
Abstract
Other than the expected abdominal pain post-embolization, only few complications occur after uterine artery embolization (UAE). Necrotic cavitation of adenomyosis is a particularly rare complication. Here, we describe a patient with adenomyosis who experienced persistent fever after UAE, which ultimately resolved with the spontaneous expulsion of adenomyosis.
Introduction
Although surgical hysterectomy is considered the sole definitive treatment for adenomyosis, UAE has been performed as a minimally invasive alternative. A recent meta-analysis revealed that 83.1% of patients with adenomyosis exhibited improvements in clinical symptoms after UAE. 1
Case
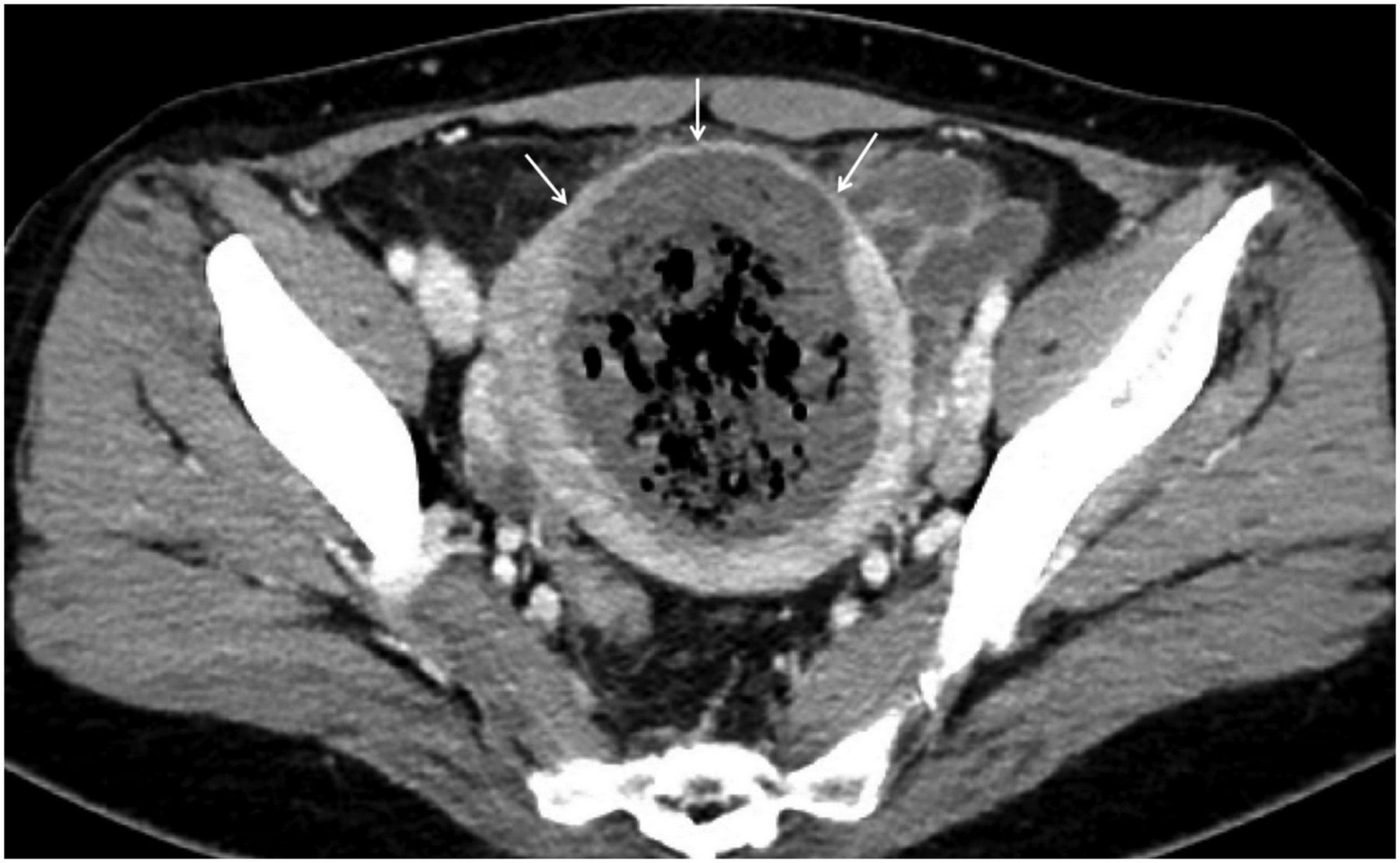
A 46-year-old woman with no history of coitus presented to our clinic with severe menorrhagia and dysmenorrhea, as well as urinary frequency and pelvic heaviness. Magnetic resonance imaging revealed diffuse enlargement of the uterus with multiple bright foci, which suggested diffuse adenomyosis (Figure 1). Bilateral UAE was performed using polyvinyl alcohol particles (Bearing; Merit Medical) with sizes of 150–250 μm and 250–355 μm, followed by the use of tris-acryl gelatin microspheres (Embosphere; Merit Medical) with sizes of 300–500 μm and 500–700 μm. Embolization was performed until complete cessation of blood flow was observed for an interval of 10 heartbeats. There were no immediate post-procedural complications, and the patient was discharged uneventfully on the next day after the procedure. Two weeks later, the patient returned to the clinic with a fever of 38.5–39°C and foul-smelling vaginal discharge. Her C-reactive protein level had increased to 55.8 mg/L (normal: 0–8 mg/L), and her white blood cell count had increased to 15,060/μL (normal: 4,000–10,800/μL). Conservative treatment was initiated with a 2-week course of cefixime and metronidazole. However, the patient returned with persistent fever and leukocytosis. Pelvic computed tomography revealed complete necrosis of adenomyosis and cavitation with an air-forming abscess (Figure 2) despite the preservation of normal myometrium. The patient was hospitalized for treatment with intravenous cefotiam, amikacin, and metronidazole. After 5 days of treatment, the patient’s leukocytosis and inflammatory markers improved, and she was discharged. Approximately 6 weeks after discharge, the patient returned with recurrent fever, which coincided with her first menstrual period after UAE. Follow-up computed tomography revealed a persistent abscess, although its size had decreased (Figure 3). Thus, the patient was prescribed antipyretics alone. Three days after her clinic visit, she reported vaginal expulsion of pus-like material