
Abstract
Background
Imaging-guided percutaneous biopsy of renal masses is regarded as safe and is widely used for histopathology diagnosis before treatment. Recommended observation time after tumour biopsy varies in international guidelines and the literature is sparse.
Purpose
To assess the effect of a 1-h post-biopsy observation time of percutaneous image-guided renal mass biopsy.
Material and Methods
This was a single-centre retrospective study. During January 2015 to September 2019, a total of 484 patients underwent renal mass biopsies. 4-h-observation-group: 178 patients and 1-h-observation-group 306 patients. All records were retrospectively reviewed, and data such as complications was obtained and compared between the two groups.
Results
A total complication rate of 4.5% (n = 22) without any major complications (Cardiovascular and Interventional Radiological Society of Europe-grade (CIRSE) 5–6). Furthermore, a non-significant difference of 1.3% of the 1-h group and 3.4% in the 4-h group experiencing complications was found (p = .18). A total biopsy-accuracy of 84% was observed.
Conclusion
This study shows that renal mass biopsy is safe with no major complications. This suggests that an outpatient approach with 1-h-observation time can be safely implemented for renal mass biopsy.
Introduction
The incidence of renal cancer is increasing worldwide 1 due to an increased amount of abdominal imaging leading to incidental findings of small renal masses.2,3 Ultrasound (US)- and Computed tomography (CT)-guided percutaneous renal tumour biopsy (PRTB) is a common procedure following an incidental finding of an indeterminate renal mass on either a magnetic resonance (MR) or CT scan. 4 Studies have shown that PRTB prior to treatment is of high diagnostic value and a favourable option regarding subtype histopathological analysis of the presented renal mass in regard to accuracy and rate of complications. 5
Percutaneous renal tumour biopsy has been proven to be of use in an outpatient setting with a short post-biopsy observation time, when sudden onset complications are not present, proving it to be an efficient and reliable choice. 6
A study on short-duration post CT-guided thoracic biopsy observation time concluded that a 30-min observation time in patients without immediate complications related to the procedure was sufficient. 7 The outcome of this shortening of observation time regarding renal mass biopsy has not yet been evaluated.
The aim of this study was to evaluate the outcome after 1-h and 4-h post-biopsy observation time of PRTB.
Material and methods
Patient inclusion and data collection
This retrospective, single-centre study was approved by the National Patient Safety Authority (19/44304). Data from PRTBs performed on 484 patients at Odense University Hospital in Odense, Denmark between the 1 January 2015 and the 30 September 2019 were retrospectively reviewed and collected. All data enquired for the study was obtained from electronic patient journals, Picture Archiving and Communication System (PACS), Radiology Information System (RIS) and pathology records by author JV and any questions or problems were discussed with senior consultant in radiology (OG).
Only biopsies of renal masses originating from renal tissue were included. Therefore, any biopsies of retroperitoneal masses with relations to the kidneys, biopsies of metastases or diagnostic biopsies of renal parenchyma were excluded. Furthermore, any cancelled, attempted or discontinued biopsies due to lack of compliance were excluded (Figure 1). Flowchart illustrating exclusion of patients.
For every patient, demographic information such as age and sex were collected. Furthermore, any use of anti-hypertensive and/or antithrombotic drugs were collected.
For each renal mass, the localisation was confirmed by a CT-or MR-scan obtained prior to the biopsy. The diameter of the mass was measured in the coronal plane. The distance from skin to tumour was measured in axial plane. Information about the renal mass’ solid, cystic and/or solid-cystic components were collected. It was also recorded if the renal mass was endo- or exophytic and if the renal mass was located in the upper, central or lower pole. Regarding the procedure of PRTB of each mass, the modality used, number of samples collected, and post-biopsy observation time was collected.
On the 1 March 2017, the guidelines for post-biopsy observational time at our institution was changed from 4 h to 1 h. Therefore, the 4-h-observation-group was sampled from patients undergoing PRTB from 1 January 2015 to 28 February 2017 and patients in the 1-hour-observation-group from 1 March 2017 to 1 September 2019.
The accuracy was calculated as the number of conclusive diagnoses of renal masses out of the total amount of PRTBs. Inconclusive biopsies are defined as tissue not being obtained from the renal mass, resulting in the pathologist not being able to properly diagnose the received material.
Biopsy procedure
Every renal mass was presented on a conference in which both subspecialised urologists and radiologists attended. Patients with renal masses with a size over 2 cm are offered a biopsy. Patients were informed about the procedure and risks of complications and consent was given. All patients using anticoagulant medication was informed to pause the therapy and eventually receive replacement therapy in form of subcutaneous anticoagulation prior to the biopsy in accordance with national guidelines. 8 Any patient unable to comply had their procedure cancelled. At the time of biopsy, all patients had acceptable coagulation status measured by international normalised ratio (INR) and platelet count.
