
Abstract
Bronchial artery embolization is minimally invasive, has a low complication rate, and achieves good hemorrhage control. It is the first-line treatment in hemoptysis patients whom medications are ineffective. Cerebral infarction is a rare complication of bronchial artery embolization, with posterior circulation infarcts being the most common. Possible mechanisms include a neurotoxic reaction to the contrast medium used, bronchial artery-pulmonary shunt, embolus formation, fistula formation between the bronchial artery and the cerebral artery, and so on. To the best of our knowledge, there have been relatively few reports regarding posterior circulation infarcts after BAE, including 14 cases shown in Table 1. 11 patients recovered well after medical treatment, while the other patients did not survive. We report a case of a patient with a large posterior circulation infarct post bronchial artery embolization who developed severe neurological symptoms and died after 3 months of medication. Conclusion: Posterior circulation infarction is a rare but severe complication of bronchial artery embolization, and measures should be taken to prevent its occurrence.
Case of posterior circulation infarction after bronchial artery embolization.

Case report
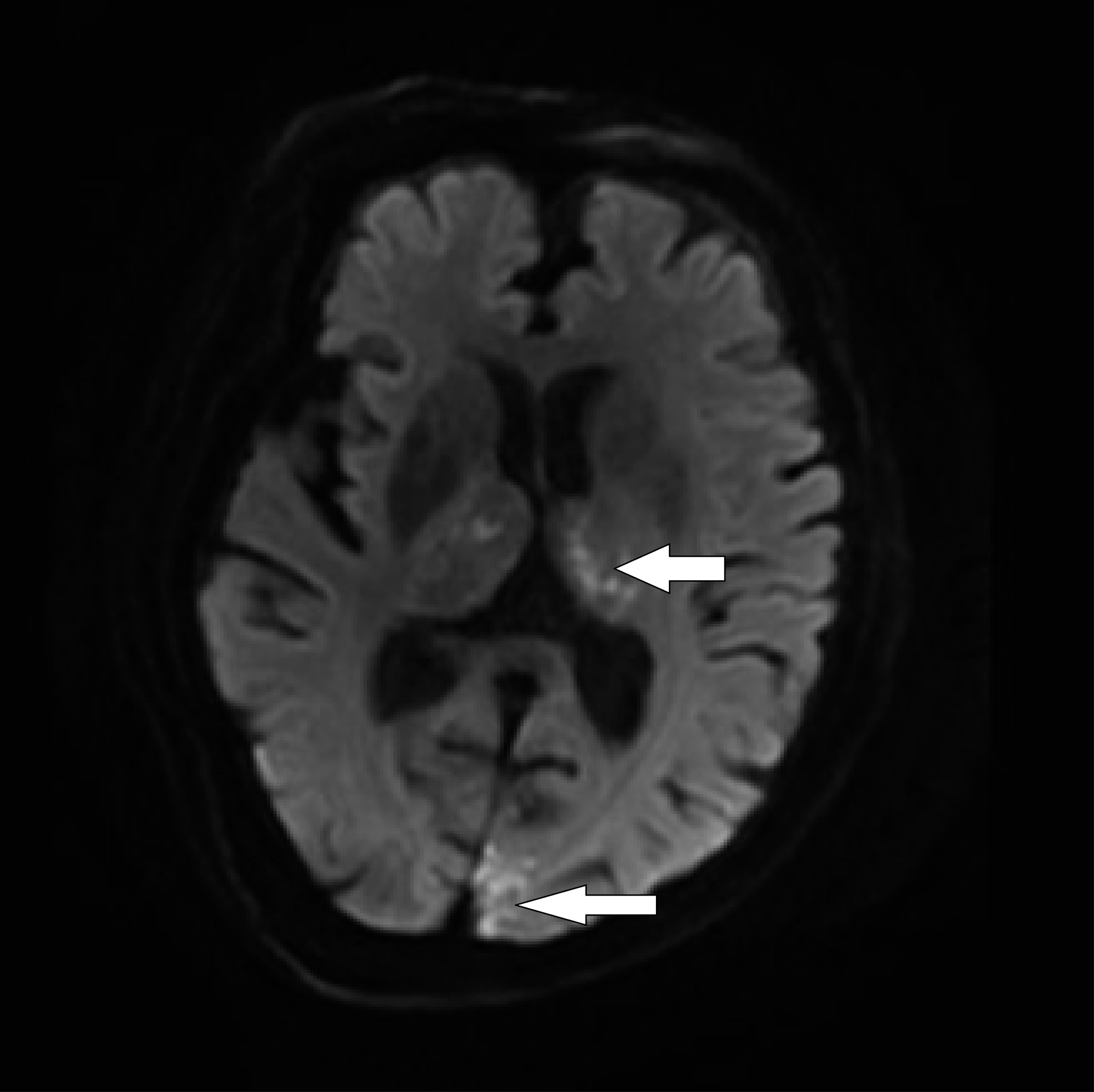
An 86-year-old female patient was admitted to the respiratory ward 1 day after she was found to have a lung mass following a history of cough for 2 months and hemoptysis for 1 week (160 mL of blood daily). She reported chest tightness, dyspnea, fever, and cold tolerance, underwent chest computed tomography (CT) in the emergency department, and it showed a mass in the left upper lobe of the lung. She was prescribed antibiotics, mucolytics, bronchodilators, and coagulants, which resulted in a decrease to 110–130 mL of the daily hemoptysis amount. 