
Abstract
Background
Selecting the correct size of implants to be used in total knee arthroplasty is critical for a successful outcome. Marker-less templating systems use an institutionally derived magnification factor for all radiographs.
Purpose
To determine the institutional magnification of knee radiographs for patients awaiting total knee arthroplasty.
Material and Methods
Eighty patients awaiting total knee arthroplasty underwent preoperative knee radiographs using a standardized protocol. A marker attached to the patients’ knees at the level of the knee joint was used to calculate the magnification factor on both anteroposterior (AP) and lateral (LAT) views. Two independent observers estimated the magnification to determine the intra and inter-observer reliability.
Results
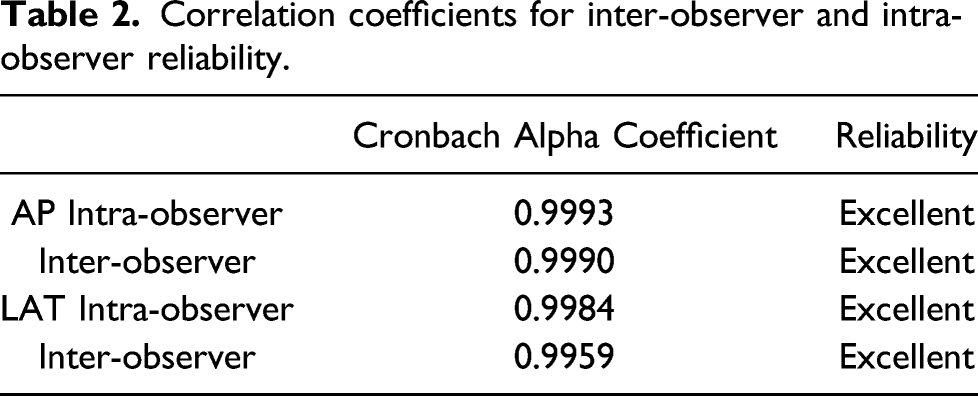
The mean magnification of the AP (15.3%) radiograph was significantly greater than the LAT (12.1%) radiograph (p< 0.0001). Patients with absent markers on their radiographs were heavier than patients in whom the marker was visible (84.7 kgs vs. 76.6 kgs, p=0.01). No marker was visible on the radiographs in 56.3% (45/80) of patients. There was excellent inter and intra-observer reliability of both the AP and LAT measurements.
Conclusion
After standardizing the protocol for preoperative knee radiographs, our results show significantly greater institutional magnification of the anteroposterior compared with the lateral images. Accurate templating in knee arthroplasty requires both radiographic images. To reduce errors in implant sizing, we recommend surgeons use different institutional magnification factors for the anteroposterior and lateral radiographs.
Introduction
Templating is an important exercise in preoperative planning for total knee arthroplasty (TKA), which has clinical, logistical and economic benefits.1,2 Preoperative templating allows surgeons to choose the most appropriate size of implant that would restore alignment and stability of the knee, resulting in better functional outcomes.1-3 Templating also facilitates improved theatre efficiency and lower cost; by identifying the implant sizes preoperatively, the correct sizes can be ordered in advance reducing cancellations and intraoperative delays.2,4
The technique used for templating should be both reproducible and accurate. There are primarily two templating methods; one uses an external marker and can be either digital or acetate-based; the other requires no marker, using patient demographic data instead to estimate the implant size. In the first method, the magnification of each radiograph is calculated using a standardised technique with an external marker of known size placed at the position of the knee. The radiographs are then superimposed upon manufacturer-supplied acetate templates of known magnification to estimate the sizes of the implants required. For digitally acquired radiographs, implant-specific templating software allows the magnification to be manipulated to match the image and template. Using this method, both acetate and digital templating have been shown to accurately predict the size of the implanted component to within one size in 91% and 93% of cases, respectively.2,3,4
Although accurate, external markers, interrupt the smooth workflow of a busy radiology department, adding both time and expense to the process. To address this issue, several studies have investigated the use of patient demographics to predict TKA implant size, reporting accuracy within one size in 85–100% of cases.1,5-7 In spite of its accuracy, surgeons are generally more comfortable viewing radiographs when templating, which allows them to analyse bone loss and deformity.
Therefore, the ideal templating system will seem to be both markerless and accurate yet allow surgeons to critically assess the preoperative radiographs. To this end, some surgeons have used a fixed institutional magnification for all preoperative radiographs. A prospective randomised surgeon-blinded study comparing institutional magnification with marker magnification in total hip arthroplasty (THA) showed no statistically significant difference between both methods. The institutional magnification group correctly predicted the femoral and acetabular implant within one size in 90% and 96% of cases, respectively. 8 To the best of our knowledge, similar studies involving TKA have not been performed.
Both patient factors and variations in the technique used to obtain radiographs (institutional factors) contribute to the inconsistent radiographic magnification of most radiology departments. Although guidelines exist, there are no universally accepted standards for taking knee radiographs. Therefore, to reduce errors due to institutional factors and achieve our primary aim, we first needed to standardise the technique at our hospital.