Biopsies were performed in the department of radiology by trained radiologists under guidance either by US or CT using an 18G core-needle for every procedure (SemiCut, M.D.L. Srl, Via Tavani 1/a, 23014 Delebio, Italy). Ultrasound remained the primary choice for any mass, leaving the CT-guided approach for masses which were either difficult to visualise or considered difficult to properly reach under US-guidance. Prior to the biopsy, patients underwent either multiphase CT- or MR-imaging of the kidney(s) for characterising the mass, securing the best point of entry and distance from the skin to the mass. Biopsy location was anesthetised using 10–20 mL Lidocaine (10 mg/mL). The biopsy material was sent directly for histopathological analysis.
Before leaving the hospital, patients were thoroughly informed on whom to contact in case of any late-onset complications.
If the patient presented symptoms of acute complications, US assessment of the region or a CT scan was performed. In case of any complications, patients were kept in hospital for observation and, if necessary, adequate treatment was started.
Any sudden or late-onset complication was noted. Sudden complication is defined as a complication which occurs during the time of the procedure. Delayed onset is any complication which occurs after the procedure – either during the observation period or after the patient is sent home and returns with any persistent problems relevant to the biopsy within the following days post-biopsy. Classification regarding severity of the complication was made using the Cardiovascular and Interventional Radiological Society of Europe-grade (CIRSE) Classification System for Complications in concordance with guidelines from the Cardiovascular and Interventional Radiological Society of Europe. 9
Statistical analysis
All statistical calculations and approximations were done using STATA16. Wilcoxon Rank Sum test was used for any non-normally distributed data and Fisher’s exact test was used for any binomial data. A p-value < .05 was considered statistically significant.
Results
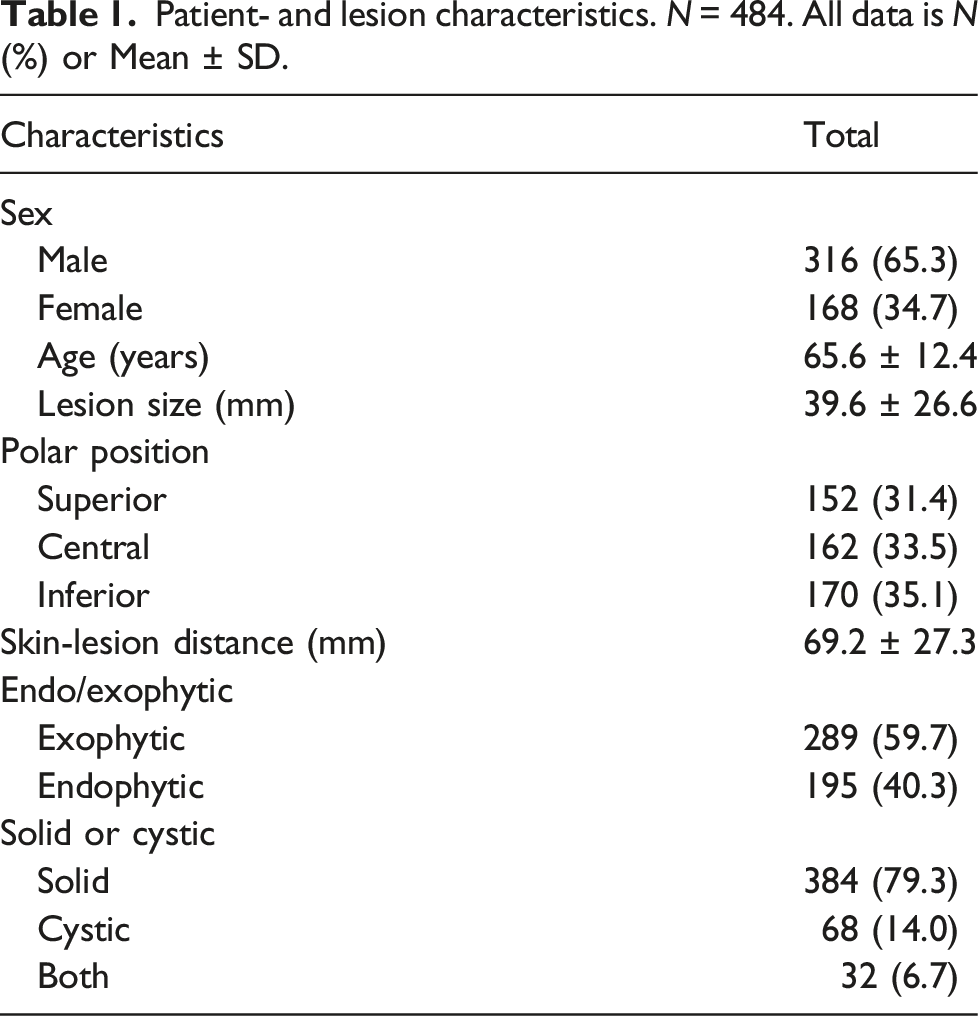
Patient- and lesion characteristics. N = 484. All data is N (%) or Mean ± SD.