2 days later, a chest contrast CT was performed and it showed a space-occupying lesion in the patient’s left upper lobe of the lung (Figure 1). Nine days later, the patient underwent bronchial artery embolization with regional anesthesia. During the procedure, the right femoral artery was punctured by the Seldinger puncture technique, a 5-F catheter sheath (Terumo, Japan) was introduced, and a 4-F Cobra catheter (Cordis, USA) was followed by a 0.035-inch guide wire (Terumo, Japan). The 4-F Cobra catheter that was passed through the bronchial artery revealed asymmetrical contrast uptake in the left upper lobe of the lung (Figure 2). The left bronchial artery originates from the thoracic aorta, supplies blood to the left lung, and can be seen due to its curvature and thickness. The 2.7-F microcatheter (Terumo, Japan) was inserted in the middle of the left bronchial artery for contrast injection to identify the target vessel. The microcatheter was then used to inject 100–300 μm Embospheres (Merit, USA), using one vial to embolize the left bronchial artery. After embolization, contrast was injected via a 4-F Cobra catheter to assess the degree of bleeding from the left bronchial artery. Embolization of the arterial supply to the left lung mass was then confirmed. At this stage, the patient was hypersomnolent, apathetic, and then unresponsive. Her blood pressure was 140/95 mmHg, heart rate was 60 bpm, and respiratory rate was 20/min. An emergency head CT showed no infarct. Cerebral CT angiography (CTA) showed cerebral arteriosclerosis and multiple areas with mild stenosis of the posterior circulation. After the brain CT, the patient became delirious and her pupils became asymmetrical. Her left pupil had a diameter of 1.5 mm while the right one had a diameter of 1.0 mm. Her pupillary reflexes were delayed bilaterally, and she could not protrude her tongue on prompting during the examination. Emergency brain diffusion-weighted magnetic resonance imaging (DW-MRI) showed acute infarcts in both cerebellar hemispheres, the brainstem, thalamus, and left parieto-occipital lobe (Figures 3 and 4). The patient was subsequently transferred to the neurology intensive care unit and administered vasodilators, antibiotics, and mucolytics. There was no hemoptysis after bronchial artery embolization; it was considered to be effective. 