
Abstract
Background
Spinopelvic balance measurement is a key point to get an appropriate diagnosis and treatment in a group of spine pathologies; thus, it seems necessary the evaluation of different methods for obtaining the most reliable values. For that reason, different automatic and semi-automatic computer-assisted tools have been developed, and one example of them is Surgimap.
Purpose
To demonstrate that the sagittal balance measurements with Surgimap are equal and more time-efficient than with Agfa-Enterprise.
Material and Methods
Retrospective-prospective study. Biased comparative analysis of radiographic measurements performed on two different occasions (96 h interval), between two spine surgeons using Surgimap and two radiologists using the traditional Cobb method (TCM) with the Agfa-Enterprise program in 36 full spine lateral X-ray, determining inter- and intra-observer reliability and the mean time required to obtain the measurements.
Results
Measurements with both methods demonstrated an excellent intra-observer correlation (Surgimap: PCC 0.95 [0.85–0.99]; TCM: PCC 0.90 [0.81–0.99]). Inter-observer correlation also demonstrated an excellent relationship (PCC >0.95). Thoracic kyphosis (TK) demonstrated the lowest levels of inter-observer correlation (PCC: 0.75). The average time in seconds with TCM was 154.6, while with the Surgimap it was 41.8 s.
Conclusion
Surgimap proved to be equally reliable and 3.5 times faster. Therefore, in consistency with the available literature, our results would allow us to promote the use of Surgimap as a clinical diagnostic tool considering precision and efficiency.
Introduction
Sagittal balance represents the basic mechanism to maintain an upright posture with a low energy requirement.1,26 Faced with the loss of this, the body uses compensatory mechanisms, at the expense of muscle contracture with a higher energy cost, to maintain an adequate posture, which has a negative impact on the quality of life of the patient,2–5 which even has an impact like pathologies such as chronic lung disease, visual disturbances, osteoarthritis, rheumatoid arthritis, and others. 2 For this reason, the analysis of the sagittal balance, through the assessment of radiographic measurements and parameters, is essential in the evaluation and treatment of an individual with spinal deformity.2,3
Even in the most experienced hands, this analysis can be an arduous practice that will have its difficulties, due to either poor visualization of anatomical landmarks or manual measurement errors.6,7
Although the TCM is still the most important and used technique for the evaluation of the sagittal balance,8–12 to correct these difficulties, as well as to perform measurements in a faster and more practical way, various automated and semi-automated computer-aided tools, such as Surgimap (Nemaris Inc., New York, NY), have been developed.
Despite the growing number of research supporting the use of these tools, there is a need for new studies to support their use and practicality, as many spine surgeons admit not to use them regularly.13,14 The objective of the present work is to evaluate the usefulness of this tool, determining the intra- and inter-observer reliability, and establishing the potential advantages compared to the TCM.
Material and methods
Thirty-six full spine lateral x-rays from the database of our institution were randomly analyzed. Those that belonged to 18-year-old individuals or older with adequate radiographic technique (inclusion of femoral heads up to auricle) were included. In contrast, all those with poor visualization of anatomical landmarks or with the presence of deformity in the sagittal plane secondary to tumor, infectious, and/or post-traumatic causes were excluded.
The sample size was determined by statistical power software (G-Power), using defined precision (Power 0.85; statistical significance p < .05).
Two experienced spine surgeons, using the semi-automatic program (Surgimap), and two radiologists, using the TCM with the Agfa-Enterprise program, separately measured different radiographic parameters (cervical lordosis [CL], pelvic incidence [PI], sacral slope [SS], pelvic tilt [PT], mismatch [PI-LL], lumbar lordosis [LL], and thoracic kyphosis [TK]) in all radiographs that met the inclusion criteria. Measurements were carried out in a biased way between the evaluators, doing the same process two times separated by a timeframe of 96 h each; the evaluators were blind to their own measurements at the time of taking the second round.
A statistical analysis was performed through intraclass correlation coefficient (ICC), a widely used reliability index. We used it for the evaluation of intra-rater and inter-rater reliability analyses through Pearson correlation coefficient (PCC) with a 95% confidence range. We take as a model Dang et al. 7 to interpret the measurements as poor (PCC <0.40), adequate (PCC 0.40 0.59), good (PCC 0.60 0.74), or excellent (PCC >0.75). 15
Additionally, the time to get the measurements in each case was recorded and registered in seconds. This time variable was analyzed making a simple math comparison between average time obtained by both methods.
