
Abstract
Lumbar spinal stenosis is one of the most commonly diagnosed pathological conditions of the spine. Patients with lumbar spinal stenosis can be symptomatic or asymptomatic. Regardless of the clinical presentation, a combination of radiological imaging modalities including magnetic resonance imaging, CT, and dynamic X-rays can be used to evaluate the severity. An often underrecognized aspect of severe lumbar spinal stenosis is its effect on nerve roots. We propose coining the term “GatorSign” to describe nerve root edema above the area of severe central canal stenosis. This radiological finding can help identify patients with severe central canal stenosis in patients who would likely be neurologically symptomatic, requiring an invasive intervention such as epidural injections or surgical decompression for relief as conservative treatments such as physical therapy and/or medications are less likely to be effective.
Introduction
Lumbar spinal stenosis is a degenerative spinal condition affecting nearly 50% of the population with low back pain. 1 Often, patients report symptoms that are substantiated with clinical examination and imaging modalities, including magnetic resonance imaging (MRI), CT scan, and dynamic X-rays. Lumbar spinal canal stenosis indicates a decrease in the available space (narrowing) inside the spinal canal, lateral recess, and/or neuroforamina. These can be present at single or multiple levels in the lumbar spine. The reason for the narrowing could be (a) anterior column culprits, including bulging, degenerated, or herniated discs, and posterior longitudinal ligament hypertrophy; (b) central canal culprits, including epidural lipomatosis, epidural fibrosis, or scarring from previous surgery, facet cysts, or ligamentum flavum cysts pushing into the central canal, or congenitally short pedicles; and (c) contribution of posterior elements to stenosis, which could come from bone spurs or facet overgrowth/degeneration, as well as hypertrophy and/or infolding of the ligamentum flavum.2,3 Hypertrophy of posterior elements could lead to degenerative spondylolisthesis and/or instability of the lumbar spine, which is best assessed by CT and dynamic X-rays. MRI is usually the best imaging modality to assess the severity of stenosis and the contribution of anatomical structures to the narrowing.
There is not always a good correlation between radiological findings and clinical presentation, and the severity of narrowing on imaging does not predict the clinical severity of stenosis and the degree of neurogenic claudication. 4 Usually, such patients are managed conservatively in the beginning with physical therapy, a home exercise regimen, and medications such as gabapentin, pregabalin, and nonsteroidal anti-inflammatories. Invasive treatment such as injections or surgery is considered only when such conservative treatments are not effective. However, in our clinical experience there is a subset of patients suffering from severe lumbar spinal stenosis who have unique findings on MRI, and they usually do not respond to conservative treatments.
In this article, we propose coining the term “GatorSign” as a radiological finding evident in some cases of severe lumbar central canal stenosis. This is defined as more than a 50% reduction in the area of the spinal canal, resulting in edema surrounding the nerve roots just above the level of maximum stenosis (narrowing) that is seen on sagittal and axial sections on T2-weighted images, as well as on short T1 inversion recovery sequence. This radiological feature can be used to accurately describe severe lumbar central canal stenosis and prognosticate the likely need for invasive treatment approaches. Our clinical experience has been that a patient with GatorSign is almost always symptomatic with neurogenic claudication and does not respond to conservative treatment approaches such as physical therapy or medications. We have seen patients with mild to moderate stenosis progress from having no GatorSign to developing severe stenosis, that is, demonstrating GatorSign. In such patients, earlier conservative treatment measures slowly lose efficacy, coinciding with the appearance of GatorSign. The patients included in this case series provided verbal consent for their cases to be described in this report and all images have been deidentified.
Case history
Case 1
An 80-year-old man with a history of progressively worsening chronic low back pain for more than a decade presented to us for an evaluation. Both clinical examination and radiological findings were consistent with severe lumbar spinal stenosis, resulting in neurogenic claudication. The patient described his leg pain as a cramping, tingling/pins and needles, and stabbing sensation that was constant as soon as he stood up. His symptoms had gradually worsened in intensity. He rated the pain as 10/10 at its worst with an average pain score of 3/10. No motor weakness was found, but he had decreased sensation to light touch and pin prick in both lower extremities across all dermatomes. He denied any bowel or bladder symptoms resembling cauda equina syndrome.
