
Abstract
Background
Magnetic resonance imaging (MRI) of the cervical spine is one of the routine MRI scans of the cervical region in investigating spinal disc pathologies, spinal stenosis, and the detection of spinal lesions, which are the major parameters to be evaluated in this examination.
Purpose
The authors of this study are focused on a different aspect of cervical MRI, revealing the incidences and reporting rates of extraspinal incidental findings.
Methods
A total of 1000 patients (324 males, 676 females, mean age 47 ± 14) who had undergone an MRI of the cervical spine were enrolled in this study. The magnetic resonance (MR) images of these patients were re-interpreted with respect to the incidental extraspinal imaging findings. The incidence and reporting rate of each incidental finding encountered during the evaluation were presented in percentages.
Results
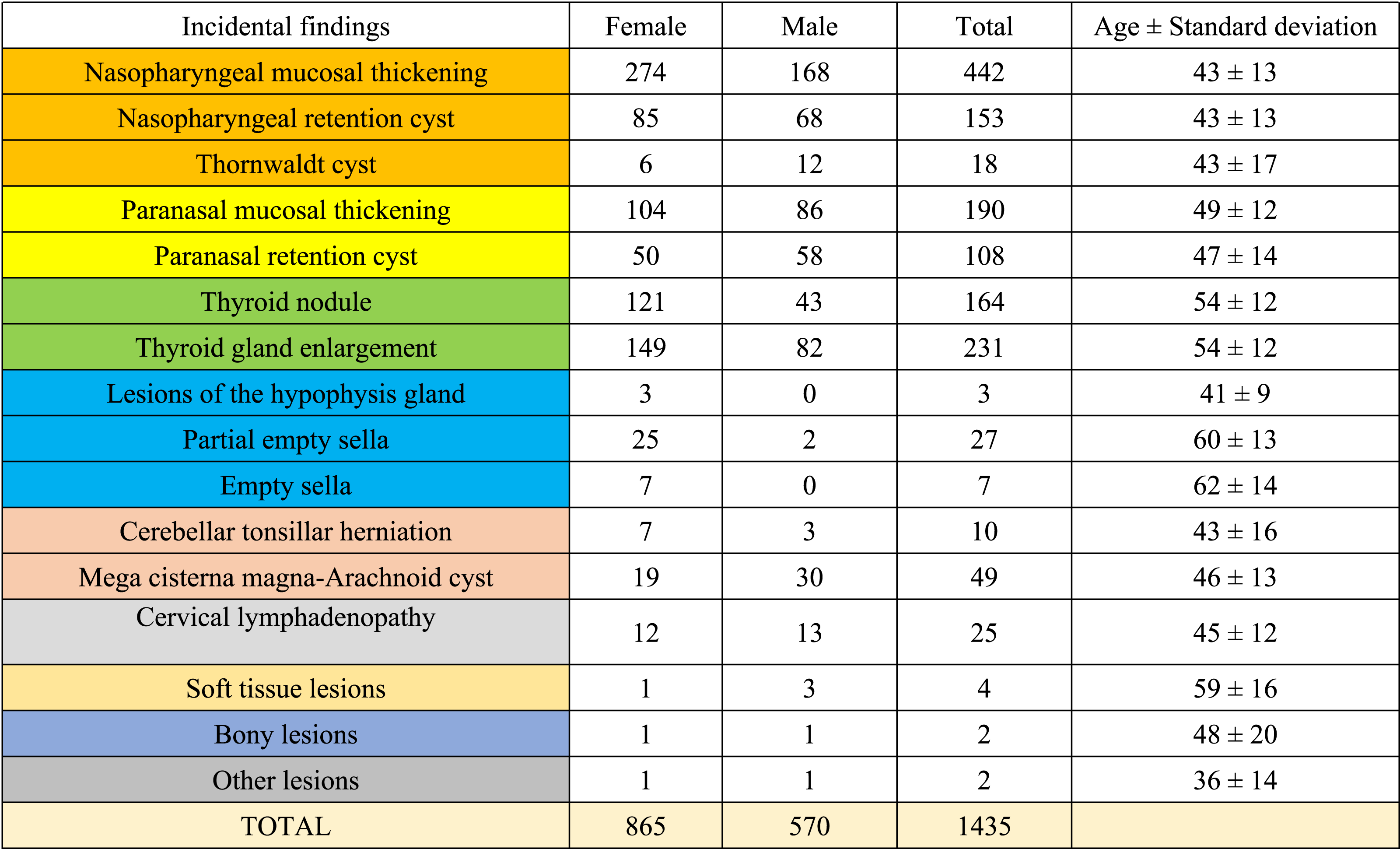
726 patients in this study had at least one incidental lesion. The results of this study revealed that the most common incidental lesions encountered during the reinterpretation of cervical MRI were nasopharyngeal mucosal thickening (n = 442) and thyroid hypertrophy (n = 231). The total reporting rate of incidental findings was 5.29%.