The primary aim of this study was to determine the institutional magnification of knee radiographs for patients awaiting total knee arthroplasty.
Material and methods
The Research Ethics Committee approved this study protocol, and all patients gave informed consent for participation (CEC318/1017).
All patients requiring a primary total knee replacement who attended the arthroplasty screening clinic over 3 months were eligible to be included in the study. During the time, 83 patients were recruited. We excluded three patients who obtained their knee radiographs at another institution, leaving 80 patients who had their radiographs taken using the standardised preoperative protocol.
The magnification theory of X-rays dictates that the greater the focus film distance (FFD), the smaller the magnification and the greater the knee film distance (KFD), the larger the magnification. Figures.1 and 2. In the absence of a universally agreed FFD for conventional radiographs, several authors have quoted different distances in their studies, leading to notable variation in the literature.9-11 Use of a standard protocol with an agreed FFD has been shown to increase the accuracy of templating radiographs in arthroplasty, with a mean absolute difference between measured and actual implant sizes of 0.16 mm.10,12 As a first step to improve both accuracy and reproducibility we standardised the FFD, using a distance of 1016 mm (40 inches).
4
Illustration of the magnification of the knee with a standard fixed focus distance (FFD) and a variable knee focus distance (KFD). The greater the KFD the greater the knee magnification. Illustration of the magnification of the knee with a non-standard fixed focus distance (FFD) and a fixed knee focus distance (KFD). The greater the FFD the smaller the knee magnification.

Our standardized technique ensured that one factor in the magnification equation, the FFD, was kept constant. The other factor, the distance between the centre of the knee joint and the film, the KFD, is variable and depends on the patient’s body habitus, in particular the size of their buttocks, thighs and calves. 13
All radiographs were obtained using the previously described standard protocol. The patients were positioned centre in the beam and close to the photographic plate so that their skin just touched the plate. Figure 3. We used a 22 mm metallic sphere attached to the patients’ skin with a Velcro strap as the external marker. The marker was placed at the level of the joint line, in the centre of the knee, which was assumed to be the centre of the knee joint on both the anteroposterior (AP) and lateral (LAT) images. The radiographers were instructed to repeat these steps as often as necessary to ensure a consistent marker position before taking the X-ray, but repeat x-rays were not permitted. All images were acquired using a 2003 Siemens® (Munich, Germany) machine, formatted and loaded onto the Picture Archiving and Communication System (PACS®). A typical set-up for the anteroposterior projection of both knees is shown. The source is 1016 mm (40 in) away and the beam centred at the level of the joint line.
The images were viewed using the Osirix® (version 2 64-bit; Pixmeo, Geneva, Switzerland) image processing system without digital modification. Measurements of the marker were taken by two experienced clinicians, one consultant orthopaedic surgeon and a consultant radiologist, with repeat measurements after 1 week. Measurements were recorded in millimetres and corrected to one decimal place. We calculated the magnification factor for both the AP (MF AP) and LAT images (MF LAT) and determined the intra and inter-observer reliability.
Data were collated using Excel ® (version 16.15, Microsoft, Redmond, Washington, USA), and descriptive statistics were used to analyse the variables and measurements. The difference between the AP and lateral projections were compared respectively, using a paired t-test for both. A one-sided t-test was used to compare patients with or without markers present on both the AP and LAT radiographs. Cronbach’s Alpha was used to assess the intra-observer and inter-observer reliability. Statistical analysis was performed using Stata® (version 14, StataCorp LLC, Texas, USA), and significance was assigned to a p-value < 0.05.
Results
Eighty patients underwent standardized knee radiographs prior to total knee arthroplasty. In 35 patients the marker used for estimation of knee magnification was seen on the radiographs, (Both AP and LAT 27, LAT only 7, AP only 1), but was absent in the remaining 45 patients.
The mean magnification on the AP (MF AP) radiograph was 15.3% (SD 6.35, n =112), and the mean magnification of the LAT (MF LAT) radiograph was 12.1% (SD 5.46, n=136). There was a significant difference between the MF AP and the MF LAT (p< 0.0001).
The mean age of the patients was 66.0 years (Range 44–86, SD 8.1). Patients were divided into two groups.
Group A: Marker visible on the radiographs
Group B: Marker not visible on the radiographs
Demographics of both groups, mean and standard deviation.

BMI- Body Mass Index * statistically significant
The mean weight of the patients in Group B was 84.7 kgs (SD 14.7 kgs) which was significantly greater than Group A, 76.6 kgs (SD 12.0 kgs) (p = 0.01).
Correlation coefficients for inter-observer and intra-observer reliability.
Discussion
There is general agreement among surgeons that preoperative templating is an important exercise and contributes to improved function and outcome in total knee arthroplasty. Because radiographs are a two-dimensional representation of a three-dimensional structure (the bones of the knee joint), predicting the exact size of the prosthesis with templates can be very difficult. The usefulness of templating goes far beyond estimating implant size, and arguably its primary purpose is to force the surgeon to think in three dimensions and anticipate potential difficulties. Notwithstanding this, using implants of the correct size is important, and implant manufacturers collectively recommend preoperative templating to estimate implant size.
