collection, and analysis
Chukwudi A. Ogabido = Manuscript writing and revision, data collection, and analysis
Chukwuemeka J. Ofojebe = Manuscript writing and revision
Chinedu L. Olisa = Manuscript writing and revision, data collection, and analysis
All the authors contributed substantially to the final draft, revision, and approval of the manuscript for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
The data used for this study is available following a request from the authors.