
Abstract
Background
Dorsal/volar tilt is an important radiographic measurement commonly included in the treatment decision of distal radius fractures (DRFs). However, studies have shown that forearm positioning relative to rotation (i.e., supination and pronation) can affect the measured tilt value but with substantial interobserver variance.
Purpose
To examine whether interobserver agreement on radiographic tilt measurement is influenced by forearm rotation.
Material and Methods
We radiographed 21 cadaveric forearms at 5° rotational intervals between 15° supination and 15° pronation on lateral radiographs. A radiologist and a hand surgeon measured tilt in a blinded and randomized fashion. Bland–Altman analyses with bias and limits of agreement (LoA) were used to estimate interobserver agreement for forearms in all degrees of rotation, non-rotated forearms, supinated forearms, and pronated forearms.
Results
Interobserver agreement varied with forearm rotation. Bias (95% confidence interval [CI]; LoA) was −1.54° (95% CI: −2.53, −0.55; LoA: −13.46, 10.38) when measuring tilt on radiographs with all degrees of forearm rotation, and −1.48° (95% CI: −4.13, 1.17; LoA: −12.88, 9.92) when measuring tilt on true lateral 0° radiographs. When measuring on supinated and pronated radiographs, bias was −0.03° (95% CI: −1.35, 1.29; LoA: −8.34, 8.28) and −3.23° (95% CI: −5.41, −1.06; LoA: −16.90, 10.44), respectively.
Conclusion
Interobserver agreement on tilt was similar when comparing measurements made on true lateral radiographs to those made on the group with all degrees of forearm rotation. However, interobserver agreement improved with supination and worsened with pronation.
Introduction
Distal radius fractures (DRFs) account for approximately 20% of fractures in adults, making them one of the most frequent fracture types. 1 A common DRF subtype is the dorsally angulated DRF with distal fragment impaction with or without ulnar styloid fracture. 2 Long-term DRF effects can be pain, joint instability, loss of strength, limited range of motion (ROM), and osteoarthritis, which can have different lifelong consequences depending on the patient’s age. 3 Long-term DRF effects can potentially affect the patient’s future job opportunities, which can have a major socioeconomic impact. For geriatric patients, long-term DRF effects can influence their quality of life by decreasing functional independence. 1 Therefore, correct diagnosis and DRF treatment decision-making are important.
DRFs are traditionally diagnosed using radiographic imaging, and the decision of conservative versus operative treatment is based partly on radiographic measurements.4–6 An important radiographic measurement in many clinical practice guidelines (CPG) is the degree of angulation of the distal articular surface of the radius, defined as volar or dorsal tilt depending on its direction.4–6 The Danish CPG recommends a threshold value of >10° dorsal tilt relative to the long axis of the radius to determine when operative treatment should be considered. 4 The treatment aims to restore an anatomically correct angulation of approximately 12° volar tilt, which has been correlated with better patient-reported outcomes and ROM.3,7,8 Hence, dorsal tilt is used to quantify fracture displacement, while volar tilt is used to assess fracture reduction or surgical outcome regarding fracture displacement. Therefore, it is important to test the quality of the measurement method in fractured forearms and in anatomically correct forearms.
Given the importance of volar tilt measurement in treatment and prognosis, it is concerning that several studies have found interobserver variance when experienced physicians measure tilt.9–12 Furthermore, studies show that the measured value of tilt is influenced by forearm rotation since supination and pronation, respectively, increase and decrease the measured value of volar tilt.11,13–17 This observation emphasizes the importance of a true lateral radiograph in diagnosing and treating DRFs. However, the effect of forearm rotation on interobserver agreement on the radiographic measurement of dorsal/volar tilt has, to the best of our knowledge, not been explored.
This study examines whether interobserver agreement on tilt is influenced by forearm rotation. Its objectives were to estimate interobserver agreement on volar tilt when measured on (a) forearms in various degrees of rotation, (b) neutral rotation (i.e., true lateral radiographs), (c) supinated forearms, and (d) pronated forearms.
Material and Methods
Data collection
This study used 11 right and 10 left cadaveric forearms severed mid-humerus. After inclusion based on bone maturity and exclusion based on congenital abnormalities and fracture sequelae, no arms were excluded. The arms all came from anonymous individuals who donated their bodies to science. The Regional Ethics Committee approved the study according to the Danish Law of Health §14 (Project-ID: S-20,180,077).
The material used in this study was collected for a previous study. Radiographs were obtained with a focus-to-detector distance of 100 cm and the central ray directed at the radio-carpal joint with no tube angulation. The method of obtaining the radiographs is further described in Jensen et al.
14
A custom-made platform was used to stabilize the forearms. A Kirchner wire in the proximal radius and a goniometer attached to the platform were used to induce forearm rotations of approximately 15° to either side in steps of 5°. The 0° rotation was defined as a true lateral radiograph determined by the pisoscaphocapitate relationship.