Results
Intra-observer correlation between measurements obtained by spine surgeons and radiologists.
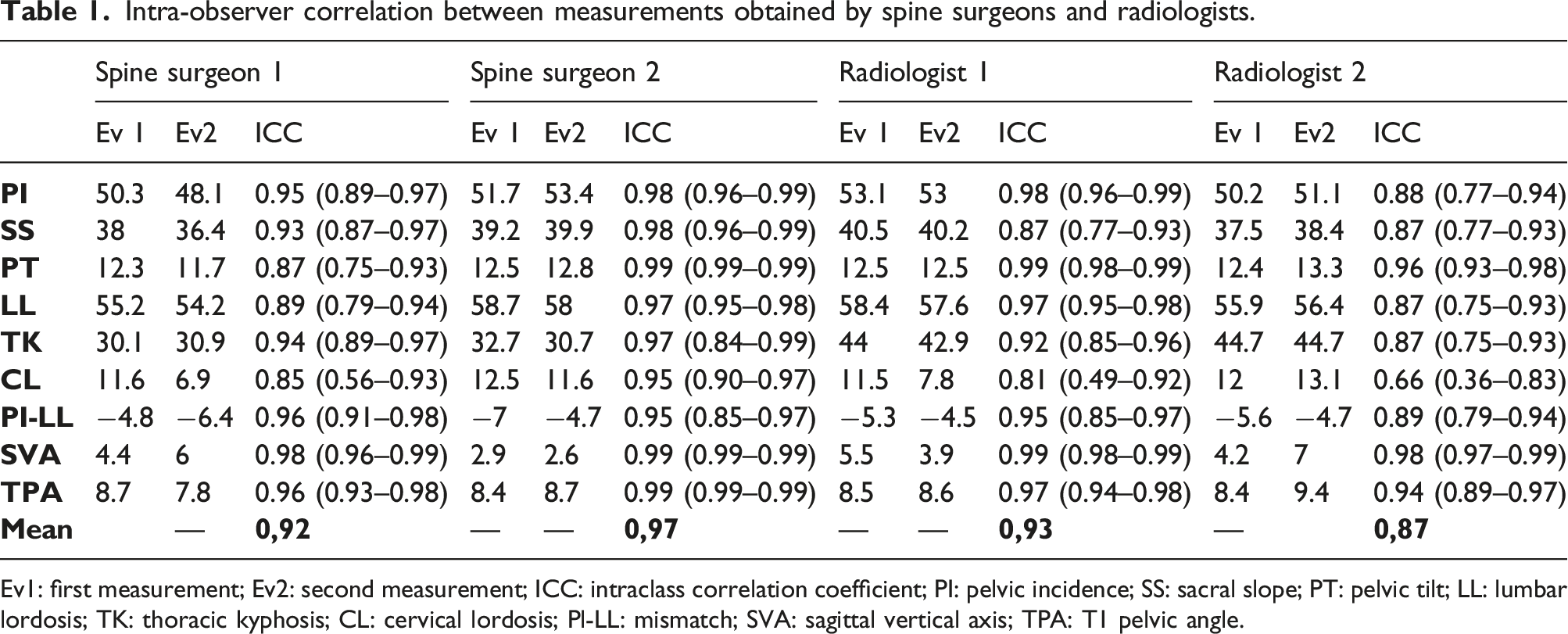
Ev1: first measurement; Ev2: second measurement; ICC: intraclass correlation coefficient; PI: pelvic incidence; SS: sacral slope; PT: pelvic tilt; LL: lumbar lordosis; TK: thoracic kyphosis; CL: cervical lordosis; Pl-LL: mismatch; SVA: sagittal vertical axis; TPA: T1 pelvic angle.
Inter-observer correlation between measurements obtained by spine surgeons and radiologists.