Conclusion
There are many data to be reported and evaluated by MR imaging of the cervical spine, not only the main parameters of MRI scanning in the routine daily practice of radiologists. All our colleagues should be aware and careful of these incidental findings, which may be the initial medical data of the patients’ diagnoses, or to avoid undesirable medicolegal problems.
Introduction
A radiological image should be interpreted according to certain parameters which are related to the purpose of the examination. An incidental finding is an unexpected abnormality encountered in the field of view of the image and an unrelated finding to the major parameters to be reviewed according to the aim of the examination.
Magnetic resonance imaging (MRI) provides excellent images and soft tissue contrast expediently to detect spinal lesions, intervertebral disc pathologies, and the assessment of the spinal canal and neural foramina. On the other hand, neck anatomy is complex and constitutes many organs and tissues in the paravertebral region. Aside from the assessment of major lesions or pathologies which might be the cause of radiculopathies or other neurological symptoms, various tissues, organs, and systems lay in the field of view of a cervical MRI. This situation brings an advantage to providing a detailed image and detecting many more lesions other than the cervical spine and spinal canal. However, much more care should be taken, and a meticulous review should be done not to neglect these unexpected lesions or signal alterations.
It is crucial for the radiologist to determine whether the incidental finding needs further investigation, a follow-up, or just a lesion to be mentioned in the radiology report. Reporting incidental findings might have a significant impact on patient management and may be more significant than the diseases of the cervical spinal column. 1
This study aims to reveal the incidence and the reporting rates of incidental lesions encountered in cervical MRI examinations. To the best of our knowledge, this is one of the largest series in the literature focused on the incidental findings of cervical MRI.
Materials and methods
Patients
This research has been designed as a cross-sectional retrospective study and approved by the institutional ethics committee. The ethics committee has waived the informed consent from each patient due to the methodology of the study. The magnetic resonance (MR) images of all patients aged 18 years or older who have been admitted to our university hospital and undergone cervical MR imaging between January and April 2021 have been re-interpreted according to the incidental findings of the cervical MRI. Consecutively, 1019 patients were reviewed, and 18 of them were excluded due to the motion artifacts, which lowered the quality of the interpretation significantly. One MRI examination was excluded because of extensive susceptibility artifacts or image distortions due to multiple operation materials. Totally 1000 cervical MR images, each belonging to different patients (324 male, 676 females, mean age 47 ± 14), were enrolled in this investigation.
MR imaging
All images were obtained by a 1.5 tesla MR machine (Magnetom Aera, Siemens Healthcare, Erlangen, Germany) using a neck coil with 20 channels. The imaging protocol consisted of T1 weighted sagittal plane spin echo [TR: 663 ms, TE: 11 ms, Field of view (FOV): 240 mm, Slice thickness: 3 mm, Voxel size: 0.9 × 0.9 × 3 mm]; T2 weighted sagittal plane turbo spin echo (TR: 3800 ms, TE: 91 ms, FOV: 220 mm, Slice thickness: 3 mm, Voxel size: 0.7 × 0.7 × 3 mm) and T2 weighted axial plane turbo spin echo (TR: 780 ms, TE: 22 ms, FOV: 180 mm, Slice thickness: 3 mm, Voxel size: 0.4 × 0.4 × 3 mm) sequences. The axial plane images were not continuous, and they were focused on the intervertebral discs since this examination was performed to explain the intervertebral disc pathologies. Five axial plane slices of each cervical intervertebral disc were obtained.
