
Abstract
Background
Systemic air embolism is a rare, however potentially fatal, low incidence, complication to CT-guided transthoracic needle biopsy of lung lesions.
Purpose
The purpose of this review of case reports and series was to pool data about this rare complication and glance for a pattern or similarities in the patients’ initial symptoms and course, as well as the management of the patients in relation to current guidelines.
Material and methods
PubMed was searched for case reports and case series about systemic air embolisms following CT-guided transthoracic needle biopsy of lung lesions from inception to November 2021. A reviewer screened the results for eligibility and included studies which reported at least two outcomes of interest. Data was extracted by one author and a descriptive analysis was conducted.
Results
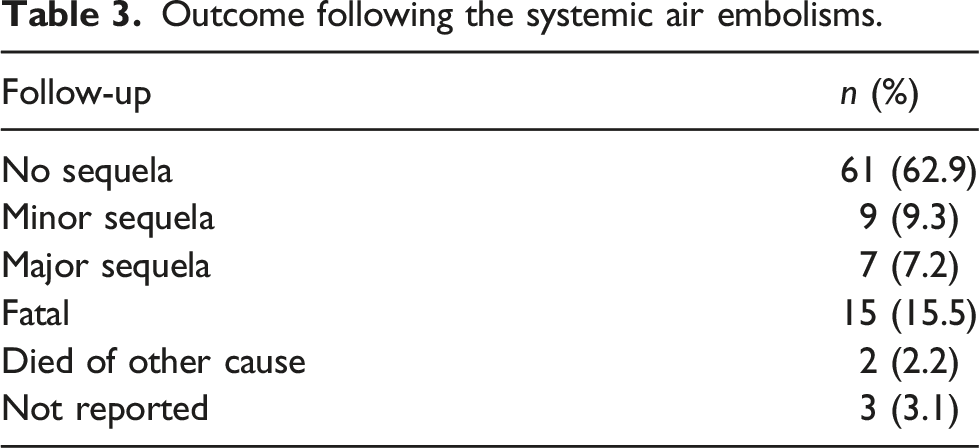
Of 1,136 studies screened, 83 were eligible for inclusion involving 97 patients. The mean age was 64.8±11.7 years and ≈60% of the patients were men. In 15 cases the outcome was fatal, and most of the fatal cases (n = 12) had cardiac arrest as the primary initial symptom. In addition to conventional oxygen therapy, 34 patients received hyperbaric oxygen therapy, and in 30 cases the physician in charge chose to change the patient from standard supine position to – most often – Trendelenburg position.
Conclusion
No similarities were found that could lead to more rapid diagnosis or more correct management. The staff should keep systemic air embolisms in mind, when more common complications are ruled out, and consider hyperbaric oxygen therapy in case of suspicion.
Introduction
Computed Tomography (CT)–guided transthoracic needle biopsy (CT-TTNB) plays a major role in the diagnostic workup of lung lesions. It is today widely accepted and commonly used – especially for peripheral lung lesions where endobronchial procedures are not possible.1,2
The increased use of scanning modalities and screening programs for pulmonary cancer will most likely lead to an increased number of transthoracic as well as endobronchial lung biopsies, and as a result an increased number of complications. The most common complications after CT-TTNB are pneumothorax, parenchymal bleeding and haemoptysis.1,3 Systematic reviews and meta-analyses report an overall risk for complications using fine needle biopsy of 24.0% and for core needle biopsy 38.8% – depending on risk factors which include chronic obstructive pulmonary disease (COPD), long needle path with fissure crossing, needle size and smaller lesion.1,3
Systemic air embolism is another complication to CT-TTNB. Because of the potential severity and in some cases fatal outcome, systemic air embolisms remain a topic of interest. The challenge is that systemic air embolisms after CT-TTNB are extremely rare, and the symptoms vary from completely asymptomatic to acute fatal with cardiac arrest as the first symptom.4,5 Studies have systematically and for research purposes performed thoracic CT scans after CT-TTNB to identify systemic air embolisms and the literature report an incidence of approximately 0.08%–4.8%.5,6 Risk factors for systemic air embolisms are described as cough during the procedure and high-pressure ventilation. The prospective and retrospective cohorts, gathered in systematic reviews and meta-analyses, aim to explore incidences and causal relationships (risk factors) of systemic air embolisms as described, but rarely focus on occurrence of rare events and how they are clinically handled.