He initially underwent conservative management with opioid-free pharmacotherapy including duloxetine, gabapentin, medical marijuana, and acetaminophen. He also exhausted physical therapy for over 1.5 years in the early course of his disease; weekly isotonic and isometric home stretching exercises did not provide relief. The patient underwent several injection procedures to alleviate his back pain, including caudal epidural steroid injections and transforaminal epidural steroid injections.
Lumbar spine MRI showed severe stenosis of his spine at multiple levels from L1–L2 to L5–S1 (Figure 1(a)–(f)). The patient was evaluated by the neurosurgery team and found to be nonoperative. He consulted our team, and a plan was made for a unilateral two-level lumbar endoscopic laminotomy for bilateral decompression at L3-L4 and L4-L5, which were the worst levels of his lumbar spinal stenosis. Axial (a, c, e) and sagittal (b, d, f) views of T2-weighted magnetic resonance images of the lumbar spine for a 80-year-old patient demonstrating perineural edema, that is, GatorSign, above and below the sites of maximal canal stenosis. (b) The white arrow indicates the site of maximal stenosis with the correlating axial view in (a). Perineural edema, GatorSign, is shown by the white arrows in (c) and (d) above the site of maximal stenosis, as well as below the site of maximal stenosis in (e) and (f).
Case 2
A 61-year-old woman presented to us 6 years ago for lower back pain radiating to her legs. She had a history of L4-S1 traditional laminectomy and posterior decompression combined with instrumented fusion in 2007. She suffered from adjacent segment disease at L3-L4 with moderate stenosis at that segment evident on MRI in 2016. Her symptoms of lower back pain radiating down both lower extremities were not controlled with physical therapy and medications such as gabapentin. Her pain was managed well for almost 6 years with regular transforaminal epidural steroid injections at the L3-L4 level spaced every 4–5 months until the injections stopped being effective and her symptoms worsened. A recent MRI showed severe central canal stenosis at L3-L4 with perineural edema (GatorSign) just above the site of maximal stenosis, as well as dynamic instability of L3-L4 on flexion extension X-rays (Figure 2(a)–(h)). The patient was referred to her neurosurgeon, who scheduled her for decompression at the L3-L4 segment, along with an extension of her fusion to L3. Axial (a, c, e, g) and sagittal (b, d, f, h) views of a T2-weighted magnetic resonance imaging of a 61-year-old woman with severe lumbar stenosis demonstrating GatorSign. (a) An axial view of the site of maximal compression in the setting of severe spinal canal stenosis (white arrows). (b) The correlating sagittal view with white arrows indicating the site of maximal compression. (c) The axial view of the region just proximal to the site of maximal compression with the beginning of T2 signal change, with the correlating short T1 inversion recovery image in (d). (e) An axial view slightly above the site of maximal compression demonstrating perineural edema (white arrows), that is, GatorSign, with the correlating sagittal view in (f). (g) An axial view of perineural edema (GatorSign), with the correlating short T1 inversion recovery sequence image in (h).