Grouping the incidental findings
In this study, an incidental lesion is defined as a lesion in the field of view of a cervical MR image that is not located in the specific area of the cervical imaging to focus and is not related to the main purpose of the imaging. All extra vertebral areas of the neck and the skull base have been examined rather than a routine assessment of intervertebral discs, neural foramina, and spinal canal. Vertebral lesions were not accepted as incidental lesions since this area is included in the focus of a radiologist during a routine cervical MR examination. The extraspinal findings were classified into main groups regarding the regions as follows: nasopharyngeal, paranasal sinuses, thyroid gland, sella and hypophysis, posterior fossa, cervical lymphadenopathies, other soft tissue lesions, bony lesions outside the vertebras and other (unclassified) lesions.
Nasopharyngeal mucosal thickening, nasopharyngeal retention cyst, and Thornwaldt cyst were classified as nasopharyngeal lesions. Paranasal mucosal thickening and retention cysts were accepted as paranasal lesions. Thyroid nodules and enlargement of the thyroid gland were grouped in thyroid lesions. Lesions of the hypophysis, partial and total empty sella consisted of the lesions of sella and hypophysis. Cerebellar tonsillar herniations, mega cisterna magna, and arachnoid cysts (mega cisterna magna and arachnoid cysts were considered in the same group of lesions) consisted of the lesions of the posterior fossa.
Assessment of each lesion classification
All radiological interpretations were performed by two radiologists (with 4 and 17 years of experience) at the same time, using the same workstation of picture archiving and communications system (PACS).
Nasopharyngeal mucosa was measured on sagittal T2 weighted images, and more than a 3 mm thickness was accepted as a nasopharyngeal thickening by the criterion used in the literature before. 2 The cystic lesions with sharp margins and smooth contours were defined as a Tornwaldt cyst if the cystic lesion was in the midline and if the cyst had a direct attachment to the posterior wall of the nasopharynx. Cystic lesions located in other regions rather than the midline and have no direct attachment to the posterior nasopharyngeal wall is classified as retention cyst. 3 A thickness of more than 3 mm was accepted as a cut-off value to be a significant thickening for paranasal sinuses as described in the literature. 4 Dome-shaped cysts with homogeneous high signals in T2 weighted images with sharp demarcations and smooth spherical outlines along the free border of the cyst without bony destruction, and without any contact with the teeth roots were accepted as mucosal retention cysts. 5 The enlargement thyroid gland was accepted as an anteroposterior dimension of each lobe greater than 20 mm or isthmus thicker than 10 mm. 6 When more than half of the sella is filled with cerebrospinal fluid (CSF) and the thickness of the pituitary gland is less than 2 mm, this situation is classified as empty sella. Partial empty sella was considered if less than half of the sella is filled with CSF and the pituitary thickness is at least 3 mm. 7 A tonsillar herniation is considered if the descendent of the cerebellar tonsils below the foramen magnum is greater than 3 mm. 8 The enlargement of CSF-filled subarachnoid space of the inferior and posterior parts of the posterior cranial fossa refers to a normal variant called mega cisterna magna. Mega cisterna magna may be difficult to distinguish from an arachnoid cyst, which is a CSF-filled cyst and may be located in the same position as the mega cisterna magna. 9 A brain MRI may be helpful in differential diagnosis, but in this study, the aim was to indicate the possible lesions which are underestimated during the interpretation of the cervical MR imaging. Therefore, rather than focusing on the differential diagnosis between these lesions, they are classified as one lesion incidentally encountered during routine cervical MR examinations. Lymphadenopathy was considered if the short axis diameter was equal to or greater than 10 mm. If the lymph node was located in the lateral retropharyngeal region ≥5 mm, and any visible lymph node in the medial retropharyngeal group was also considered as lymphadenopathy. A cluster of three or more lymph nodes (each lymph node ≥8 mm) was also accepted as lymphadenopathy. Cystic or necrotic areas with high signals in T2 weighted images were also used to determine lymphadenopathy.10,11 Any cervical lymph node with a long-to-short axis ratio <2 was also considered lymphadenopathy as well. 12 Besides, indistinct or irregular nodal margins or infiltration into adjacent fat or muscle tissue indicating an extranodal extension was concluded as lymphadenopathy.