The aim of this study was to glance for a pattern or similarities in the published patient histories and to describe the patients’ symptoms immediately after CT-TTNB in order to correlate the symptoms to the location of the air embolism and describe the management of the patients according to guidelines. Hence, a strategy was chosen in which case reports and case series were included in order to pool the rare events.
Methods and material
The systematic search was prepared in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines although the study design does not fulfil all criteria for a systematic review. 7
Research question and PICO model for search preparation.
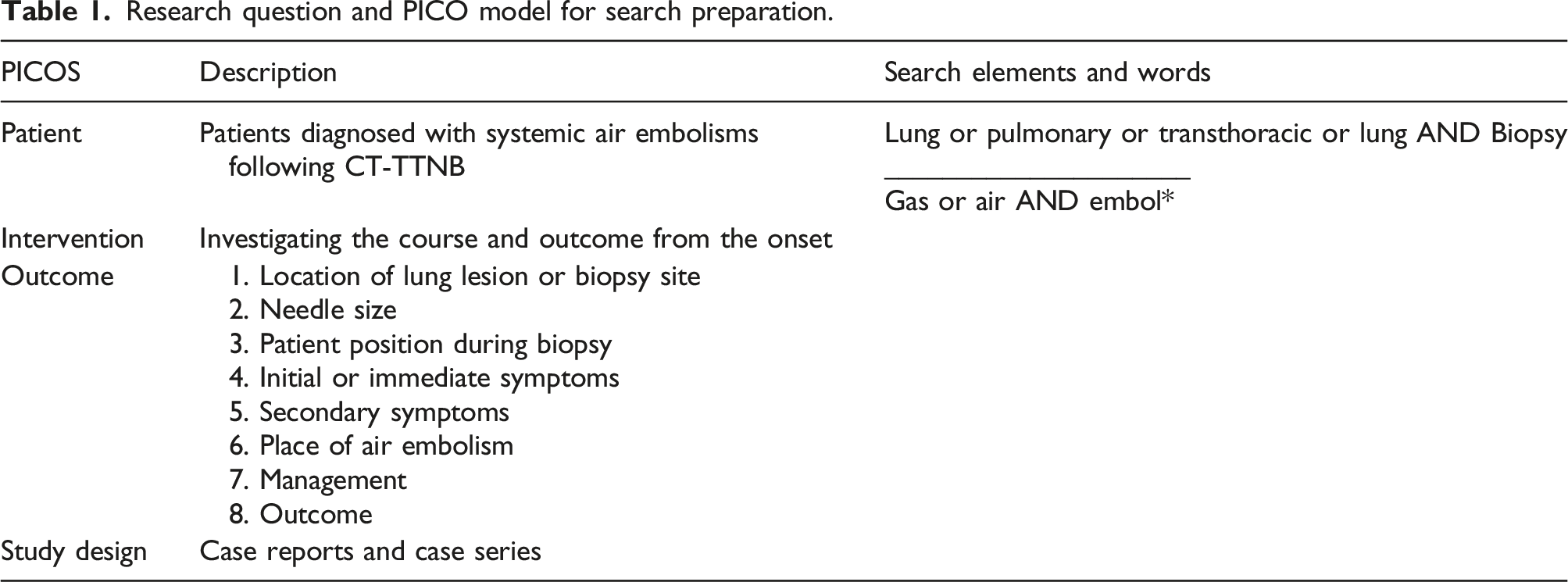
Prospective and retrospective cohorts, with their respective advantages and disadvantages, aim to explore incidences and causal relationships (risk factors). We only chose to include case reports and case series because we wanted to pool the events and glance for a pattern in the initial symptoms as well as explore the management of the patients after the diagnosis of systemic air embolisms.
Search strategy
The search was built on the central elements of the research question, see Table 1, and developed for Medline. Both controlled vocabulary and, for example, MeSH terms, free text and key words were applied. The final search was done in OVID Medline in October 2021.
No filters were used (e.g. publication dates or language). Records were managed using the reference tool Endnote X9 (Clarivate Analytics, Philadelphia, US). First, title and abstract of the results were screened and subsequently full-text reading.
