
Abstract
Background
Routine CT scans may increasingly be used to document normal aortic size and to detect incidental abdominal aortic aneurysms.
Purpose
To determine whether ultra-low-dose non-contrast CT (ULDNC-CT) can be used instead of the gold standard CT angiography (CTA) for assessment of maximal abdominal aortic diameter.
Materials and Methods
This retrospective study included 50 patients who underwent CTA and a normal-dose non–contrast CT for suspected renal artery stenosis. ULDNC-CT datasets were generated from the normal-dose non–contrast CT datasets using a simulation technique. Using the centerline technique, radiology consultants (n = 4) and residents (n = 3) determined maximal abdominal aortic diameter. The limits of agreement with the mean (LOAM) was used to access observer agreement. LOAM represents how much a measurement by a single observer may plausibly deviate from the mean of all observers on the specific subject.
Results
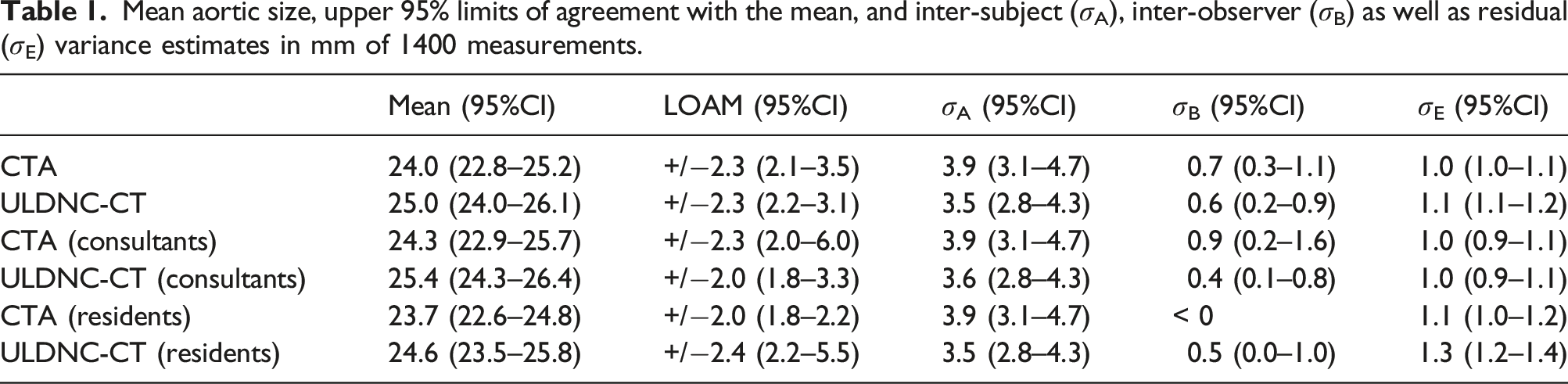
Observers completed 1400 measurements encompassing repeated CTA and ULDNC-CT measurements. The mean diameter was 24.0 and 25.0 mm for CTA and ULDNC-CT, respectively, yielding a significant but minor mean difference of 1.0 mm. The 95% LOAM reproducibility was similar for CTA and ULDNC-CT (2.3 vs 2.3 mm). In addition, the 95% LOAM and mean diameters were similar for CTA and ULDNC-CT when observers were grouped as consultants and residents.
Conclusions
Ultra-low-dose non–contrast CT exhibited similar accuracy and reproducibility of measurements compared with CTA for assessing maximal abdominal aortic diameter supporting that ULDNC-CT can be used interchangeably with CTA in the lower range of aortic sizes.