If more than one of the same lesion types was observed, only one lesion has been noted as an incidental finding. For example, if there were three thyroid nodules in a patient, it counted as one lesion type, thyroid nodule. When multiple lesion types were detected, all these classified lesions were counted in the worksheet.
Incidences and reporting rates
After the assessment of lesions and regional classifications, each lesion was noted for each cervical spinal MR examination. The incidences were calculated and presented with percentages from the collected data. In addition, the radiology reports were also re-examined regarding whether these incidental findings were mentioned or not. The reporting ratios of each lesion and region were also calculated and presented with percentages.
Results
The demographic properties of each incidental lesion classification.

Incidences and reporting rates of each incidental lesion in cervical MR examinations.


n: total number of patients with the related incidental lesion; INC: incidence; PCT: percentage (n/total of the patients with incidental lesions); REP: number of patients for which the related incidental finding was mentioned in the cervical MR report by the radiologist; NON-REP: number of patients for which the related incidental finding was not mentioned in the cervical MR report by the radiologist; PCT OF REP: reported/n ratio for each specific incidental finding; *: reported/n ratio for all of the incidental lesions.

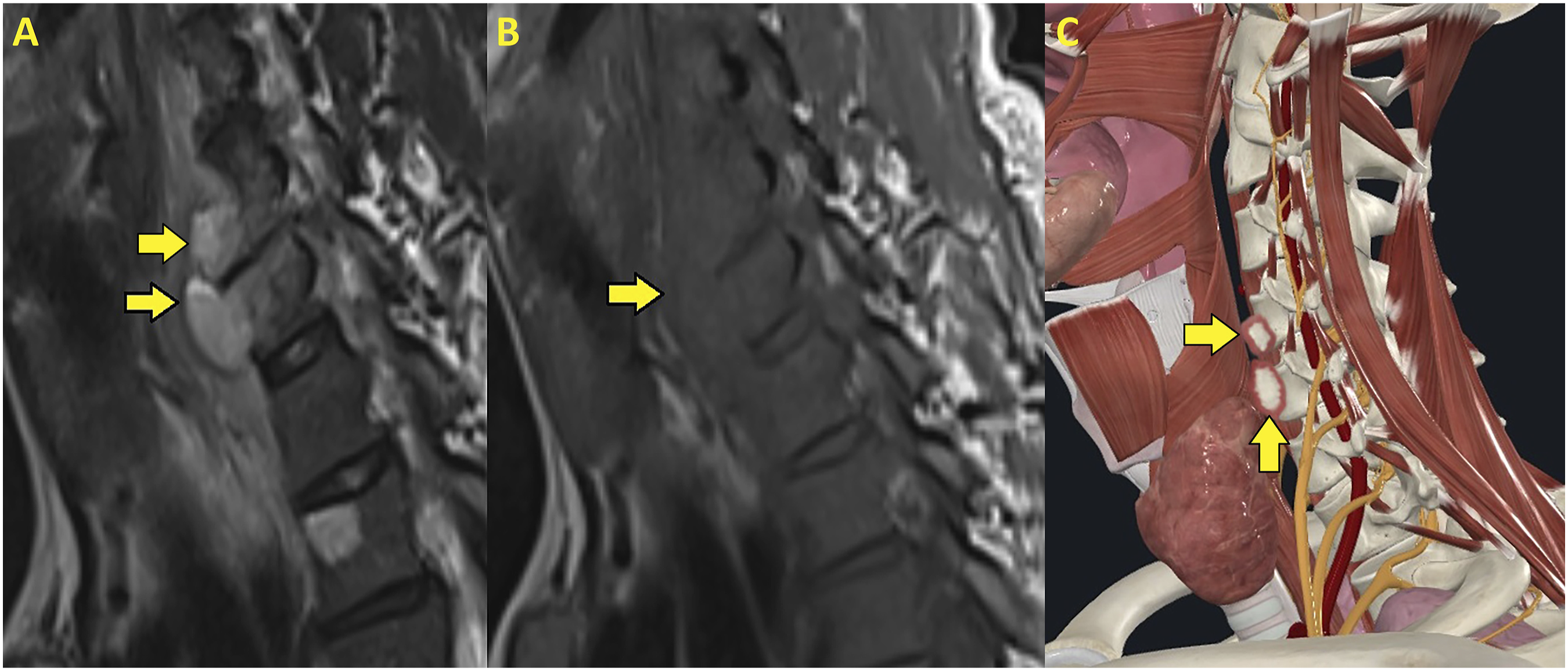
In sagittal plane T2 weighted (a) T1 weighted (b) and a 3D illustration (c) a thyroid nodule with a heterogenous structure is shown(yellow arrows).