Eligibility criteria
Criteria for inclusion were defined as follows: 1. Case reports or case series about systemic air embolisms following CT-guided transthoracic needle biopsy of lung lesions. 2. At least two outcome measures, defined in Table 1, with at least one of them being initial symptoms or management of the patient.
Criterion for exclusion was: 1. Full text not available.
Data management and synthesis
Extraction of data was done by second author (BK) and verified by first author (PP). The data was handled in a prefabricated data extraction template in Microsoft Excel, version 16.52 (Microsoft Corp, Washington, US). All analyses and syntheses performed using Stata 16.0 (StataCorp LLC, Texas, US).
Due to the wide aim of the research question and outcome measures, simple descriptive statistics were done on publication characteristics, patient demographic and procedure information. Case reports were then grouped by asymptomatic, incidental systemic air embolisms and acute, severe systemic air embolisms.
Results
Search
The search was conducted in December 2020 and updated in November 2021 revealing a total of 1,136 records. After screening first by title and abstract, subsequently for full text, a total of 83 studies were identified including 97 patients, (Fig. 1). A detailed list of included case reports and case series is provided as Supplementary 1. PRISMA flowchart of study selection and eligibility.
Patient- and procedure-related information
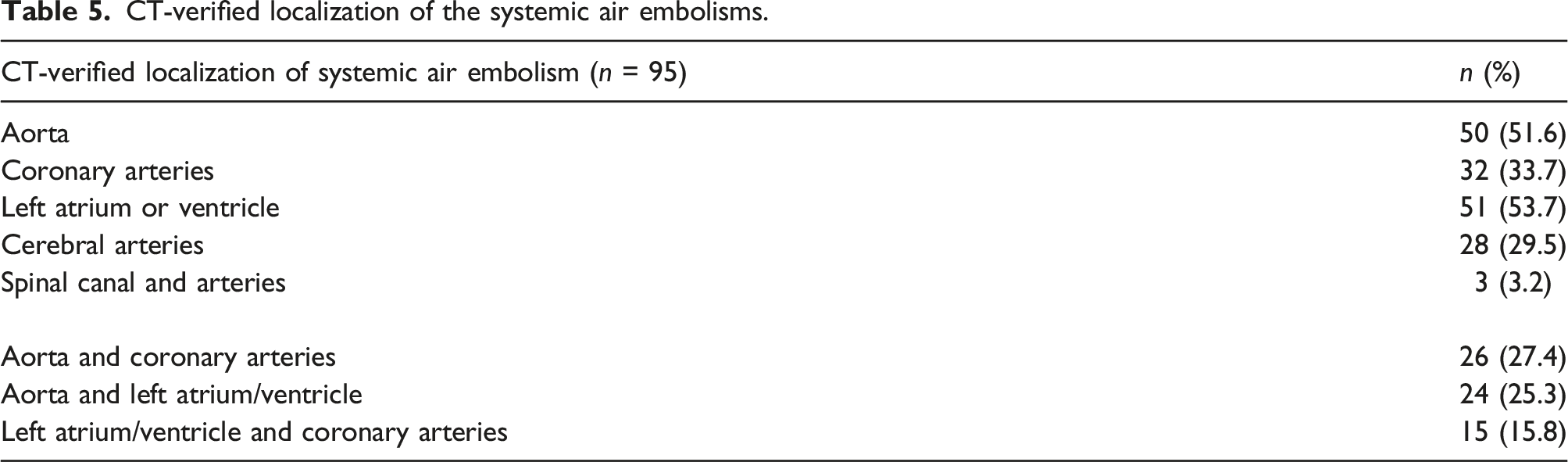
The mean age of the patients suspected of having a systemic air embolism was 64.8 ± 11.7 years (described in 95 cases of the 97 patients) and most of the patients were men n = 58, 59.8% (described in 94 of 97 cases). In one case, the systemic air embolism was not CT-verified, but the clinical suspicion overruled the negative control CT scan and thereby the diagnosis was established based on the symptoms. 8 In another case, the air embolism was described in the right ventricle and in the thoracic veins. 9
Patient and procedure characteristics.

Symptoms and outcome
Outcome following the systemic air embolisms.
Symptoms and treatment.

CT-verified localization of the systemic air embolisms.