Introduction
A clear evidence-based indication for elective abdominal aortic repair exists with a cut-point of maximum abdominal aortic diameter (Dmax) at 5.5 cm or when rapid growth (> 10 mm/year) is observed. Population-based systematic screening programs following this algorithm are cost-effective in reducing mortality and are recommended in guidelines.1,2,3 However, the evidence for systematic screening has existed for decades, so the likelihood of population-based screening programs being implemented in countries without current programs established is low. Here opportunistic screening could be the optimal alternative. In contrast to population-based screening, opportunistic screening happens on an ad hoc basis initiated by individuals, healthcare providers, or the healthcare systems. 4
Ultrasound is the standard imaging modality in screening and surveillance of AAA. Computed tomography angiography (CTA) is considered the gold standard in assessing the maximal abdominal aortic diameter, and compared to ultrasound, CTA is more expensive, less available, and requires ionizing radiation and iodinated contrast, which may carry a risk in prolonged surveillance and patients with chronic renal failure. However, several studies have investigated the utility of using pre-existing imaging, mainly CT, in opportunistic screening for AAA.5-12 In two studies from England and the USA, 21% of patients invited for screening had already undergone a radiological investigation that could have diagnosed an AAA. 9 Another series reported that 48% of patients eligible for screening had undergone prior abdominal imaging. 7 It has been suggested that such routine CT scans can be used not only to identify aneurysms but also to document normal aortas that need no further screening.6,7,8,12
The American College of Radiology Appropriateness Criteria deems normal dose non–contrast CT as diagnostically equivalent to ultrasound for AAA detection. 13 Yet, routine CT scans performed with different protocols for documenting normal aortas may not be readily accepted by all health professionals as evidenced by the guideline from the European Society for Vascular Surgery. 2
The lowest quality CT scans employed in the clinic are those performed at a significantly reduced radiation dose level (i.e., ultra-low-dose CT) which comes at the expense of increasing image noise. 14 No study has investigated if the reproducibility and accuracy of low-dose non-contrast CT are comparable to the gold standard CT angiography in assessing the maximal abdominal aortic diameter.
Consequently, the purpose of this study is primarily to assess the interchangeability of ultra-low-dose non–contrast CT (ULDNC-CT) and standard-dose CTA in terms of accuracy and reproducibility in determining maximum abdominal aortic diameter. Secondarily, to determine the average time spent completing such measurements.
Material and methods
Patient population
In this retrospective single-center study, 50 consecutive patients over the age of 50 with a non-operated abdominal aorta who underwent a CT as part of the workup for suspected renal artery stenosis were included. All CT scans were identified in the picture archiving and communication system (PACS) of the radiology department at our university-based hospital. A screenshot of each patient’s aorta is available for review in Supplemental appendix A.
Computed tomography protocol
Non-contrast and arterial phase images were obtained for all patients with a slice thickness and increment of 2 and 1 mm, respectively. Additional protocol details can be found in Supplemental appendix B.
Dose-length product (DLP) stored in our PACS system was retrieved for all 50 non-contrast scans, and the effective dose was estimated by multiplying the DLP with a conversion factor of 0.018 mSv/mGy*cm. 15 The mean DLP and effective dose from the non-contrast CTs were 546 (±203) mGy*cm and 9.8 (±3.6) mSv, respectively.
Dose reduction simulations
We used a previously demonstrated technique for simulating lower dose CT scans by adding measured noise samples to Digital Imaging and Communications in Medicine (DICOM) images (Figure 1).16,17 Clinical scans can retrospectively be used for simulating lower dose scans which avoid irradiating patients multiple times. The simulated lower dose CT approximates images reconstructed with filtered back-projection at a mean DLP and effective dose of 37 (±25) mGy*cm and 0.7 (±0.4) mSv, respectively. An average effective dose of < 2 mSv for a CT of the abdomen is consistent with the definition of ultra-low-dose CT.
18
Details of the simulation technique can be found in Supplemental Appendix B. Axial slices from the original normal-dose non–contrast CT A) and simulated low-dose non–contrast CT B) at the origin of the coeliac trunk. The transition between the abdominal aorta and the left crus of the diaphragm is substantially less conspicuous on the simulated low-dose non–contrast CT owing to the increased noise.
Observers
Resident (n = 3) and consultant (n = 4) radiologists from the Department of Radiology at Aarhus University Hospital were recruited. The eligibility criteria were: 1) more than three years of radiological experience, 2) experience with diameter measurements using double oblique multiplanar reconstruction, and 3) had interpreted CT scans covering the abdominal aorta at least once a month during the previous 12 months. The included radiologists had a mean age (±SD, range) of 37.9 years (± 3.8, 33–46), a mean in years of CT experience of 7.9 years (± 3.2, 4–15), and all were university hospital-based.