The sagittal T2 weighted (a) T1 weighted (b), and 3D illustration (c) indicates a cystic lesion in the soft palate (yellow arrows).

A hypophysis adenoma is depicted by T2 weighted (a) T1 weighted (b) sagittal images, and a 3D illustration (c) which also indicates the location of the lesion (yellow arrows).
Multiloculated paravertebral abscess is shown by yellow arrows in T2 weighted (a) and T1 weighted (b) sagittal images. A 3D illustration (c) emphasizes the prevertebral location of the abscess formations (yellow arrows).

T2 weighted axial images indicate the cervical lymphadenopathies (a), (b), and a 3D illustration (c) of the lymphadenopathies indicates the cervical compartments of the lymph nodes (yellow arrows).

The protrusion of the suprasellar cistern into the sellar region with a hypophysis gland decreased in thickness indicates an empty sella in T2 weighted and T1 weighted sagittal images (yellow arrows).
Incidences and reporting rates of incidental lesion groups in cervical MR examinations.

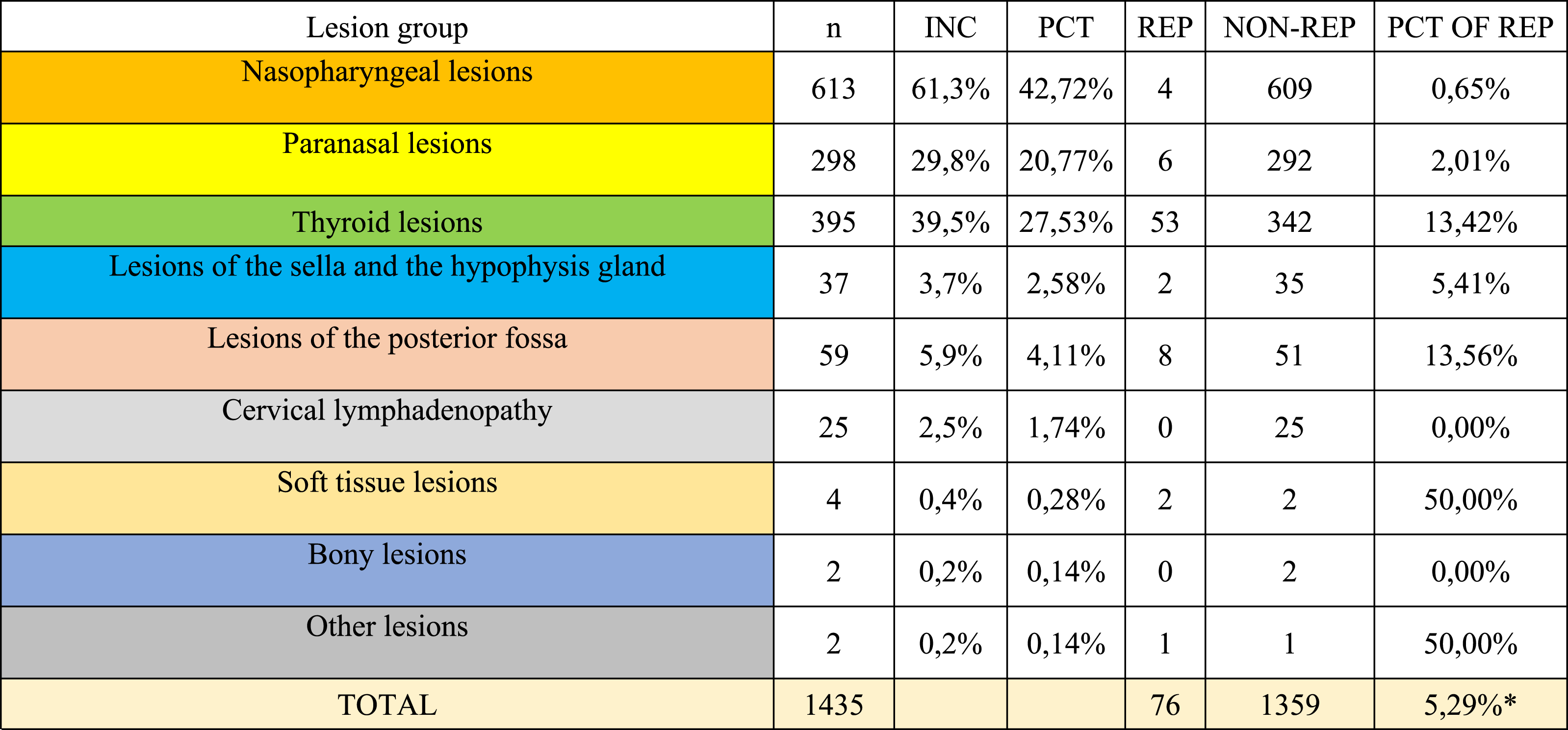
n: total number of patients with the related incidental lesion group; INC: incidence; PCT: percentage (n/total of the patients with incidental lesions); REP: number of patients for which the related incidental finding was mentioned in the cervical MR report by the radiologist; NON-REP: number of patients for which the related incidental finding was not mentioned in the cervical MR report by the radiologist; PCT OF REP: reported/n ratio for each specific incidental finding; *: reported/n ratio for all of the incidental lesions.

Distribution of the incidental lesion groups in this study population.
Reporting rates were also presented (Tables 2 and 3), and including all of the incidental findings, 5.29% of the lesions were mentioned in the radiology report of the cervical MRIs.
Discussion
Despite the low reporting rates in the daily radiology practice, this study emphasizes the high incidence and variability of the encountered incidental lesions in cervical MR imaging. The underestimation of these lesions may be a result of focusing on the main purpose of the imaging modality or as a consequence of using different reporting styles, which may be another topic to discuss with valid and objective data.