18
Supination is indicated by negative values and pronation by positive values. This protocol provided seven radiographs per specimen with −15°, −10°, −5°, 0°, 5°, 10°, and 15° degrees of rotation, resulting in 147 total radiographs. Two observers, a hand surgeon with 25 years of experience, and a musculoskeletal radiologist with 19 years of experience, were introduced to the same method of measuring volar tilt, which was described in Kreder et al., Figure 1.
2
Blinded to the degree of rotation, the observers independently measured tilt on the 147 radiographs. Method for measuring tilt. Key: A, a line through the longitudinal axis of the radius; B, a line perpendicular to line A; C, a line along the distal articular surface of the radius. Tilt was measured as the angulation between lines B and C.
Statistical analyses
The distribution of all data groups was tested for normality. The agreement between the two observers was illustrated using Bland–Altman (BA) plots with limits of agreement (LoA). The LoA were estimated to contain 95% of all observed differences between the two observers. Therefore, they were used to estimate the realistic range of differences between observers. The average difference between observers was described as bias, which represented the possible tendency of one observer to systematically measure higher or lower than the other.19,20 The following four BA-plots were created: (a) one containing all radiographs (n = 147), (b) one containing the true lateral radiographs (n = 21), (c) one containing the radiographs of forearms supinated between −10° and −15° (n = 42), and (d) one containing the radiographs of forearms pronated between 10° and 15° (n = 42). All statistical analyses were performed using Stata v.17 (StataCorp 2021, TX).
Results
We found a minor difference in interobserver agreement between the group containing all degrees of rotation and the group containing only true lateral radiographs. LoA was ±11.9° for all radiographs compared to ±11.4° for true lateral radiographs. There was no clinically relevant difference in bias between the two groups, which was −1.54° for all radiographs and −1.48° for true lateral radiographs.
Interobserver agreement on volar tilt for different rotations, quantified by Bland–Altmann limits of agreement and bias.
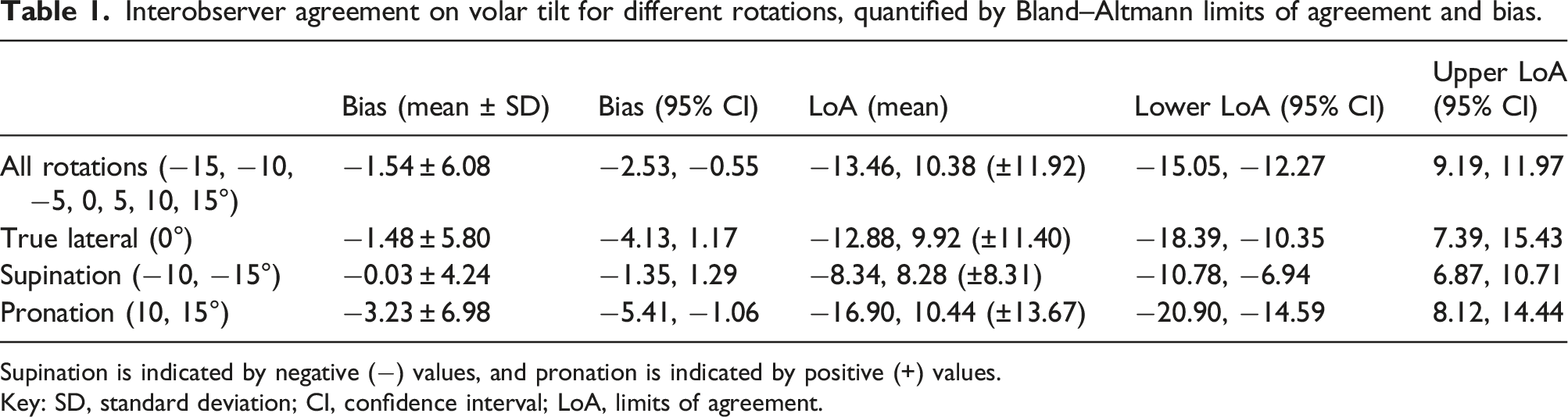
Supination is indicated by negative (−) values, and pronation is indicated by positive (+) values.
Key: SD, standard deviation; CI, confidence interval; LoA, limits of agreement.

Bland–Altman plots showing interobserver agreement for different forearm rotation groups. (a) Radiographs with forearm rotations of 15° supination to 15° pronation (n = 147). (b) Radiographs of true lateral forearms according to pisoscaphocapitate relationship (n = 21). (c) Radiographs with forearm supination of 10°–15° (n = 42). (d) Radiographs with forearm pronation of 10°–15° (n = 42). The mean measured difference between the two observers is indicated by the dotted line, with a 95% confidence interval (CI) indicated by the green box. The limits of agreement are estimated to contain 95% of all observed differences between observers and are indicated by solid lines, with 95% CIs indicated by the blue boxes.
