
Abstract
Background
Meningiomas are occasionally fed by pial blood supply (PBS). It is postulated that peritumoral flow void (PTFV), peritumoral brain edema (PTBE), and absence of an arachnoid plane (AP) are useful parameters for evaluating PBS.
Purpose
To determine whether conventional magnetic resonance imaging (MRI) using a multiparametric scoring system (MSS) is a useful way to predict PBS.
Material and Methods
Forty-six patients were included and divided: PBS and non-PBS groups. Differences between the groups in six parameters of MR imaging were analyzed: tumor size, tumor location, PTBE grade, AP grade, PTFV, and MIB1 labeling index (MIB1-LI) grade. Cutoff values were determined using receiver operating characteristic (ROC) curve analysis for the differentiation of both groups based on statistically significant parameters. All cases were scored as 1 (PBS) or 0 (non-PBS) for each parameter according to set thresholds. Individual scores were totaled for each case, yielding a combined score for each case to obtain a cutoff value using ROC curve analysis for the MSS.
Results
Peritumoral brain edema grade, AP grade, PTFV, and MIB-LI grade were statistically associated with PBS. Receiver operating characteristic curve analyses showed that PTBE grade 3 or 4, AP grade 3 or 4, and PTFV positivity had the highest accuracy of 69%, 64%, and 68%, respectively. Regarding the MSS, a cutoff value of 2 had the highest accuracy of 71%; PBS diagnosis was indicated by at least two of the three parameters, namely, PTBE grade, AP grade, and PTFV.
Conclusion
The MSS is a useful way to predict PBS in intracranial meningiomas on MRI.
Keywords
Introduction
Meningiomas are common intracranial neoplasms and benign tumors1–6; however, tumor recurrence after surgical treatment is frequent.4,6.Ki-67/MIB-1 is a typical immunohistochemical marker of cell proliferation.7,8
On magnetic resonance imaging (MRI), meningiomas typically appear well-circumscribed.9,10 However, atypical cases may occur with unclear circumference and a variable extent of peritumoral edema, such that diagnosis, using conventional MRI sequences, is challenging.9–11
Meningiomas are principally supplied by external carotid artery branches, although they may also be fed by pial arteries that supply to the brain, namely, the pial blood supply (PBS). Cerebral angiography is the gold standard for evaluating PBS. The proliferation of pial vessels and their penetration to the arachnoid membrane are reported to cause disruption of the barrier surrounding the meningioma, which leads to adhesion to the brain. 12 Therefore, neurosurgeons pay careful attention to the presence of PBS because it may lead to difficulties in complete tumor resection and tumor recurrence. Advancing the date of surgery should also be considered when the presence of PBS is predicted, even if the tumor is small. Peritumoral flow void (PTFV) can be evaluated using conventional MRI as a substitute for PBS. 13 In addition, there are two important imaging features associated with meningiomas: absence of an arachnoid plane (AP) and peritumoral brain edema (PTBE). The AP is a brain–cerebrospinal barrier. 14 Peritumoral brain edema occurs in 30%–60% of meningiomas.12,15 Both AP and PTBE have been used for the evaluation of meningiomas on conventional MRI. PBS has been reported to be strongly associated with the presence of PTBE.15–17 The absence of AP has been reported to be correlated with PTBE 14 and PBS.18,19 Therefore, PTFV, AP, and PTBE are deeply associated with each other, and it is postulated that these will be useful parameters obtained by conventional MRI to evaluate PBS. Prediction of PBS only by conventional MRI may be useful in the clinical setting because it is a non-invasive procedure, unlike angiography. Tumor location (skull base or superficial) has been determined to be a significant factor for PTBE and PBS because vascularization of skull base meningiomas, relying on more proximal dural branches from internal carotid artery, might be different from that of superficial meningiomas.12,13,16
A multiparametric scoring system (MSS) is an original simple method that uses summed scores obtained by each parameter according to its threshold for discriminating between two groups. This scoring system can potentially offset an incorrect classification based on any single parameter and is expected to be a more useful indicator than any single parameter.20–22 Thus, the objective of this study was to perform a retrospective study of patients with meningiomas to determine whether conventional MRI using MSS is a useful way to predict PBS.