Management and treatments of the patients
In all cases where the patient suffered from cardiac arrest, the primary management and treatment was cardiopulmonary resuscitation, including intubation and in some cases admission to the intensive care unit (ICU). The most frequent reported management and treatment for the patients who did not suffer from immediate cardiac arrest was oxygen therapy – in patients not receiving cardiopulmonary resuscitation or intubation a total of 46 patients received oxygen therapy (sixteen patients received oxygen therapy solely). Thirty-four patients received hyperbaric oxygen therapy (HBOT) (n = 34) and 30 cases reported change in patient position to other than conventional supine emergency management (n = 30) as a treatment modality. In most cases, the change was to Trendelenburg position. One handled the patient with keeping the patient in the prone position (as during the biopsy) and add Trendelenburg position after CT-verification of the systemic air embolism. 11 In this case, the patient was also diagnosed with patent oval foramen which caused air in both the venous and arterial system. Two cases describe that the patients were placed in the lateral decubitus position; one on the left side including Trendelenburg after CT-verified air in the left ventricle, 18 and one on the right side including Trendelenburg after CT-verified air also in the left ventricle. 19
Hyperbaric oxygen therapy was described in 34 case reports, either as treatment alone (n = 9 cases) or in combination with other treatments depending on the symptoms of the patients (n = 25 cases).
Of other treatment modalities that are described are therapeutic hypothermia20,21 and cardiac catheterization, 22 see supplementary 2 for overview of treatment strategies for each specific case.
Discussion
We aimed to provide a review of case reports and case series on systemic air embolisms following CT-TTNB of lung lesions to explore potential similarities and patterns in the cases published with focus on initial symptoms and management of the patients. We identified 97 cases with systemic air embolism following CT-TTNB, but we did not find significant patterns or similarities in the included case reports or case series that could indicate how to handle initial symptoms or management of the patients.
Theoretically, there are two possible aetiologies for air to enter the pulmonary vein system during a CT-TTNB of a lung lesion. First, air may enter directly from the needle lumen to the pulmonary vein system. In this case, the tip of the needle is accidentally placed directly in the pulmonary vein and when the stylet is removed the atmospheric pressure exceeds the pulmonary vein pressure. 23 This risk is described as even greater if the patient takes a deep breath and thereby increases the difference in intra- versus extra-thoracic pressure. Secondly, air may enter if the needle ruptures alveoli and thereby creates a connection between the alveoli and the pulmonary veins. Increased pressure could then promote air embolisms, for example, if the patients cough, if the patients suffer from severe COPD or air trapping. These theoretical causes have been presented repeatedly but cases keep being published even though the patients are not coughing, are not under positive pressure ventilation, etc. 24
Several studies have been published investigating the incidence and risk factors for systemic air embolisms. A meta-analysis from 2021 reports a pooled incidence of 0.08% (95% CI 0.048–0.128%, I2 = 45%) for symptomatic air embolisms following transthoracic needle biopsy of lung lesions. 5 The meta-analysis suffers from a small population size (n = 123) and significant heterogeneity among the studies included. Several larger retrospective studies confirm this finding.25-27 However, some studies report the incidence slightly higher. Freund et al. report an incidence of 3.8% in a retrospective study of 610 patients, with a clinically apparent incidence of 0.49%, 28 and Monnin-Bares et al. report an incidence of 4.8% with clinical incidence of 0.17%. 6 In the latter, 27 cases of CT-verified systemic air embolism were found among the 559 patients with one patient having symptoms corresponding to the finding. Thereby, results could indicate that the incidence was significantly higher in studies doing routine CT scans after the biopsy procedure. However, since systemic air embolisms are detected in the cerebral arteries and the studies include control CT scan of the thorax, this could be a limitation. Because of the very low incidence, and potentially asymptomatic presentation, large studies requiring control CT scans after the biopsy are needed to explore the true incidence. This setup has limitations that would lead to additional radiation exposure and multiple additional CT scans. It is, however, important to debate number needed to scan to detect one systemic air embolism when most of the patients have no symptoms at all and the patients developing cardiac arrest most often suffer from this symptom immediately after the procedure. It is probably more important to create awareness of the complication than to explore the true incidence, as well as it is more beneficial to ensure that the staff are competent in cardiac resuscitation and are aware of the potential benefit of, for example, hyperbaric oxygen therapy than to avoid potential risk factors which will exclude a patient population for further diagnostic tests, for example, due to long needle path or COPD.