Distribution of malignant and benign diagnoses in patients with a positive primary biopsy.
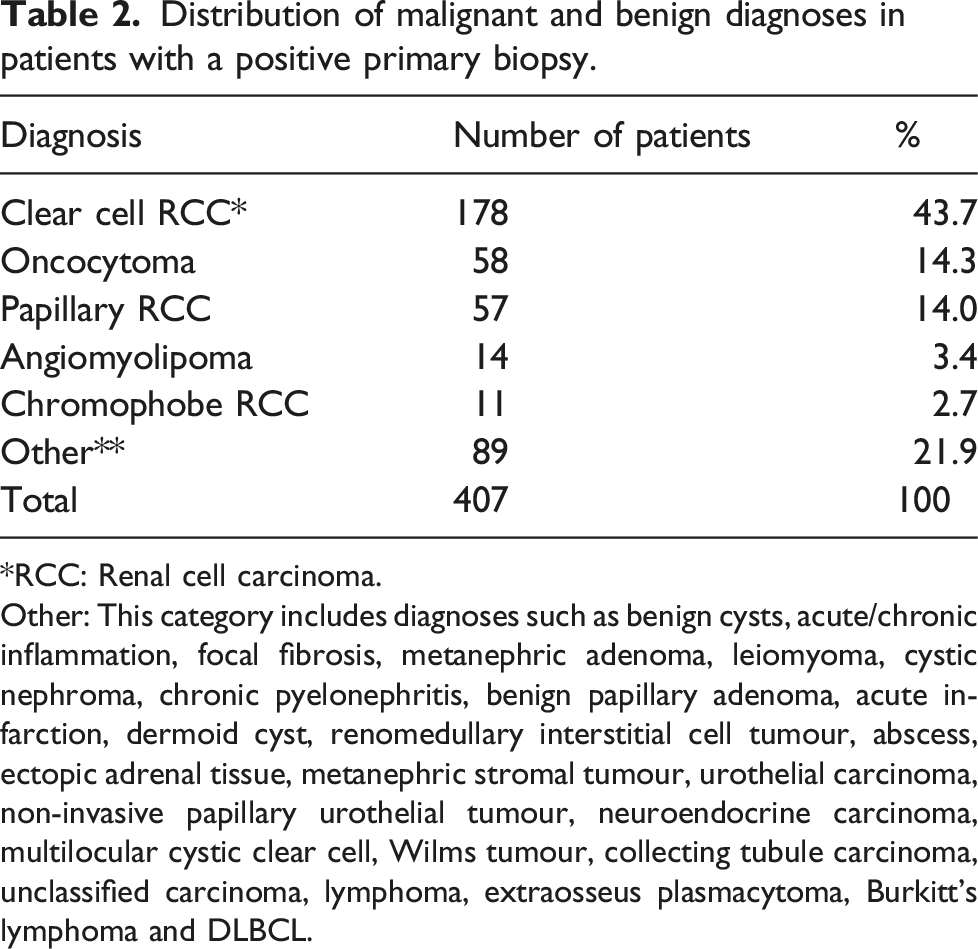
*RCC: Renal cell carcinoma.
Other: This category includes diagnoses such as benign cysts, acute/chronic inflammation, focal fibrosis, metanephric adenoma, leiomyoma, cystic nephroma, chronic pyelonephritis, benign papillary adenoma, acute infarction, dermoid cyst, renomedullary interstitial cell tumour, abscess, ectopic adrenal tissue, metanephric stromal tumour, urothelial carcinoma, non-invasive papillary urothelial tumour, neuroendocrine carcinoma, multilocular cystic clear cell, Wilms tumour, collecting tubule carcinoma, unclassified carcinoma, lymphoma, extraosseus plasmacytoma, Burkitt’s lymphoma and DLBCL.
Further diagnostics for inconclusive primary biopsies.

Rebiopsy: CT- or US-guided rebiopsy.
Watchful waiting/active surveillance: Scheduled follow-up appointment(s) and surveillance of tumour.
End: No further diagnostics – either treatment without diagnosis or patient completely refraining from further diagnostics.
Death: Patient did not receive further diagnostics due to passing away from other reasons than due to PRTB.
Oncological treatment: Patient received chemo- or radiation therapy.
Total: Total number of patients with inconclusive pathological diagnosis from primary or rebiopsy.
Risk factors for complications.

All data is N (%) or Mean ± SD
*This calculation was performed with n = 482 due to missing data on amount of samples. Neither of the excluded patients experienced complications.
CIRSE-classification of complications from primary biopsies.