Material and methods
Patients
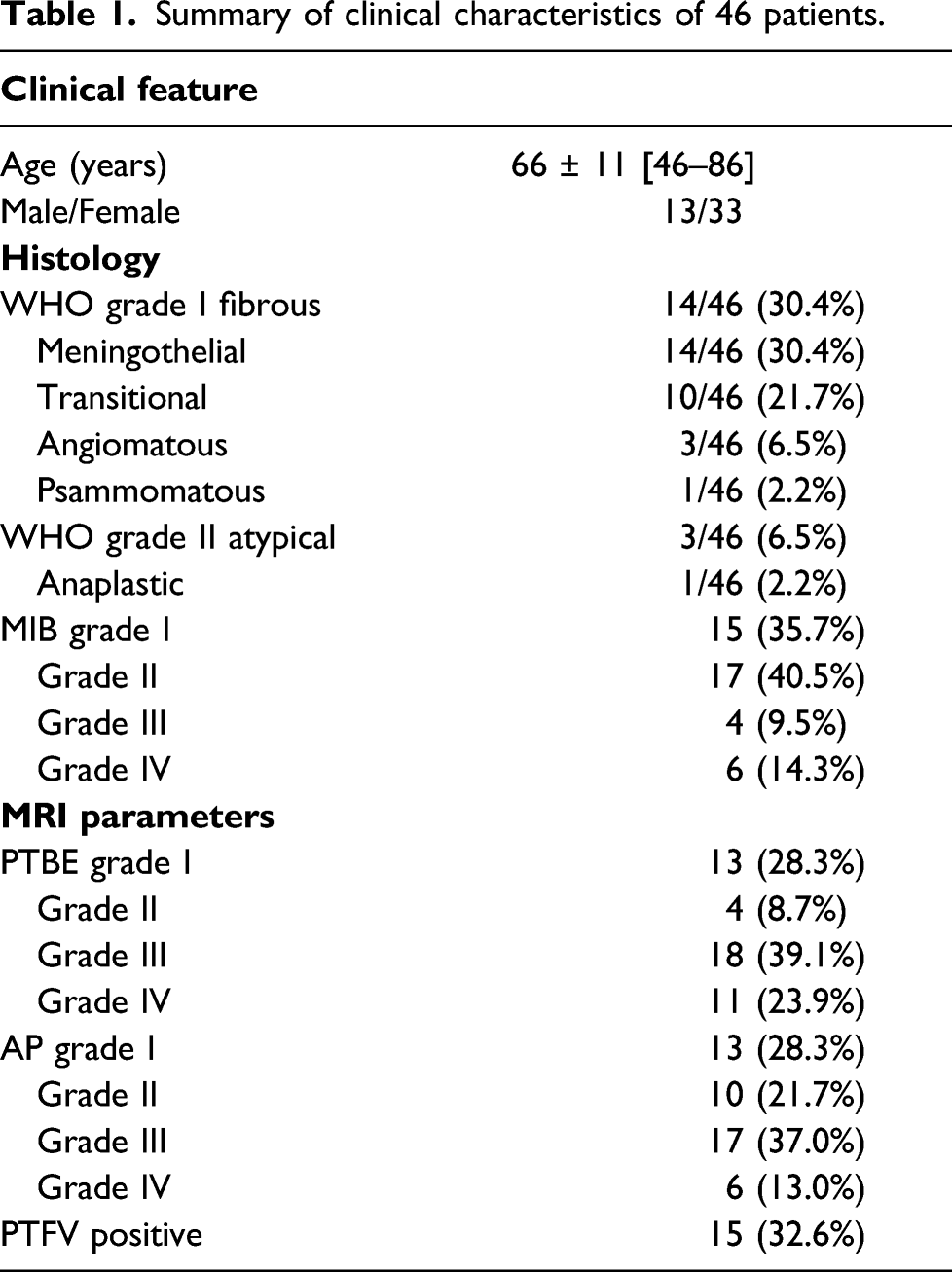
Summary of clinical characteristics of 46 patients.
This study was reviewed and approved by the institutional review board of our hospital. The hospital name is blinded. The correct information is shown in the tittle page.
