
Abstract
We report a rare case of retroperitoneal pseudotumor caused by Schistosoma japonicum that was diagnosed by computed tomography (CT) guided percutaneous biopsy in a 15-year-old Filipino male. Computed tomography (CT) and magnetic resonance imaging (MRI) revealed a mass lesion, including a mesenteric artery, in the right retroperitoneal space. His mother had a history of S. japonicum infection but his initial stool examination was negative. As schistosomiasis was suspected, cone-beam CT-guided biopsy was performed to enable transcatheter therapeutic arterial embolization to be performed immediately in the event of hemorrhage. Histopathological examination revealed schistosomal eggs. Cone-beam CT-guided technique with a coaxial biopsy system is a safe and accurate diagnostic procedure for S. japonicum retroperitoneal pseudotumor.
Introduction
Schistosomiasis is a common parasitic infection worldwide, but is rarely found in nonendemic areas. 1 In Japan, retroperitoneal masses caused by Schistosoma species are rare. We report a case of retroperitoneal pseudotumor caused by Schistosoma japonicum that was diagnosed by computed tomography (CT)-guided percutaneous biopsy in a Filipino male.
Case Report
An asymptomatic 15-year-old Filipino male came to our hospital for screening for underlying infection after his mother was diagnosed with schistosomiasis. He had grown up in the Philippines, where he had swum in a local river during his childhood. He moved to Japan at the age of 10 years. When he was 14 years old, his mother was diagnosed as schistosomiasis.
Routine blood tests showed elevated alkaline phosphatase and gamma-glutamyl transferase levels. Transaminase levels were normal and stool examination was negative. Unenhanced computed tomography (CT) revealed several calcified lesions in the wall of the ascending and sigmoid colon, ileocolic lymphadenopathy, parenchymal retractions of the liver, hypertrophy of the caudate lobe, dilatation of periportal spaces, and splenomegaly. A mass lesion of soft tissue density, measuring 70 × 16 mm, was seen in the right retroperitoneal space just posterior to the ascending colon (Fig 1(a)). The mass showed gradual homogenous enhancement on dynamic contrast-enhanced CT (Fig 1(b) and (c)). On fluorodeoxyglucose-positron emission tomography (FDG-PET)/CT, the mass had a maximum standard uptake value of 3.3 (Fig 1(d)). Magnetic resonance imaging (MRI) revealed