SS1: spine surgeon 1; SS2: spine surgeon 2; R1: radiologist 1; R2: radiologist 2; ICC: intraclass correlation coefficient; PI: pelvic incidence; SS: sacral slope; PT: pelvic tilt; LL: lumbar lordosis; TK: thoracic kyphosis; CL: cervical lordosis; PI-LL: mismatch; SVA: sagittal vertical axis; TPA: T1 pelvic angle.
Regarding the recorded time to obtain the measurements, the mean time was 154.6 s per X-ray with the TCM, while with the semi-automatic program it was 41.8 s, thus, showing a speed in performing these measurements 3.5 times greater in the case of spine surgeons (Figure 1). Mean time (seconds) required to obtain the measurements.
Discussion
Poor radiographic technique and poor visualization of anatomical landmarks can make it difficult to obtain radiographic measurements in the sagittal profile and it is even more complex in the presence of different pathologies such as infection, scoliosis, deformities, obesity, osteoporosis, or high-grade spondylolisthesis,6,24,25 making the assessment of the sagittal balance a challenge.
The advent of digital X-rays, which made it possible to adjust the contrast, invert the colors, and modify the sharpness, has been able to overcome, in part, this problem by allowing better visualization and identification of the reference points, thus reducing the measurement error, and showing an excellent intra- and inter-observer reliability when compared with measurements made on traditional radiographic templates.16,17
Together with the digital X-ray era, multiple computerized programs have been developed, such as automatic and semi-automatic tools, which have also showed a good correlation with less time required to obtain these radiographic measurements.18–22
Despite technological advances, the correct identification of anatomical landmarks continues to be a limitation and the main generator of variability between different methods and observers, specifically, in the thoracic area where the overlapping of the shoulders makes it difficult to see the upper region of this segment, hindering the assessment of TK, 6 which is reflected in our work on the lower levels of PCC obtained. At the cervical level, the CL also showed low PCC values, which could be explained by the curved shape of the lower endplate of C2, where the user must use an approximate straight line, leading to confusion and measurement error. 14
According to the results obtained in this study and those mentioned in the literature, computer-assisted methods do not improve the precision of the measurements, but rather the time in obtaining them, this being the main advantage shown.18–22
In our study, the average time required to obtain all the variables assessed was 41.8 s with the semi-automatic program compared to 154.6 s with the TCM, the former resulting 3.5 times faster, in consistency with other studies that indicated an average time of 75 s compared to 3–15 min for TCM. 14
The greatest speed in obtaining these measurements, specifically with the Surgimap, is explained by its semi-automatic nature, which yields multiple measurements through only the sequential identification of a limited number of anatomical points (femoral heads, upper endplate of S1, L1, and T1, and lower endplate of C2), compared to TCM, 17 which requires the identification of these points for each measurement to be performed, implying a longer time with a greater operator-dependent requirement and, therefore, representing a greater risk of human error.
One of the main negative aspects of the spine measurement software is its lack of practicality, and it is often cumbersome due to the difficult interfaces that require extensive knowledge or handling of it. In the case of the Surgimap, it offers a user-friendly interface with instructions and graphical representations of each tool, making it a simple-to-use program that allows performing osteotomy simulations and surgical planning, in addition to obtaining the assessment of the sagittal profile in a fast and reliable manner, without requiring a considerable level of expertise on the part of the user, which has not proven to be a factor that influences the reliability of this method either. 23
The main limitation of the present study was because all the X-rays belonged to healthy patients; therefore, they did not present deformities or structural alterations of the spine, which may represent a bias in our results. However, other studies with similar characteristics where pathological spines were evaluated showed that these conditions did not seem to modify the reliability of the method.27–30 In addition, there may be a built-in bias toward more reproducible results on the part of the operators, who were familiar with the two types of tools used. Despite this, Segev et al. 23 could not demonstrate that the evaluator’s experience had a significant implication in carrying out measurements of different radiographic parameters.
In conclusion, the results shown in our study, in consistency with the available literature, support the reliability and usefulness of semi-automatic programs, specifically the Surgimap, by demonstrating an excellent inter- and intra-observer correlation with significantly shorter times (3.5 times faster) to obtain different measurements and radiographic parameters that are necessary for the assessment of the patient’s sagittal profile, in comparison with the TCM, further adding the ability of this tool to carry out pre-surgical planning and post-surgical simulations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.