Measurement platform
A previously utilized web-based platform for facilitating imaging observer performance studies was used. 19 The platform was coupled with a web-based DICOM viewer with on-the-fly multiplanar reconstruction (MPR) capability.20,21 The simulated ULDNC-CT and CTA studies were anonymized and randomized.
Measurements
Various imaging planes for Dmax measurement are available in clinical practice. However, the real Dmax is found on cross-sections perpendicular to the aorta centerline, which will vary in the presence of aortic tortuosity. Consequently, this measurement approach is the one recommended in reporting standards for AAA.2,22,13
For both ULDNC-CT and CTA, observers used the on-the-fly MPR functionality of the DICOM viewer to identify the cross-section perpendicular to the aortic centerline containing the maximum diameter in any direction. The aorta from below the coeliac trunk to the aortic bifurcation was evaluated. Diameters were measured from the outer to outer wall of the aorta (Figure 2). If observers found no aortic ectasia (i.e., Dmax < 2.5 cm), they were instructed to place calipers in the maximum cross-section perpendicular to the aortic centerline just below the coeliac trunk. Representative images of Dmax caliper placement using the web-based DICOM viewer with centerline technique. A) ultra-low-dose non-contrast CT and B) CT angiography.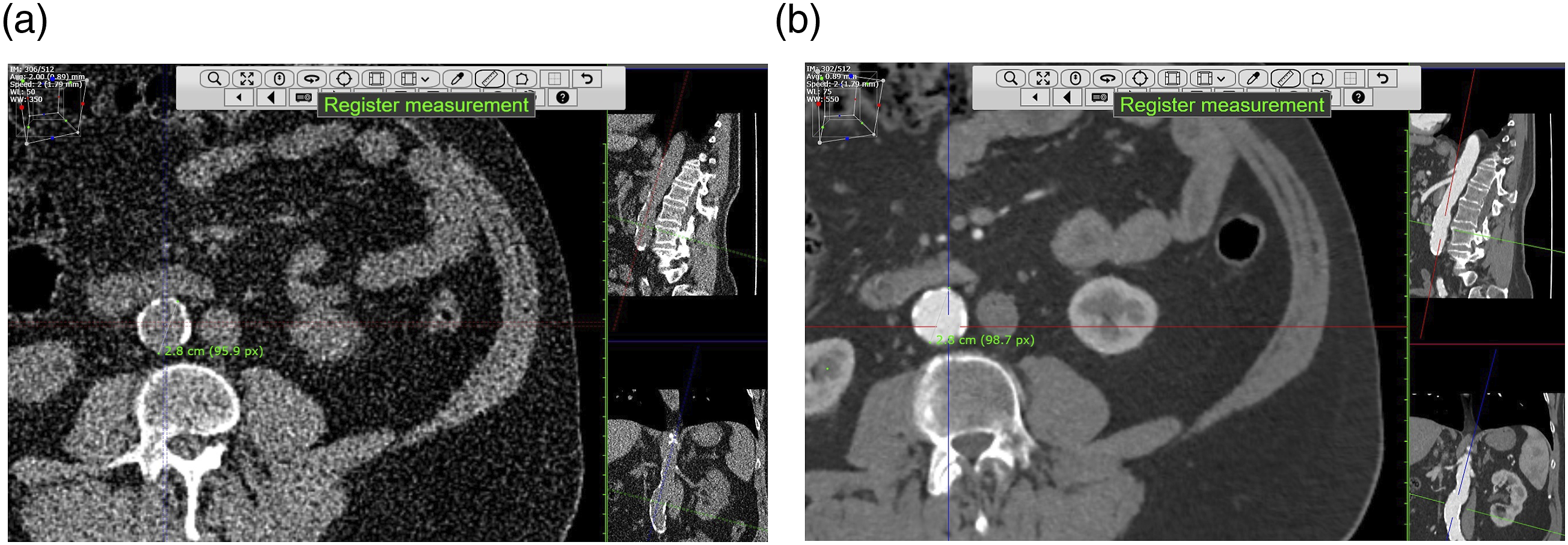
For estimating inter-observer variability, each observer measured the Dmax of the 50 ULDNC-CT and 50 CTA scans for a total of 100 measurements each.