Case 3
A 49-year-old man with a history of multiple injuries related to playing professional ice hockey was referred for management of progressively worsening lower back pain along with neurogenic claudication. Standing for a few seconds was challenging before cramping in his legs began. He went through multiple rounds of physical therapy and epidural steroid injections over the years, which ceased to be effective about 2 years ago. MRI of his lumbar spine revealed severe central canal stenosis at L3-L4 with moderate central canal stenosis at L4-L5 (Figure 3(a)–(d)). He underwent lumbar endoscopic unilateral laminotomy for bilateral decompression of L3-L4 and L4-L5 stenotic segments and reported almost immediate improvement in his ability to stand and walk. He reported full recovery at his 3-month follow-up visit. Axial (a, c) and sagittal (b, d) views of T2-weighted magnetic resonance images of the spine of a 49-year-old patient demonstrating perineural edema, with GatorSign observed above the sites of maximal canal stenosis at L3-L4. (a) An axial view of the site of maximal compression with a corresponding sagittal view in (b). (c) An axial cut just above the site of maximal compression with GatorSign. (d) The corresponding sagittal view.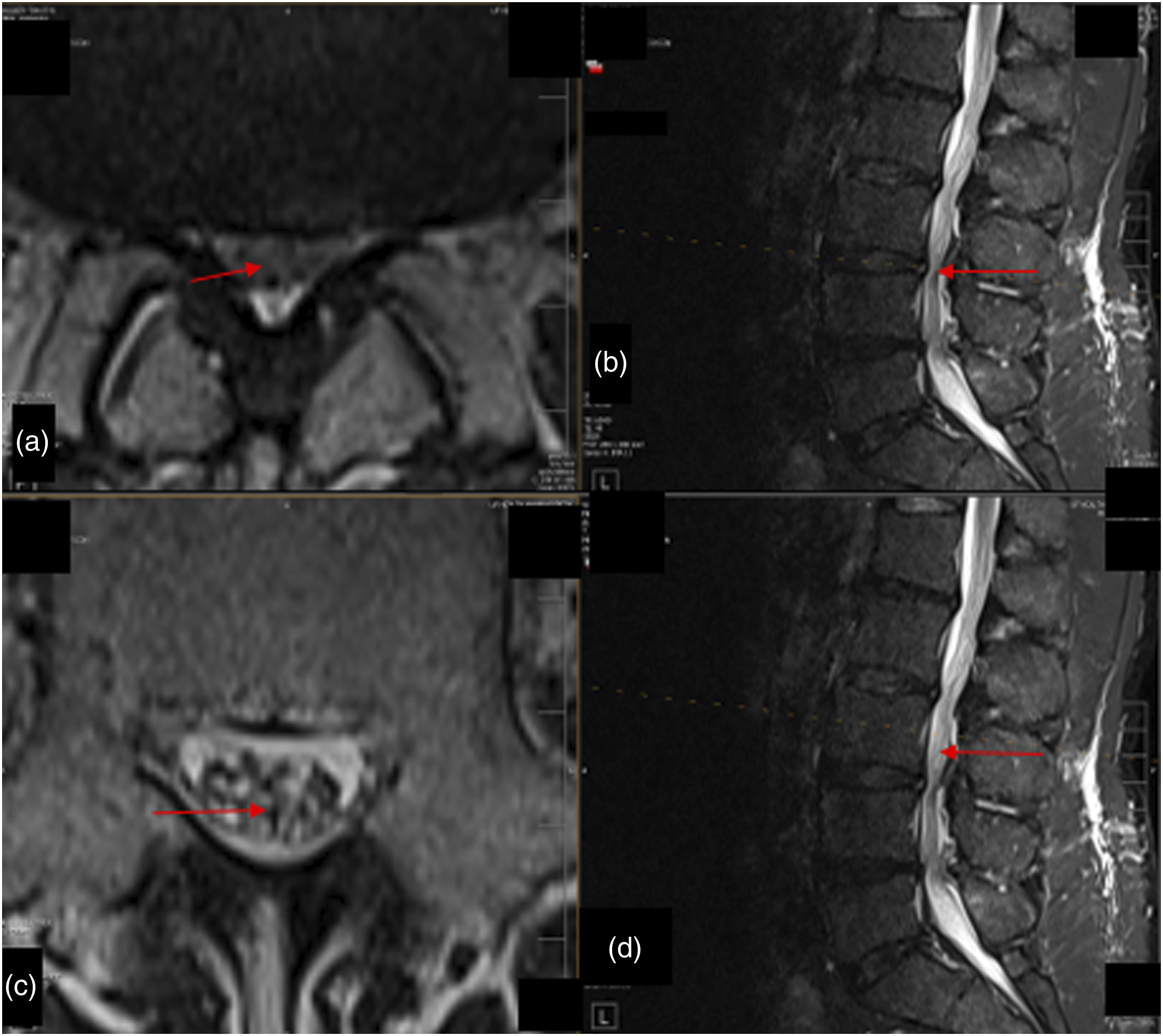
Case 4
A 72-year-old man was suffering from chronic lower back pain and lower extremity numbness and weakness, as well as gait and balance abnormality due to a lack of sensation in his feet/toes. He was able to ambulate only by using a walker. His neurologist diagnosed him with idiopathic peripheral neuropathy. MRI of his lumbar spine showed multilevel degenerative stenosis with severe central canal stenosis at L4-L5 and L3-L4, along with moderate stenosis at L2-L3 (Figure 4(a)–(h)). He was also diagnosed with mitochondrial myopathy and was evaluated by neurosurgery for possible decompressive surgery, but surgery was deemed a poor option because of the possibility that mitochondrial myopathy was contributing to his weakness. Upon evaluation by the interventional pain team, perineural edema was discovered above the site of maximal stenosis at both L4-L5 and L3-L4: GatorSign. He underwent lumbar endoscopic unilateral laminotomy for bilateral decompression of the L3-L4 and L4-L5 stenotic segments. The patient recovered all sensation in his legs below the knees and reported 100% improvement in his chronic lower back and radicular pain, as well as neurogenic