Discussion
This experimental study used 21 cadaveric arms to examine the influence of forearm positioning (i.e., rotation) during acquisition of wrist radiographs on interobserver agreement in tilt measurement. No clinically relevant difference was found in interobserver agreement between the group containing all the radiographs and the group containing only true lateral radiographs. Notably, we found that supination improved interobserver agreement compared to pronation, which worsened interobserver agreement. Interestingly, supination improved the interobserver agreement more than true lateral positioning.
Jensen et al. 13 found that forearm rotation significantly impacted interobserver agreement on dorsal tilt in cadaveric arms with surgically manufactured DRFs. Using a BA analysis, they compared agreement between various degrees of supination and pronation combined with neutrally rotated (0°) forearms, finding that bias (BA LoA) improved from −1.41 (±7.68°) to 0.12 (±3.94°). Christersson et al. 9 also used a BA analysis to examine interobserver agreement on dorsal tilt in 33 patients with DRFs. However, they only examined non-rotated forearms and found a bias (BA LoA) of 0.2 (±4.6°). Therefore, they did not add directly to the knowledge about the influence of forearm rotation on interobserver agreement. However, their findings support the interobserver agreement found in Jensen et al. 13 as a realistic estimate of interobserver agreement on tilt in true lateral radiographs. This study did not find the same level of improvement with true lateral radiographs as Jensen et al. 13 and Christersson et al. 9 However, this might be explained by the use of non-fractured versus fractured forearms, which is the biggest methodological difference between this and the aforementioned studies. Perhaps the anatomical deformity brought on by a DRF visually depicts the landmarks used when measuring tilt more clearly, improving observer agreement.
An important finding of this study was that supination improved interobserver agreement on tilt, contrasting with pronation, which worsened it. The clarity of bone landmarks might also explain this difference since there is appreciable bone overlap on a lateral radiograph, and rotation affects how the overlap appears. The distal articular surface of the radius is angled in more than one plane. The articular surface of the radius is inclined in the volar direction while simultaneously being inclined in the direction of the ulna. With rotation, these angles might affect one another. 12
The association between supination and improved interobserver agreement has rarely been examined in previous studies. A similar tendency was recognized in Johnson et al. 11 in which five non-fractured cadaveric arms were rotated 20° to either side and radiographed with 5° intervals, and interobserver variance on tilt between 15 orthopedic surgeons was quantified using the mean standard deviation. Examining the data of Johnson et al., 11 it appeared the agreement was superior with supination compared to pronation. This tendency was not discussed in the study. However, the best agreement was with 15° supination (1.17°), which was superior to the agreement of the 0° reference rotation (4.76°). The agreement was worst with 10° of pronation (5.56°). These findings supported the tendency found in this study.
Therefore, the next question inevitably is if the forearm should be slightly supinated in a lateral radiograph instead? However, forearm rotation not only impacts the interobserver agreement. Several studies have reported that forearm rotation changed the measured value of dorsal/volar tilt in both fractured and non-fractured forearms, potentially making the measurement less reliable in the treatment decision. These studies all found that supination led to the overestimation of volar tilt by 3–6.8° per 10° of supination and that pronation led to a corresponding underestimation.11,13–16 Hence, while the findings of this study were surprising and significant, we cannot recommend changing the clinical practice of how the lateral radiograph is taken when diagnosing a DRF. Furthermore, the current method using the pisoscaphocapitate relationship 18 is more reproducible than aiming for an exact angulation of supination, which supports the use of a true lateral projection in clinical practice. 18
The sample size of this study posed both a strength and a limitation. Similar studies using cadaveric arms included between five and nine specimens for examination.11,15,16 Comparatively, this study examined 21 specimens. This set of specimens provided a satisfactory sample size of 147 total radiographs. However, when exclusively analyzing the true lateral radiographs, the sample size was only 21 radiographs, resulting in broad CIs, which posed a limitation to this study. All radiographs in the current study were obtained with the central ray perpendicular to the radio-carpal joint. It has previously been reported though, that angulating the tube between 15 and 20° in the proximal direction improves visualization of the articular surface and therefore improves measurement consistency.17,21 Angulating the central ray away from perpendicular will however introduce a degree of geometric distortion in the radiograph and depict the carpal bones with more overlap as opposed to in the perpendicular view. More research is needed to explore the impact of tube angulation on various measurements obtained from the lateral wrist radiograph not only in relation to DRF but also carpal measurements.
In conclusion, this study found that forearm rotation did not significantly influence interobserver agreement on tilt. However, when isolating and comparing the direction of rotation, interobserver agreement significantly improved with supination and worsened with pronation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.