For investigating intra-observer variability, observers repeated measurements for an additional 100 measurements completed by each observer. Reading sessions were separated by a minimum of 1 week. In each reading session, the review of the 50 simulated ULDNC-CT datasets preceded the review of the 50 corresponding CTA datasets. Furthermore, the observers were blinded to all technical parameters, clinical data, previous measurements, the key images, and the measurements taken by other observers.
Each measurement duration taken from when a scan had loaded until the measurement was completed was recorded in the platform database.
Statistical analysis
T-tests were used to assess differences in mean diameters and reading time between ULDNC-CT and CTA. To assess observer agreement for continuous measurements in a multi-observer setup, we used the limits of agreement with the mean (LOAM).
23
The LOAM represents how much an observer’s measurement may plausibly deviate from the mean of all observers’ measurements on the specific subject (i.e., a measure of the combined intra- and interobserver variation) and can be interpreted as the measurement reproducibility. For data visualization, an agreement plot of the observed differences against the observed subject-specific mean is constructed. The LOAM is formulated under an additive two-way random effects model to integrate inter-subject (
To enable an easier comparison with prior studies, 24 we calculated Bland-Altman limits of agreement (LoA) for the repeated diameter measurements completed by each observer (n = 7) for ULDNC-CT and CTA. In addition, we calculated the LoA of the first session CTA versus the first session ULDNC-CT measurements for each observer (n = 7). Furthermore, we evaluated LoA of first session diameter measurements between observer pairs (n = 21) of the seven observers for CTA, ULDNC-CT, and CTA versus ULDNC-CT. When applied to AAA diameter analysis, the clinically accepted range of the limits of agreement has been set to −5 mm to +5 mm. 25
A small pilot study including three observers measuring aortic diameters on 50 ULDNC-CT scans was conducted. Based on obtained measurement variation, it was estimated that seven observers would be needed to obtain an expected 1.0 mm width of the 95% CI for the 95% LOAM.
An image of each caliper placement was automatically saved in the platform database. Measurements deviating more than 3 mm from a given subject mean were investigated to identify sources of inaccuracy.
The degree of abdominal aortic calcification was quantified with a validated CT score ranging from zero to six; six indicates severe calcification and a score of zero is given if no calcification is present. 26 Associations between measurement variation (defined as standard deviation (SD) of the differences of observers from the mean for each subject) and mean abdominal aortic diameter, patient age, BMI, and aortic calcification were evaluated with Pearson correlation coefficients.