claudication. He no longer needed a walker or cane to ambulate, and he was able to walk for long distances and swim several laps in the pool after many years. Prior to surgery, he was wrongly diagnosed with idiopathic peripheral neuropathy causing gait and balance problems, which resolved after his decompressive surgery. His MRI 3 weeks after decompressive surgery showed an expanded spinal canal with a decrease in perineural edema around the nerve roots. Axial (a, c, e, g) and sagittal (b, d, f, h) views of T2 and short T1 inversion recovery sequence magnetic resonance images of the spine for a 72-year-old patient demonstrating perineural edema, with observed GatorSign above the sites of maximal canal stenosis. (a) An axial view of the site of maximal compression with a corresponding sagittal view in (b). (c–f) The cord areas above and below the sites of maximal compression, (c, d) and (e, f), respectively. (g, h) Images after endoscopic surgical decompression of the central canal at the L4–L5 and L3–L4 levels. (g) A re-expanded central canal at L4-L5 with reduced edema surrounding the nerve roots in comparison to (e), which is a corresponding view at the same level (L4-L5) prior to surgery.
Case 5
A 74-year-old woman was suffering from weakness and numbness in both legs, with her left leg worse than her right. She presented to the interventional pain clinic due to increased pain in her back and legs from multiple falls due to her weak legs “giving out.” Her condition worsened despite 3 months of physical therapy and epidural injections for at least 3 months. MRI of her lumbar spine showed severe central canal stenosis at L4-L5 with GatorSign just above the site of maximal compression (Figure 5(a)–(f)). She underwent lumbar endoscopic unilateral laminotomy for bilateral decompression with remarkable recovery of her lower extremity strength and resolution of numbness in her lower extremities. Axial (a, c) and sagittal (b, d) views of T2-weighted magnetic resonance images of the spine for a 74-year-old patient demonstrating perineural edema, with GatorSign observed above the sites of maximal canal stenosis at L4-L5. (a) An axial view of the site of maximal compression with a corresponding sagittal view in (b). (c) An axial cut just below the site of maximal compression with GatorSign and the corresponding sagittal image in (d). (e) The axial cut just above the site of maximal compression with GatorSign and the corresponding sagittal image in (f).