Larger biopsy needles, parenchymal haemorrhage, lesion in the lower lobes and prone position have been associated with and been proven as risk factors for systemic air embolisms.26,28,29 Our data is based on case reports and case series, and therefore, we cannot provide evidence on incidence or risk factors. What we can conclude is that in most of the cases with fatal outcome, the patient developed cardiac arrest immediately after the procedure. Thus, if a patient has symptoms suggesting systemic air embolisms after a CT-TTNB, and a control CT scan, for example, hours after the procedure confirm the findings, the risk of a fatale outcome is low if cardiac arrest was not among the first symptoms. The patients’ who developed cardiac arrest but had return of spontaneous circulation after successful cardiopulmonary resuscitation had no or minor sequela when discharged from hospital.
Numerous of the included case reports include a review of the literature in their presentation and discussion of their case report or case series.14,17,30-33 The reviews are scarce as they mostly consist of references within the topic of systemic air embolisms included in their discussion section, and one study compares the results of only three other studies. Only one of the studies includes a detailed review including 46 publications (case reports, case series and retrospective studies) including 77 patients. 32 A strength within the current study is the comprehensive and systematic search of case reports and case series, and we succeeded to gather and pool data from a rare complication which is difficult to investigate, and which has not previously been systematically addressed using a more conventional systematic review approach of assessing larger studies.
We acknowledge several limitations to our study. First, the study does not fulfil the criteria for a systematic review; the search was not done in three or more databases and the eligibility process was not done by two independent reviewers or assessors. However, the study was conducted according to many of the principles in the PRISMA guidelines. The level of evidence for a systematic examination of 83 case reports or case series is low. However, the study design is not intended for causation. The aim of the study was not to establish evidence on incidence, risk factors or aetiology of systematic air embolisms but to glance for a pattern or similarities in the published patient histories.
With respect to published evidence and case reports about CT-guided transthoracic needle biopsy of lung lesions, there are no clear recommendations and guidelines to avoid and handle this potentially fatal complication. To our knowledge, only one recent guideline describes systemic air embolisms following CT-TTNB. The 2020 Clinical Practical guideline for percutaneous transthoracic needle biopsy of pulmonary nodules reports: ‘When systemic air embolism occurs, we recommend supplying oxygen at as high concentration as possible, including hyperbaric oxygen therapy, and anticonvulsants, if needed’ as an A recommendation with a level of evidence at III and based on case reports. 34
Hyperbaric oxygen therapy is recommended and is described in numerous of the case reports included in this review. 34 Boyle’s law states that the size of an air bubble in liquid – in this case in the arterial system – decreases with increased surrounding pressure. Using hyperbaric oxygen therapy, the patient breathes 100% oxygen at a pressure above atmospheric pressure which theoretically decreases the size of the air embolism by raising the ambient pressure and by causing systemic hyperoxia. 35 More studies exploring systemic air embolisms advocate for supine patient position whenever possible, and supportive respiratory and cardiac treatment in acute setting. 5 This study intents to create awareness and knowledge about this rare but potentially fatal complication. To detect and diagnose systemic air embolisms, one must be aware of its existence, know the common symptoms and be able to identify the cause in a potentially acute setting.
In conclusion, no similarities or patterns in the initial symptoms were found that could potentially lead to more rapid diagnosis or more correct management. Due to sparse evidence in the field, only one guideline describes how to manage patients diagnosed with systemic air embolisms. Independent of complication type, it is important that the operator and staff in the operating rooms are ready for prompt initiation of treatment if a patient evolves neurological, cardiac or respiratory symptoms, and must keep systemic air embolisms in mind, when more common complications are ruled out.
Supplemental Material
Supplemental Material – Systemic air embolism following computed-tomography-guided transthoracic needle biopsy of lung lesion – a systematic search of case reports and case series
Supplemental Material for Systemic air embolism following computed-tomography-guided transthoracic needle biopsy of lung lesion – a systematic search of case reports and case series by Pia I Pietersen, Björg Kristjansdottir, Christian Laursen, Gitte Jørgensen and Ole Graumann in Acta Radiologica Open.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.