Results
Mean aortic size, upper 95% limits of agreement with the mean, and inter-subject (
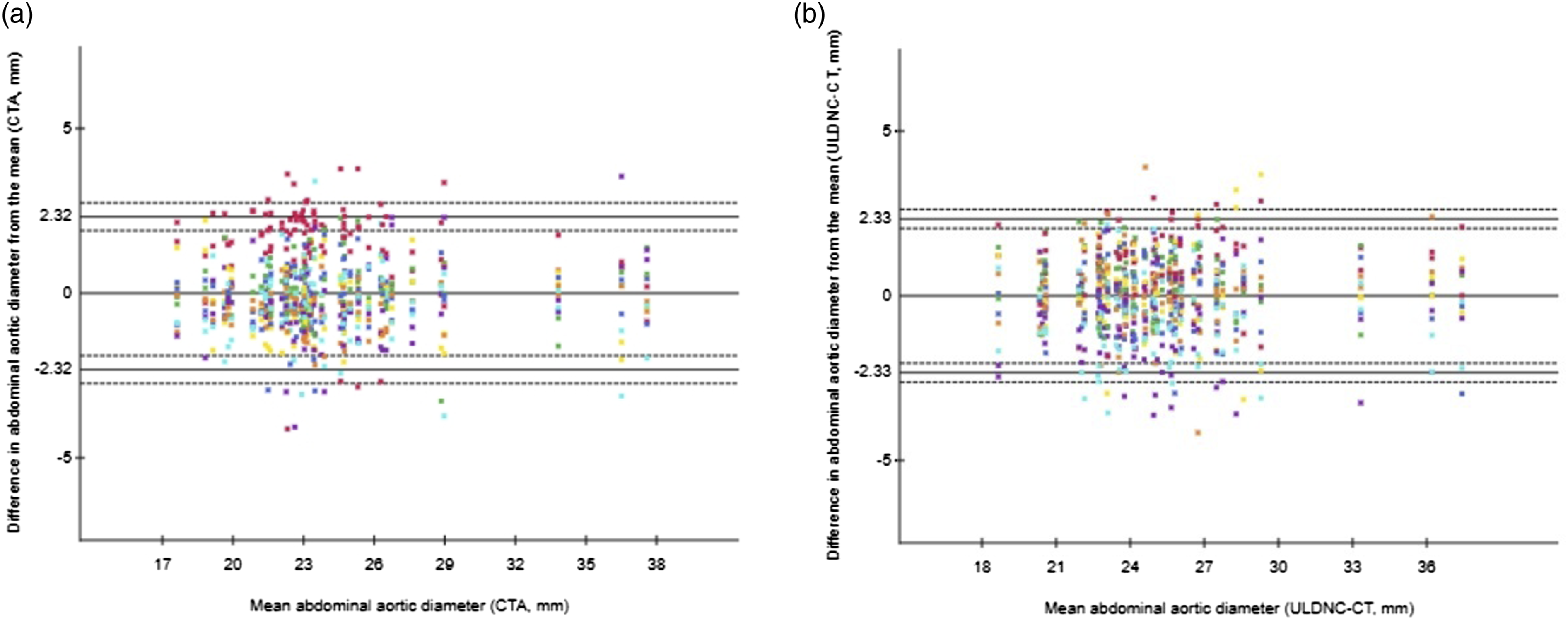
Observer agreement plots for measurements of abdominal aortic diameter in millimeters of the 1400 measurements in A) CT angiography and B) ultra-low-dose non–contrast CT, respectively (horizontal axes represent the patient-specific mean aortic diameter measurements, vertical axes represent the difference from the aortic diameter measurements to the patient-specific mean. Differently colored dots represent individual measurements of the seven observers. Note some dots have been superimposed. Horizontal solid lines indicate upper and lower 95% limits of agreement with the mean and a line of zero difference. Dashed lines correspond to the 95% confidence intervals for the limits of agreement).
Largest Bland-Altman bias, limits of agreement of measurements, and pairs outside of clinically accepted range for all seven observers.

Causes of measurement deviations more than 3 mm from the subject-specific mean for all seven observers evaluating 50 CTA (n = 13 deviations) and ULDNC-CT (n = 14 deviations) datasets.

In addition, as seen in Table 1, both the 95% LOAM and mean diameter were similar for CTA and ULDNC-CT when observers were grouped as consultants and residents.
The Pearson correlations (95% CI, p) between abdominal aortic diameter, patient age, BMI, and aortic calcification versus the SD of the differences of observers from the mean of the 50 abdominal aortas measured were r = 0.11 (−0.18 to 0.37, p = 0.46), r = −0.05 (−0.32 to 0.23, p = 0.75), r = 0.08 (−0.20 to 0.35, p = 0.59), r = 0.00 (−0.28 to 0.28, p = 0.99), and r = 0.19 (−0.09 to 0.44, p = 0.19), r = 0.21 (−0.07 to 0.46, p = 0.14), r = -0.05 (−0.32 to 0.23, p = 0.74), r = 0.12 (−0.16 to 0.39, p = 0.41) for CTA and ULDNC-CT, respectively.
For all observers, the average time to obtain a Dmax measurement was 80 s (95% CI 43–119) for CTA and 112 s for ULDNC-CT (95% CI 75–150), yielding a mean difference of 32 s (95% CI 19–44, p < 0.001).
Discussion
The study’s major findings were the following: ULDNC-CT is comparable to CTA for assessment of Dmax in terms of reproducibility as reflected by the similar LOAM. We found a significant minor mean difference of 1.0 mm in diameter estimates between ULDNC-CT and CTA. The Bland-Altman LoA observer pairs that went beyond the clinically acceptable range of +/− 5 mm only did so with a relatively small margin. The small inter-observer variance components for both the CTA and ULDNC-CT support the use of different observers in Dmax assessment, albeit care must be taken regarding consensus on how to place calipers in relation to the aortic wall.