There are not many papers that studied incidental lesions of the cervical MR imaging, especially mentioning the reporting rates. The current study has one of the largest series specifically investigating the cervical region regarding incidental extraspinal lesions and reporting rates besides the incidences of these lesions. Even though the meticulous effort of the two observers together to detect the incidental lesions of the cervical MRI in such a large population, the result of the current study needs to be discussed and compared with other findings in the literature.
In Kamath et al.’s review, the authors indicated that meningioma, thyroid, salivary gland lesions, and nasopharyngeal tumors were the frequent incidental findings on cervical MR imaging reported in the past. 1 Another study in 2018 re-interpreted 1056 consecutive MR images in terms of the incidental findings and 192 of them were cervical MRIs. In this study, the authors reported that 29.16% of these examinations had incidental findings, and paranasal region lesions were the most encountered incidental finding, followed by thyroid lesions, besides total reporting rate was 29.5% for cervical MRIs in this study. 13 Zidan et al. specifically focused on the cervical spinal MRIs as in this current study, and 266 cervical MRIs were re-interpreted in their research. In their study, 16.9% of the patients had incidental lesions and thyroid nodules (6.3%), thyroid goiter (4.6%), and mucosal thickening in paranasal sinuses (2.68) which were the most encountered incidental findings, respectively. This study also investigated the distribution of incidental findings regarding age groups. Patients 41–60 years old were the age group the incidental lesions mostly encountered in their study. 14 300 cervical MR images were re-evaluated, and 13.7% of the cervical MRIs had incidental findings in the study of Kaya et al. Thyroid nodule was the most common amongst other incidental lesions in their research. 15 Another study indicated that mucosal thickening and retention cysts of the paranasal sinuses were the most encountered incidental lesions (34.42% and 22.95% of all incidental lesions respectfully) during the interpretation of cervical MR images. 16 The number of cervical MRIs evaluated in this current research was larger (n = 1000) and two reviewers detected the incidental lesions together. In this current study, 72.6% of the patients had at least one incidental finding, and nasopharyngeal and thyroid regions were the most common sites of these lesions. Surprisingly a very low reporting rate was noted (5.29%) in our research.