Discussion
This case series demonstrates a unique and underrecognized radiological sign that can help to accurately diagnose and prognosticate treatment of severe lumbar spinal stenosis. To our knowledge, this is the first article describing such radiological findings and officially coining the term GatorSign. This term describes a pathological finding of nerve root edema just above and sometimes just below a region of lumbar central canal stenosis. An illustration of this concept can be seen in Figures 6 and 7. Illustration of GatorSign with compression of the spinal nerve roots in the sagittal view (b) and coronal view (d). (a) The sagittal view of normal anatomy of vertebral bodies with intervertebral discs and a spinal cord with trailing cauda equina. (b) A pathological variant with a large central/posterolateral herniation from the intervertebral discs impinging on the spinal canal, indicating the likely location of maximum compression and edema surrounding the lumbar nerve roots (GatorSign) just proximal and/or distal. (c) A posterior view of the spinal canal with normal anatomy. (d) A pathological central herniation of the intervertebral disc compressing the traversing nerve roots, which would cause perineural edema (GatorSign) just proximal and/or distal. Illustration of GatorSign resulting from compression of the spinal nerve roots (b). (a) The axial view of normal anatomy of an intervertebral disc with a normally appearing spinal canal, facets, and ligamentum flavum. (b) A pathological variant with a large central/paracentral herniation through the annulus of the intervertebral disc with hypertrophied ligamentum flavum, as well as hypertrophied and arthritis facet joints causing the classic trifecta compression of the spinal canal. This would result in edema just above and below the level of maximal compression, that is, GatorSign.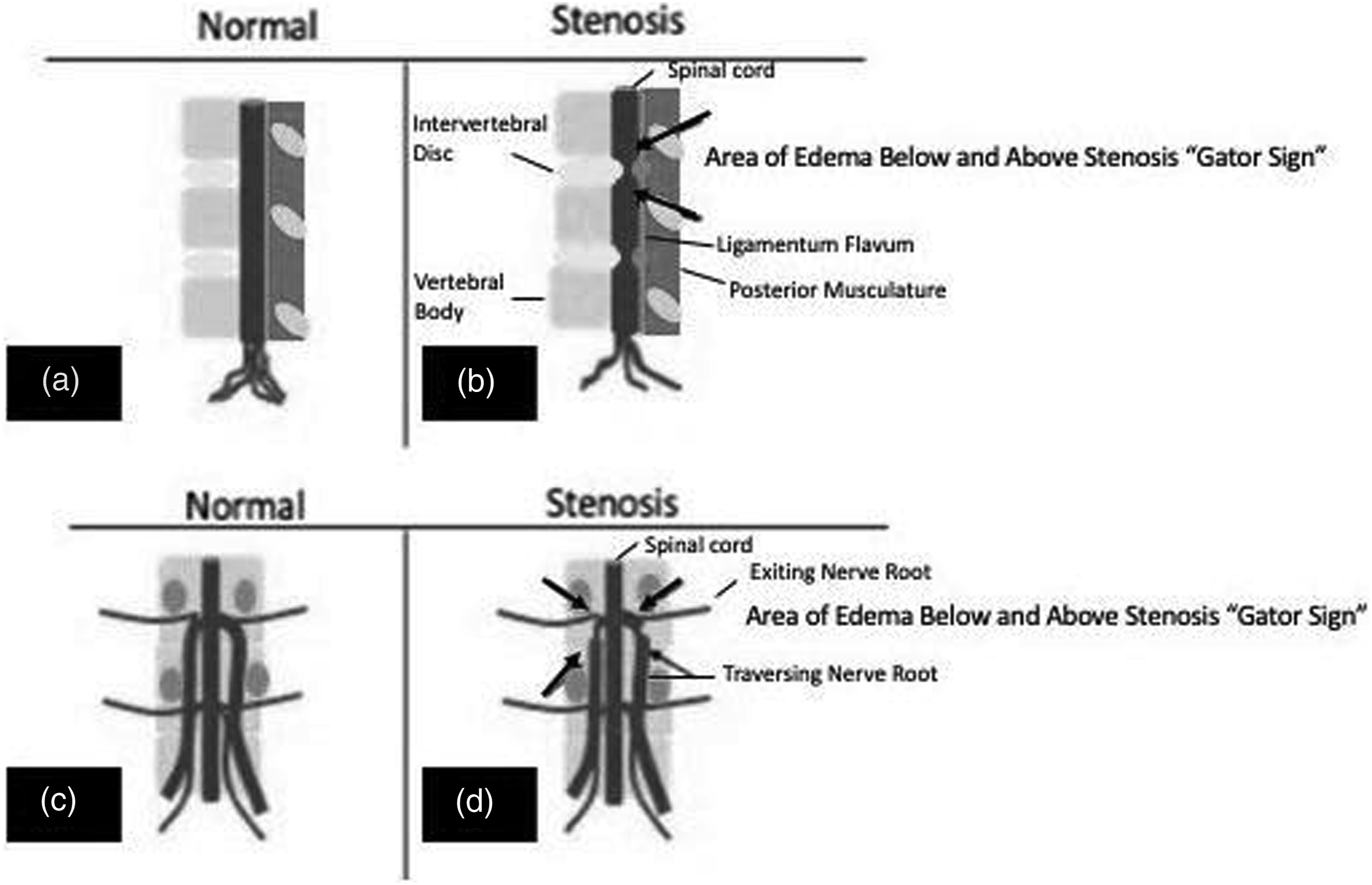

Essentially, compression of the spinal nerve roots results in inflammatory changes, including edema, starting at the region of compression or stenosis and intensifying mainly proximal and sometimes distal to the compression site. This can be likened to ligating a digit or extremity with obstruction of venous and lymphatic channels causing swelling of the digit or extremity. Spinal stenosis can cause radiculopathy via venous obstruction of radicular veins with consequent dilation of the veins and compression of nearby nerve roots. 5 Figure 7(b) shows other posterior components such as facet arthropathy or thickened ligamentum flavum that can affect both the exiting and traversing nerve roots. This would likely result in reactive inflammatory nerve root edema and/or nerve root enhancement, that is, GatorSign. The trifecta of a herniated/bulging disc, as well as hypertrophied facet joints with thick ligamentum flavum can obstruct veins in the central canal or the neuroforamen, resulting in decreased venous return from the spinal parenchyma. 