Given the high noise level of the ULDNC-CT images, it was somewhat surprising but nonetheless encouraging that the evaluation of these studies was valid and fast and did not take much longer than the evaluation of the CTA studies. The finding of a minor mean difference in diameter estimates between ULDNC-CT and CTA is likely due to the increased noise in the ULDNC-CT, making it more challenging to differentiate the aortic adventitia from peri-aortic fat clearly.
The principal strength of this study is the inclusion of a relatively large number of observers, compared to prior studies, with different degrees of experience. 27 Only one radiologist was a fellow in vascular interventional radiology, and hence our findings should be generalizable to radiologists who practice in diverse settings outside of specialized vascular centers.
The use of CTA in the assessment of AAA has been extensively studied. 25 However, only one prior study has investigated the utility of non-contrast and low-dose CT in assessing abdominal aortic size. Liisberg et al. included patients from the DANCAVAS screening trial to validate low-dose non-contrast CT compared to ultrasound as a method for AAA screening. 28 The population evaluated had an age, BMI as well as AAA prevalence comparable to the population of the study at hand. The authors concluded that low-dose non-contrast CT seems superior to ultrasound concerning sensitivity. They found a mean difference of 0.1 mm between the aforementioned modalities in the assessment of Dmax and that the overall Bland-Altman’s limits of agreement between the modalities were just outside the clinically accepted range of +/− 5 mm; however, the authors could not conclude whether this was due to ultrasound or CT measurement imprecision.
Our finding of similar high reproducibility of ULDNC-CT and the gold standard CTA in Dmax assessment suggests that ULDNC-CT has greater reproducibility than ultrasound measurements.
In all, this study, combined with the study by Liisberg et al., demonstrates that Dmax assessed by ULDNC-CT is useable for assessing abdominal aortic size. The non-contrast CT image quality employed in this study is in the range of the lowest image quality and radiation dose used in clinical practice. It follows that all routinely employed CT studies depicting the abdomen, such as CT with contrast in the portal venous phase, can reasonably be expected to be used for assessment of Dmax as compared to the gold standard CTA.
This study has some limitations. Given that we evaluated a population similar to an AAA screening population, only a subset of the abdominal aortas were ectatic (i.e., ≥ 25 mm, n = 18) and aneurysmal (i.e., ≥ 30 mm, n = 4). Although we did not find a significant correlation between measurement variability and aortic size, our demonstrated high reproducibility of Dmax based on ULDNC-CT may not be directly extrapolated to the whole range of aortic size, that is, AAAs larger than 4 cm. Additional studies are needed to document similar accuracy and reproducibility of ULDNC-CT and CTA also in large AAAs. Ideally, such studies should evaluate CT AAA cases displaying interval changes. Nevertheless, in a screening setting most abdominal aortas will be within normal range and the majority of those exceeding the 25 mm threshold for aortic ectasia will be either ectatic aortas (25–29 mm) or AAAs less than 4 cm . 29 The simulated images used in this study do not include possible noise variation due to varying electron densities being present in different tissues. However, they do exhibit an image quality degradation comparable to true CT images obtained at the corresponding lower tube current. The factory limit of 17 mAs on the CT system used in our study was a limiting factor in establishing a dose level and image quality that would yield significant incoherence in measurements. We speculate that accurate and reproducible measurements of aortic Dmax can likely be achieved at even lower image quality.
The finding of ULDNC-CT, and thus other CT studies with higher image quality, to be valid for diagnosis of AAA has implications for clinical practice, potential opportunistic screening, and rationalized systematic screening. As already alluded to, it has been shown that there is an untapped potential in utilizing pre-existing cross-sectional imaging for opportunistic screening for AAA without any additional imaging, radiation exposure, or appointments. Hence, in countries where population-based screening is not implemented, and thus probably never will be, optimization of opportunistic screening may increase the detection rates of asymptomatic cases.10,30 In population-based screening areas, pre-existing abdominal imaging may obviate the need for a screening ultrasound. In addition, opportunistic screening can potentially detect AAAs in patient groups who do not satisfy current screening criteria or would not attend if offered screening. Nonetheless, these constitute a significant proportion of the total number of AAA patients, of which some are at an increased risk of presenting with rupture. 31
A CT conducted for another indication than AAA follow-up after diagnosing an AAA might suffice instead of a follow-up ultrasound. However, as highlighted, more studies are needed to validate ULDNC-CT for this purpose.