CIRSE 1: Complication during the procedure which could be solved within the session; no additional therapy, no post procedure sequelae, no deviation from the normal post-therapeutic course.
CIRSE 2: Prolonged observation including overnight stay (<48 h); no additional post procedure therapy, no post procedure sequelae.
CIRSE 3: Additional post procedure therapy or prolonged hospital stay (>48 h) required; no post procedure sequelae.
CIRSE 4: Complication causing permanent mild sequelae (resuming work and independent life).
CIRSE 5: Complication causing permanent severe sequelae (requiring ongoing assistance in daily life).
CIRSE 6: Death.
Discussion
This study found an overall complication rate after renal mass biopsy to be low with no casualties or severe complications. There was no significant difference observed between the two groups of 1- and 4-h observation after renal mass biopsy.
Generally, PRTB and medical renal biopsies are considered as safe procedures with a low frequency of complications.10–12 This was confirmed by our study, where the overall rate of complications is lower than the median of 8.1% (IQR: 2.7%–11.1%) reported in the latest systematic review by Marconi et al. 5 Furthermore, the majority of complications in our study had CIRSE-grade 1 (50%, n = 11) and 2 (27.3%, n = 6). This low number of major complications is well in line with other studies’ rate of complications as observed by Marconi et al., who reported only three complications with a Clavien-Dindo grade ≥ 2 out of 22 studies. 5
Other similar studies found that a short observational period of 30 min to 4-h post-biopsy is feasible.6,7 The implication of this could mean greater efficiency with patients leaving the hospital earlier and therefore requiring less funds and time from personnel for post-biopsy assistance. Frimpong et al. concluded that observational period post-biopsy as little as 30 min was proven to be sufficient in cases where no imminent post-procedural complications was presented after a routine CT scan following a CT-guided thoracic biopsy. 7 Deciding the length of the observational period should not only be decided on the basis of a low complication rate, but also the consequences of the complication. In this study, 23% (n = 5) out of the 22 patients with complications needed post-procedural therapy. With a very low overall complication rate together with an even lower number of patients needing therapy because of the complications, a post-biopsy observational time of 1 h seems safe.
In regard to risk factors of complications, the significant difference in the number of samples in the complications versus non-complications group could have a possible clinical value. Complications after PRTB are, as mentioned above, rarely severe, and complications occurring within the procedure would be treated straight away regardless of severity. If there was a significantly higher rate of complications after 1 h of observation, and the procedure had more severe complications both in the literature and this specific study, the found significant difference would be of more clinical value. Moreover, the lower mean age in the complication group with a p-value = .05 was deemed as a coincidence and should not be used to influence the patients’ observation period. More studies are therefore needed within this subject.
With an overall accuracy of 84%, this study had a lower median accuracy than the 92% reported by Marconi et al., 5 although it is still within the reported interquartile range (80.6%–96.8%). This difference in accuracy can be explained by the fact that our institution performs biopsy of all complex renal cystic masses with Bosniak ≥ 2F. Biopsy of cystic masses are clinically challenging and managed differently among institutions with malignancy being found in up to 12% of Bosniak ≥ 2F lesions.13–16
Although a high accuracy was found, some patients received inconclusive histopathological reports. The majority of these patients had repeat biopsies of the mass. In a study by Golan et al., the majority (60%) of patients stated that they wanted a biopsy of their renal mass even if it had some degree of inaccuracy. The patients’ minimal accepted accuracy was 80–99%, which is well in line with the accuracy of both first and second try biopsies in this study. 17 Furthermore, Seager et al. concluded that due to the high accuracy of repeat biopsies following the primary biopsy, a repeat biopsy was to be recommended in case of an inconclusive first biopsy. 18
The present study has some limitations, mainly arising from the fact that it is a retrospective study. All data solely relies on information retrieved from electronic patient records and radiologists’ reports on scans. None of the patients included in the study were followed with scans or follow-up consultations from the study itself, therefore no asymptomatic complications were noted. Furthermore, this study did not include pain as a complication, nor post-procedurally scanned every patient for the presence of asymptomatic complications as, for example, haematomas, which arguably have had an impact on the observed rate of complications. It is feasible that the inclusion of pain as a complication would have increased this rate. Additionally, there is a risk of bias in the time factor between observation after 1 and 4 h. Since the 1-h group is chronologically after the 4-h group, the radiologists performing the procedure’s skill might have increased and equipment upgraded. At our department, performing PRTB is a daily procedure performed by many radiologists with different experience, which have not been measured in this study. Therefore, it is possible that further analysis on this could have shown an effect on the results in the 1-h group. Preferably, a prospective and larger multicentre study would be needed to further assess the findings presented in this study.
In conclusion, this study shows that renal mass biopsy is safe with no major complications. This suggests that outpatient approach with 1 h of observation safely can be implemented for renal mass biopsy in otherwise healthy patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.