5 This can cause venous congestion of the spinal nerve roots in the central canal, as well as the neuroforamen because the vertebral veins are valveless. This congestion causes increased venous pressure and subsequent vasodilation of intramedullary arteries, resulting in increased pressure in the tissues, intramedullary edema, decreased perfusion pressure, and ischemic injury. 5 For this phenomenon to occur, stenosis must be graded as severe with at least a 50% decrease in central canal volume. Generally, in patients such as ours, the degree of compression is enough to manifest as symptoms of neurogenic claudication.
Perineural edema typically develops above but also sometimes below the site of maximal compression in the spinal canal. Short T1 inversion recovery images are useful to detect edema because they obviate the signal from fat. Thus, the high-intensity signal is fluid, which is likely due to edema. Short T1 inversion recovery sagittal images are seen in Figure 2(d) and (h). Figure 2(g) emphasizes the perineural edema changes. Other radiological findings that are observed in Figure 2(a), (c), (e), and (g) include a narrowing of the canal circumferentially, thereby reducing the effective circulatory volume of the central canal. Additional findings include an engorged and tortuous appearance of the nerve roots, described as redundant nerve roots in the setting of severe lumbar spinal stenosis (Figure 2(b), (f), (d), (h)). In a T2-weighted image, the bright regions correlate to higher proton excitation, which can be explained by perineural edema. 6 Comparatively, in a T1-weighted image, the darker regions correlate to a higher proton density, likely edema. 6 In these MRIs, the presence of GatorSign offers a quick assessment of the severity of the canal stenosis and usually prognosticates the effectiveness of treatment options. In our experience, clinical symptoms are unlikely to respond to conservative management and for neurogenic claudication to improve, invasive treatment methods such as epidural injections or decompressive surgery is indicated.
Conclusion
Understanding the radiological evidence of lumbar spinal stenosis is fundamental to making an accurate diagnosis. Through several case studies, this paper proposes a new radiological sign, GatorSign, that is indicative of severe lumbar spinal stenosis. This sign describes nerve root edema possible above and below an area of maximal stenosis. These radiological changes are most notable on short T1 inversion STI MRIs, which accentuate edema and obviate signal from fat. Patients with a positive sign and clinical symptoms do not typically respond to conservative management such as pharmacotherapy, physical therapy, or a home exercise program. In the several cases discussed, correct identification of GatorSign with endoscopic surgical decompression significantly relieved patient complaints of neuroclaudication and in some instances eliminated the need to use ambulatory devices; all cases resulted in an improved quality of life after an endoscopic surgical intervention by the interventional pain team.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.