We found the mean magnification of the marker on the anteroposterior and lateral radiographs to be 15.3% and 12.1%, respectively. Several studies looking at the correlation between the estimated magnification using a marker and the actual magnification in total hip replacement have shown contrasting results.9,14-16 These studies involve THA where investigators can use the spherical shape of the femoral head and acetabular shell to calculate the true magnification of the radiographs. Not surprisingly, there are no similar studies involving TKA since the complex geometrical shapes of the femoral and tibial components make exact measurements difficult. It is therefore impractical to routinely calculate the actual magnification of knee radiographs in the same way that it can be done for hip radiographs. The use of an external marker as a proxy for true magnification depends on accurate positioning of the marker. When bony anatomical landmarks are used, these must be identified by palpation, which is arguably more accessible in the knee compared with the hip joint.2, 9, 16
This study revealed a statistically significant difference between the MF AP and the MF LAT (15.3% vs 12.1%, p<0.0001). Templating in THA uses only the AP to estimate the size of both the acetabular and femoral components. However, when templating in TKA, both the AP and LAT radiographs are used; the AP primarily estimates the size of the tibial tray while the lateral is used for femoral component estimation. The accuracy of using a marker for templating in TKA has been demonstrated by several studies which show that femoral and tibial component sizes are within ±1 of the templated size in over 90% of cases.2,4,17 Studies using a marker for templating in TKA seem to indicate that the same magnification factor is used for templating both the anteroposterior and lateral radiographs. A retrospective study by Ooka et al. 17 reported that the lateral view was better at predicting the true size of the femoral and tibial components despite the same 10% magnification being used for both . We contend that both radiographs are independent investigations, and it should not be assumed that the magnification is identical.2,4,17
Our data show that no marker was visible on the radiographs in 56.3% (45/80) of patients. Interestingly, these patients were significantly heavier than patients in whom the marker could be seen. The only other study to look at the absence of a marker on knee radiographs reported a similar incidence of 53.6% (97/181). 1 In explaining this finding, it is likely that the practical difficulties encountered while positioning the markers in larger patients may have resulted in markers being placed outside of the X-ray beam. This finding questions the routine use of markers in templating for knee arthroplasty.
Eliminating markers while accurately predicting implant size can improve workflow in the Radiology department without compromising surgical outcomes. Templating using a marker is associated with increased costs, prolonged time, inconsistent marker position and a high proportion of missing markers, all of which are unwanted.8,9,16,17 Predictive modelling using patient demographic variables have shown to be comparable to marker methods for accuracy but limits its ability to account for bone loss and deformity, which are better appreciated on radiographs. 1
To get around this, some surgeons have adopted the use of a standard magnification factor during preoperative templating. The accuracy of this technique in THA has been shown by Archibeck et al., confirming that an external marker is not necessary. 8 Similarly, it should be possible to eliminate the need for a marker in TKA after calculating the institutional magnification of standard knee radiographs.
Unfortunately, the knee implant geometry does not allow for calculation of the true institutional magnification in TKA, and therefore our calculated institutional magnification is based on external markers. The accuracy of an external marker in determining magnification is controversial.9,14-16 However, our study’s findings of the mean marker magnification on both AP and lateral radiographs are within range of magnification used in other studies on TKA, which gives us confidence in the accuracy of our results.1,4
There are several weaknesses of this study. We instructed the radiographers to take only one radiograph in either view per patient as we sought to maintain the natural workflow of a busy radiology department. This stipulation may have led to the high percentage of radiographs with missing markers, thus reducing the sample size. Although all radiographers involved in this study underwent a pre-study instruction period in positioning of the marker, we cannot be certain that the technique, however meticulously carried out, actually placed the marker at the site of the bones. Our study also did not account for any fixed deformities of the knee joint, which would have affected the size of magnification and the probability that the marker would be visible on the film. Some strengths of our study include a heavily protocolled process with standardisation of the FFD. We used two experienced physicians taking multiple measurements of each marker in both planes to boost our study’s statistical and practical strength.
In conclusion, we set out to determine the institutional magnification of preoperative knee radiographs of patients awaiting TKA as a necessary step in templating. Our results indicate that the magnification of the anteroposterior knee radiograph is significantly greater than that of the lateral knee radiograph. This finding should be taken into consideration when templating for knee arthroplasty.
Our study also revealed that many radiographs did not have visible markers. On an individual basis, such a low yield procedure represents a significant waste of resources that cannot be justified in our underfunded healthcare system. This strengthens the case for the use of fixed institutional magnification in preoperative templating.
Footnotes
Acknowledgements
We gratefully acknowledge the invaluable contributions of Robbie Rampersad DM (observer), Dr David Deane MBBS (data collection) and Dr Diana Persaud MBBS (data collection).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.