4 days later, a repeat DW-MRI series showed a greater infarct area in the cerebellar hemispheres, brainstem, thalamus, and left parieto-occipital lobe, with the left hemisphere having no significant change. The patient died after 3 months of treatment. A lesion in left upper lobe of the lung (arrow). A proximal branch of left bronchial artery (arrow) communicated with left subclavian artery. MRI DWI image showed acute infarcts in both cerebellar hemispheres, brainstem, thalamus, left parieto-occipital lobe (arrow). MRI DWI image showed acute infarcts in both cerebellar hemispheres, brainstem, thalamus, left parieto-occipital lobe (arrow).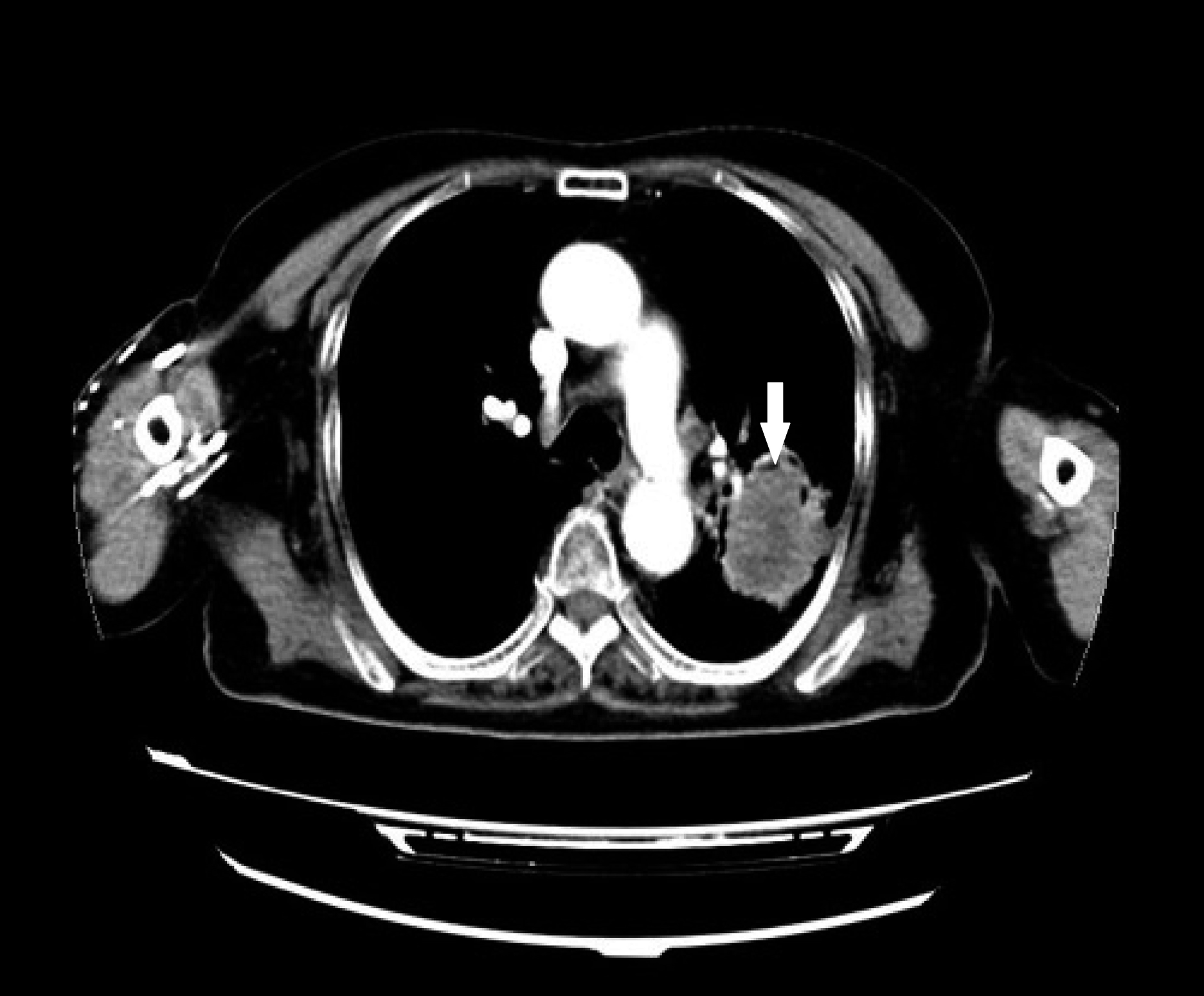


Discussion
Previous case reports document the causes for cerebral infarction after bronchial artery embolization as contrast-induced, 7 bronchial artery-pulmonary shunt, retrograde flow of embolic agent, and bronchial artery communicating branch formation. Contrast-induced encephalopathy is most likely due to the presence of iodine in the contrast, which changes the intracranial pressure and alters nerve cells and their function due to its osmotic pressure difference with cerebrospinal fluid. This is transient and reversible. A bronchial artery-pulmonary shunt is an abnormal connection between the bronchial artery and the pulmonary circulation arising from lung diseases. The embolic agent enters the pulmonary circulation from the bronchial artery through the abnormal shunt and then enters the systemic circulation. 8 Retrograde flow of the embolic agent occurs when the catheter inside the bronchial artery leaks out the embolic agent; this is commonly seen in embolization of the subclavian artery and its branches. 9 The presence of a communicating branch from the bronchial artery is a blood vessel congenital malformation. It includes communication between the bronchial artery and the coronary artery, vertebral artery, and internal carotid artery. During the embolization of the bronchial artery, the embolic agent enters the cerebral blood vessels or other arteries through the communicating branch, 10 resulting in the embolization of cerebral blood vessels and other blood vessels.