Furthermore, results support the use of low-dose non-contrast CT as a screening modality for AAA in a simultaneous screening paradigm suggested for lung cancer. 31 Finally, a ULDNC-CT can be a good alternative to ultrasound screening in obese patients and patients exhibiting significant bowel gas where poor aortic visualization is commonly observed. 32
One should expect that prior CT examinations were already used for opportunistic screening or AAA surveillance when radiologists make their mandatory report of the entire examination. However, Meecham and colleagues have demonstrated that in patients with screening detected AAA, 37% had prior imaging that could potentially substitute a screening ultrasound, but the interpreting imager diagnosed only 40% of AAA cases. 33 Additionally, Claridge et al. audited AAA detection in routine abdominal CT and found an overall miss rate of 35% mainly attributable to smaller aneurysms (i.e., < 40 mm). 6 To fully exploit the potential of these examinations, interpreting imagers should be educated in Dmax measuring and reporting of abnormal findings. One such initiative is the incorporation of structured radiology reporting.34,35 Additionally, electronic transfer of CT scans is easy in modern times, so dedicated labs with vascular services could alternatively make such transfer systematically and do it themselves.
In conclusion, ultra-low-dose non–contrast CT provides accurate and reproducible Dmax measurements validated by the gold standard CTA. Measurements can be completed in a timely fashion compatible with clinical practice. The results of this study suggest ultra-low-dose non–contrast CT imaging of the abdominal aorta can be an appropriate adjunct in AAA screening.
Supplemental Material
Supplemental Material - Ultra-low-dose non-contrast CT and CT angiography can be used interchangeably for assessing maximal abdominal aortic diameter
Supplemental Material for Ultra-low-dose non-contrast CT and CT angiography can be used interchangeably for assessing maximal abdominal aortic diameter by Jens Borgbjerg, Heidi S Christensen, Rozh Al-Mashhadi, Martin Bøgsted, Jens B Frøkjær, Lise Medrud, Nis Elbrønd Larsen, Jes S Lindholt in Acta Radiologica Open
Supplemental Material
Supplemental Material - Ultra-low-dose non-contrast CT and CT angiography can be used interchangeably for assessing maximal abdominal aortic diameter
Supplemental Material for Ultra-low-dose non-contrast CT and CT angiography can be used interchangeably for assessing maximal abdominal aortic diameter by Jens Borgbjerg, Heidi S Christensen, Rozh Al-Mashhadi, Martin Bøgsted, Jens B Frøkjær, Lise Medrud, Nis Elbrønd Larsen, and Jes S Lindholt in Acta Radiologica Open
Footnotes
Author’s Contribution
All authors attest that they meet the current International Committee of Medical Journal Editors (ICMJE) criteria for Authorship and have made contributions to the paper as specified below. 1. Conception and design of the study; 2. Acquisition of data;3. Analysis and interpretation of data; 4. Drafting the article; 5. Revising the article; 6. Final approval; Jens Borgbjerg [1,3,4,5,6], Heidi S. Christensen [1,3,4,5,6], Rozh Al-Mashhadi [1,2,3,4,5,6], Martin Bøgsted [1,4,5,6], Jens B Froekjaer [2,3,4,5,6], Lise Medrud [2,4,5,6], Nis Elbrønd Larsen [2, 3,4,5,6], Jes S. Lindholt [1,3,4,5,6]
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
This study using retrospective data was approved by the departmental research commitee.
Human rights
The authors declare that the work described has been carried out in accordance with the Declaration of Helsinki of the World Medical Association revised in 2013 for experiments involving humans.
Informed consent and patient details
The authors declare that this report does not contain any personal information that could lead to the identification of the patients.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.