There were more lesion types scanned as a part of this study. Nasopharyngeal, oropharyngeal and hypopharyngeal neoplasms, thyroglossal cysts, laryngeal lesions, cerebral or cerebellar neoplasms, vascular aneurysms of carotid arteries, esophageal lesions, lesions of the parotid and submandibular gland were also scanned, however, these lesions were not encountered in our study population.
Wagner et al.’s study investigated the effect of the picture archiving and communication system (PACS) on reporting the incidental findings of the lumbar spinal imaging. They showed that the number of incidental lesions reported increased significantly by 163% after the implementation of PACS, moreover, along with the increased number of incidental findings, the recommended follow-up studies increased by 540%. 16
The technical parameters of the imaging sequences were 0.9 × 0.9 × 3 mm voxel size for T1 weighted sagittal plane, 0.7 × 0.7 × 3 mm voxel size for T2 weighted sagittal plane, and 0.4 × 0.4 × 3 mm voxel size for T2 weighted axial plane (3 mm slice thickness for all these sequences) regarding the dimensions of the voxels used in this current study. Besides, FOVs were 240 mm, 220 mm, and 180 mm regarding the above MR sequences, respectively. These technical parameters may play a role in indicating the incidental findings. The slice thickness might influence the characterization of the lesion; in addition, as the FOV increases, the scanned area would be more extensive and may increase the possibility of finding an incidental lesion. This current study is not focused on comparing different technical parameters and their outcomes; however, research that reveals the relationship between each of these technical parameters and the number of reported incidental lesions would make a significant contribution to the literature.
The detection of incidental lesions has multiple aspects to discuss in terms of challenges for clinicians, radiologists, patients, and health economists. The developments of the detection and evaluation techniques make more lesions available to reveal, in addition, cost-effectiveness analyses also have a central place in addressing the problem of incidental lesions. 17 The medicolegal aspects of the incidental lesions were out of the scope of this research; however, incidental lesions are of great importance to the radiologist. The diagnostic error is often the basis of lawsuits against radiologists, and the possible causes of perception errors are reported in the literature resulting in the failure to detect an abnormality on a radiological examination.18,19
There are limitations of this study which should be considered carefully to interpret the outcome of the research. First, the larger the FOV, the more data is obtained. Different centers may use variable FOV choices in their routine MR applications, and crosschecking the results of this research with other studies in the literature may not reflect a true comparison. Secondly, the detection of incidental lesions was based on radiological findings instead of surgical or histopathological confirmations in this study. Some of the outcomes of the lesions cannot be reached because of the nature of the lesion, and follow-ups may be required instead of biopsy or surgery. Moreover, some of the results might not be noted in the patient records due to the patient’s lack of follow-up admittance. Another important limitation was the lack of follow-up to determine how many of these incidental findings led to clinically significant pathology. Addressing this shortfall would have significantly added to this paper’s contribution to the literature. And last, to find out more accurate numbers of incidences and reporting rates, studying larger populations or the contribution of more studies to the data pool of the literature is required.
In conclusion, incidental findings are commonly encountered; however, rarely reported during cervical MRI examinations. Radiologists should be aware of the extraspinal findings and the most common areas to detect incidental lesions. A careful MR interpretation is crucial to detect these lesions in the extraspinal region in cervical MRIs, which might be very important for the patients and to avoid medicolegal consequences.
Footnotes
Acknowledgements
All illustrations in this article have been created using the Adobe Photoshop program (Adobe Inc., 2021. Adobe Photoshop, https://www.adobe.com/products/photoshop.html) and based on the figures provided by the Complete Anatomy program (3D 4 Medical., 2021. Complete Anatomy. Retrieved from ![]() ).
).
Author Contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available due to the risk of breach of patient data privacy but are available from the corresponding author on reasonable request.