The patient in this case had a chest contrast CT performed 7 days before the procedure, and she had no neurological symptoms. Furthermore, before bronchial artery embolization, contrast imaging with iodine was performed without the patient exhibiting neurological symptoms. As such, contrast-induced encephalopathy is unlikely to have been the cause of her cerebral infarct. There was no shunting identified in the patient’s left bronchial artery on arteriography imaging; hence, the possibility of a bronchial artery-pulmonary shunt was low. The bronchial artery embolization procedure was performed under digital subtraction angiography using 2.7-F microcatheter super-selective left bronchial artery embolization. Therefore, dislodgement of the embolic agent as a cause of cerebral infarct in this patient can be excluded. The possibility of a communicating branch between the left bronchial artery and the subclavian artery was considered in this case. During the operation, a 100–300-μm Embosphere microembolus entered the left subclavian artery through the abnormal communication; it then entered the left vertebral artery, occluding the posterior circulation. This was not documented in the prior medical literature.
The 2022 practice guidelines for bronchial artery embolization of the European Society of Cardiovascular and Interventional Radiology recommend the use of non-spherical polyvinyl alcohol (PVA) particles with a diameter of 300–500 μm, and calibrated spherical microspheres larger than 300 μm can also be considered as a substitute for PVA particles. In this case, microspheres and PVA particles were selected as embolic materials. The main reason was the embolization of the trunk of blood vessels caused by the swelling of PVA particles, which could easily lead to the establishment of collateral circulation and tumor recurrence. Embosphere microspheres are spherical and compressible. After being injected into blood vessels, the spheres are compressed and flow more easily to the branches of the embolized blood vessels and to the small blood vessels of the tumor. It is also reported that the diameter of the anastomotic branch of the bronchiolar artery is approximately 72–325 μm. If the diameter of the embolic agent is less than 325 μm, the particles may enter the pulmonary artery through the anastomotic branch and cause non-target vascular embolism. 11 In this case, the size of the Embosphere microspheres was 100–300 μm rather than 300–500 μm. The main reason was that the 100–300 μm microspheres embolized the branches of the left bronchial artery and tumor target vessels more thoroughly than the 300–500μm microspheres. Because there are potentially abnormal communicating branches of the bronchial artery and the left subclavian artery in this patient, the choice of a 100–300μm or 300–500μm particle size, PVA particles or microspheres may cause ectopic embolism. Which size and type of embolic agent is safer and how to avoid such complications is a key point for future research. We believe that preoperative detailed bronchial artery CTA examination, comprehensive evaluation of bronchial artery angiography images, superselective embolization with a microcatheter, injection of the embolic agent under full fluoroscopy, embolic agent diameter greater than 300 μm, and paying attention to the changes in vital symptoms and signs during embolization are key to avoiding ectopic embolism and even cerebral infarction.
In conclusion, posterior circulation infarction is a rare but severe complication of bronchial artery embolization, and measures should be taken to prevent its occurrence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.