considered as necrotic adenomyosis and subsequent improvement in fever. Symptoms of menorrhagia, dysmenorrhea, urinary frequency, and pelvic heaviness substantially improved after the expulsion of necrotic adenomyosis. Magnetic resonance imaging at 6 months after UAE showed considerable reduction in uterine size (Figure 4). Magnetic resonance imaging shows diffuse enlargement of the uterus with multiple bright foci on T2-weighted imaging, consistent with adenomyosis. On computed tomography at 1 month after uterine artery embolization, complete necrosis of adenomyosis with air bubbles in the uterine cavity, suggesting that the adenomyosis had developed cavitation and become infected. Normal myometrium (arrows) is visible. Computed tomography two and a half months after embolization reveals that the abscess cavity was smaller but remained. Magnetic resonance imaging at 6 months after uterine artery embolization reveals considerable reduction of uterine size and restoration of normal uterine structure.


Discussion
Although surgical hysterectomy is considered the sole definitive treatment for adenomyosis, UAE has been performed as a minimally invasive alternative. Notably, the success rate of UAE is high when embolization is performed with polyvinyl alcohol particles that successively increase in size from 150–250 μm to 250–355 μm and then to 355–500 μm. 2
Although fibroids can reportedly develop cavitation and become infected after UAE, leading to leiomyoma expulsion, this phenomenon is extremely rare after UAE for adenomyosis. Kunchala et al. 3 recently reported a similar case, which initially involved conservative management followed by hysteroscopic resection for persistent necrotic adenomyosis. Although we considered hysteroscopic resection for our patient, she reported no history of coitus and refused to undergo an additional procedure; thus, only conservative treatments were performed. Whereas our embolic agent comprised polyvinyl alcohol particles with sizes of 150–250 μm and 250–355 μm at the beginning of embolization, Kunchala et al. used Embospheres with sizes of 500–700 μm. Thus, we suspect that particle size is unrelated to the onset of cavitation and infection after UAE. Magnetic resonance imaging has been used to assess the risk of fibroid cavitation, but risk factors for cavitation in patients with adenomyosis are unknown.
In conclusion, adenomyosis can develop cavitation and become infected after UAE in a manner similar to fibroid cavitation. Although hysteroscopic resection may be a reasonable approach, our findings suggest that conservative management is effective and should be regarded as a first-line treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.