a retroperitoneal mass that was isointense on T1 weighted imaging (WI) and slightly hyperintense on T2WI and showed diffusion restriction (Fig 2(a) and (b)). Homogenous mild enhancement was noted on postcontrast T1WI (Fig 2(c)). CT imaging. (a) Unenhanced CT shows an ill-defined isodense mass without calcification in the right retroperitoneal space. (b) Arterial phase image (taken 35 s after injection of the contrast media, the flow rate was 3.0 mL/s) show a tortuous mesentery artery penetrates the mass (arrow). (c) The mass shows homogenous enhancement in the late phase (taken 120 s after injection). (d) The maximum standard uptake value is 3.3 on FDG-PET CT. MR imaging. T2 weighted (a) and diffusion-weighted imaging (b) demonstrate slight hyperintensity of the mass, and the mean apparent diffusion coefficient (ADC) value is 1.1 × 10−3 mm2/s. (c) Postcontrast T1 weighted imaging shows homogenous gadolinium enhancement of the mass.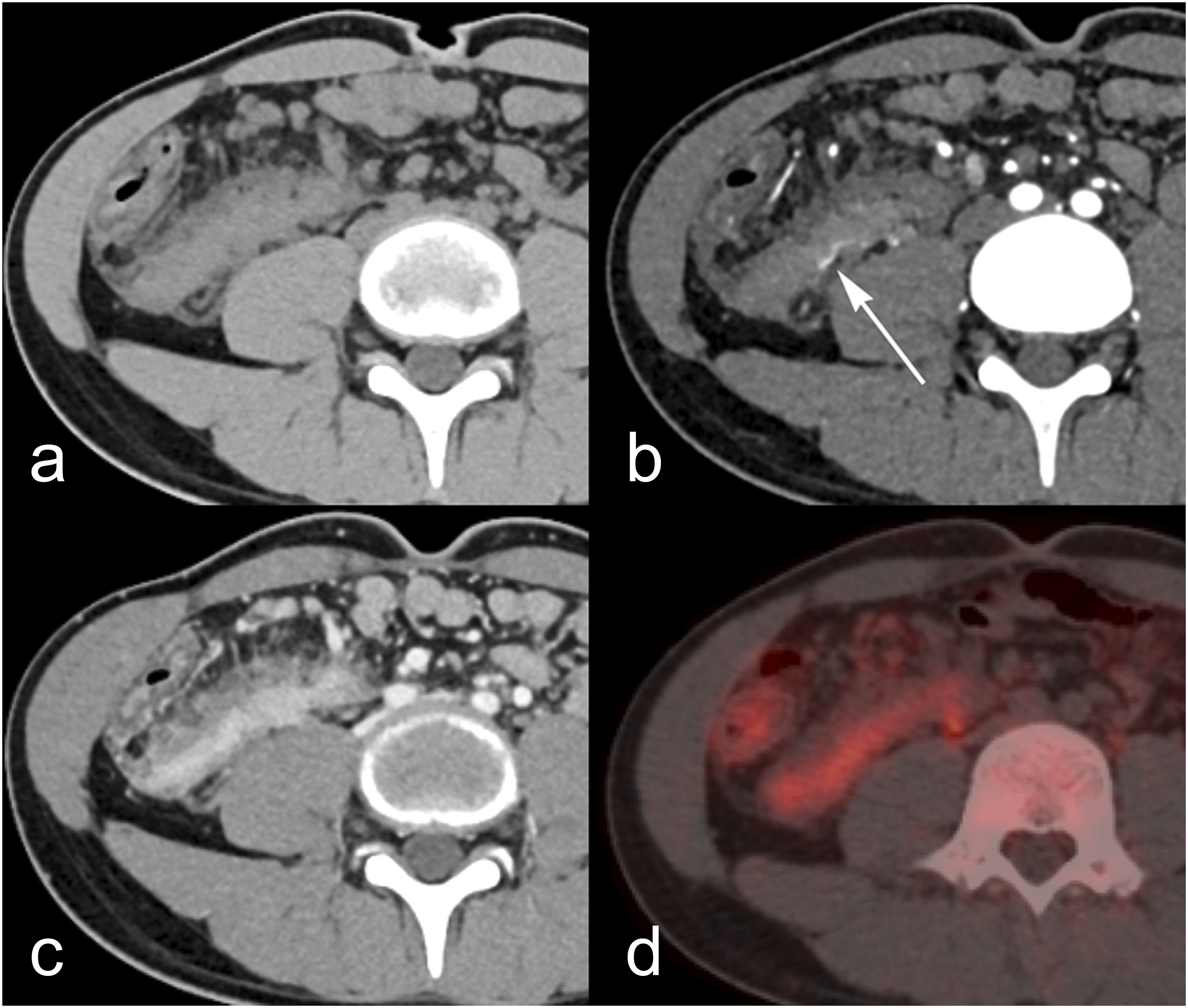

Based on the clinical presentation, we suspected that the retroperitoneal mass was a pseudotumor caused by Schistosoma. However, based on the imaging findings, the differential diagnoses included other retroperitoneal tumors such as schwannoma and lymphoma. Therefore, we performed percutaneous biopsy of the mass under guidance by C-arm cone-beam computed tomography (CBCT; Allura Clarity FD 20, Philips Healthcare, Best, The Netherlands). We used a CBCT system with a flat-panel detector and a coaxial cutting needle. The patient was positioned in the semiprone position and we used a 17-gauge coaxial introducer to access the target mass (Fig 3(a)). After the introducer had been successfully positioned at the proximal margin of the lesion, a semiautomated biopsy needle was inserted into the mass via the introducer. Each position was confirmed by CT (Figs 3(b) to (d)). Five histologic samples were collected using an 18-gauge core needle (STARCUT® aspiration-type, TSK Laboratory, Tochigi, Japan), by adjusting the angulation and rotation of the introducer toward each part of the mass. No complications were observed on unenhanced CT obtained immediately post biopsy. Cone-beam CT with the patient in the semiprone position. (a) The mass is seen in the right retroperitoneal space. (b) The introducer is placed close to the mass and passes above the iliac crest. (c) and (d) confirms the position of the biopsy needle inside the mass.
Histopathological examination of the five biopsy specimens after hematoxylin and eosin staining revealed multiple ovoid lesions surrounded by eosinophilic and lymphocytic infiltration (Fig 4(a)). The lesions were acid fast in Ziehl–Neelsen staining, with the appearance of S. japonicum eggs (Fig 4(b)). Histopathological examination. (a) Hematoxylin and eosin staining demonstrates an ovoid lesion surrounded by eosinophilic and lymphocytic infiltration. (b) The lesion is acid fast in Ziehl–Neelsen staining, suggesting Schistosoma japonicum eggs.
Discussion
This rare case of retroperitoneal pseudotumor caused by S. japonicum was diagnosed by CBCT-guided percutaneous biopsy.
Schistosomiasis is one of the most widespread parasitic infections globally, and is an important public health problem in such as the Middle East, South East Asia, Africa, and the Caribbean. 1 Three schistosome species, S. japonicum, S. mansoni, and S. hematobium, are of major importance for humans. Infection with these parasites follows direct skin contact with fresh water that contains free-swimming larval forms known as cercariae. The larvae usually live in the lumen of the intestines; however, eggs in the mesenteric veins are carried to the liver via the portal vein where they cause a granulomatous reaction in the periportal tissue. In the long term, they cause periportal fibrosis and portal hypertension.2,3 Although it can be difficult to differentiate viable from nonviable eggs, detection of eggs in extra-intestinal regions is important in deciding the treatment plan.
Multimodality imaging findings of retroperitoneal schistosomal pseudotumor have not been previously described in the literature. As our case showed a calcified lesion in the ascending colon wall, it appeared that the adult worms had migrated directly toward the right retroperitoneal space and laid eggs that caused eosinophilic and lymphocytic infiltration. We think that the infiltrative margin and homogenous late enhancement of the mass indicates its pathologically inflammatory and fibrotic nature. 4 The slight hyperintensity on T2 and diffusion-weighted MR images suggested granulomatous tissue. FDG hypermetabolism was considered to indicate active inflammation. However, it was difficult to differentiate the mass from other retroperitoneal tumors because there are so few reports of the relationship between FDG-PET uptake and schistosomiasis.5,6 Marín-Martínez et al. recently documented the case of a pseudotumoral form of retroperitoneal schistosomiasis that was similar to ours, although their case was probably caused by Schistosoma mansoni. 7 Due to its rarity, schistosomal pseudotumor is difficult to diagnose by imaging findings, and so we performed percutaneous biopsy.
Although CBCT-guided biopsy provides more patient effective dose than CT-guided biopsy, we performed CBCT-guided biopsy for several reasons. 8 First, at biopsy, we can easily detect bleeding during CBCT using a flat panel detector and perform arterial embolization immediately. Dynamic contrast-enhanced CT of our case showed a mesenteric artery running within the mass and lumbar arteries close to the puncture route, which posed bleeding risks during the procedure. Second, the tumor was difficult to delineate on ultrasonography because it was deeply located in the retroperitoneal space and there was interfering intestinal gas. Because we expected histologic features such as inflammation, fibrosis, and schistosomal eggs, we attempted to obtain samples from different locations within the mass. To improve the egg detection rate, we chose a coaxial system with an 18G introducer.
Conclusion
Schistosomal pseudotumors may occur in the retroperitoneal space and it is clinically valuable to obtain the diagnosis by percutaneous biopsy. The CBCT-guided coaxial biopsy system is a safe and accurate diagnostic procedure for investigation of these retroperitoneal tumors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient’s parents for publication of this case report.