Image acquisition of MRI
Magnetic resonance imaging was performed with three different systems; GE 1.5 T SIGNA was used between 2010 and 2014. Between 2015 and 2020, SIEMENS 1.5 T Aera and 3.0 T Skyra were used. Axial, coronal, and/or sagittal images were obtained in all cases.
The following MRI sequence parameters applied: GE 1.5 T. T1 FLAIR imaging: repetition time (TR)/echo time (TE)/inversion time (TI), 2500/11/2000 ms; matrix size, 320 × 320; field of view (FOV), 220 mm; slice thickness, 5.0 mm. T2-weighted imaging (T2WI); TR/TE, 4000/106 ms; matrix size, 256 × 256; FOV, 220 mm; and slice thickness, 5.0 mm. T2 FLAIR imaging; TR/TE/TI, 8000/142/2000 ms; matrix size, 256×256; FOV, 220 mm; and slice thickness, 5.0 mm.
SIEMENS 1.5 T. T1 FLAIR imaging: TR/TE/TI, 1800/14/890 ms; matrix size, 320 × 320; FOV, 220 mm; slice thickness, 5.0 mm. T2WI; TR/TE, 4000/91 ms; matrix size, 320 × 320; FOV, 220 mm; slice thickness, 5.0 mm. T2 FLAIR imaging; TR/TE/TI, 8500/107/2440 ms; matrix size, 256 × 256; FOV, 220 mm; and slice thickness, 5.0 mm.
SIEMENS 3.0 T. T1 FLAIR imaging: TR/TE/TI, 1800/13/890 ms; matrix size, 384 × 384; FOV, 220 mm; and slice thickness, 5.0 mm. T2WI; TR/TE, 5000/86 ms; matrix size, 448 × 448; FOV, 220 mm; and slice thickness, 5.0 mm. T2 FLAIR imaging; TR/TE/TI, 10000/99/2640 ms; matrix size, 256 × 256; FOV, 220 mm; and slice thickness, 5.0 mm.
Digital subtraction angiography analysis
Between 2010 and 2014, digital subtraction angiography (DSA) was performed using a single-plane angiography unit, INNOVA3100 (GE, Connecticut, USA), and biplane angiography was performed between 2015 and 2020 using an Artis zee BA Twin (SIEMENS, Bayern, Germany) system. Pial blood supply was defined as the presence of a tumor blush that was fed by pial artery on brain tumor interfaces. 17 The assessment of PBS was performed by an interventional neurosurgeon with 20 years of experience (S.I), blinded to the MRI results.
Magnetic resonance imaging analysis
The following parameters were obtained by MRI: tumor size, tumor location, PTBE grade, PTFV grade, and AP grade; they were independently investigated by a neuroradiologist with 15 years of experience (F.H) and a neurosurgeon with 20 years of experience (S.I), blinded to the DSA results. Maximum tumor diameter on axial, sagittal, or coronal images was measured in centimeters on T1 FLAIR imaging. Tumor location was divided into two groups: skull base and non-skull base. The maximum PTBE was evaluated on T2WI or T2 FLAIR imaging on axial, sagittal, and/or coronal images. Peritumoral brain edema grade was categorized into four groups as follows: grade 1, no edema; grade 2, peripheral edema; grade 3, less than twice the mass (the maximum diameter) of edema; and grade 4, more than twice the mass (the maximum diameter) (Figure 1). Peritumoral flow voids were graded as present or absent on T2WI or T2 FLAIR imaging
13
(Figure 2). Finally, the presence/absence of AP around the tumor margin was evaluated using T2WI or T2 FLAIR imaging. The AP grade was categorized into four groups: grade 1, whole presence; grade 2, over half presence; grade 3, up to half presence; and grade 4, absence (Figure 3). Representative T2-weighted images for PTBE grading are shown. (a) No edema was observed around the right frontal mass (grade 1) (white arrowed). (b) Peripheral edema around the right frontal mass (grade 2) (red arrowed). (c) Less than twice the mass of edema around the right frontal mass (grade 3) (red arrowed). (d) More than twice the mass of edema around the left frontal mass (grade 4) (red arrowed). Representative T2-weighted images for peritumoral flow void (PTFV) grading are shown. (a) PTFVs are present around the left fronto-parietal mass (red arrowed). (b) PTFVs are absent around the left temporal mass (white arrowed). Representative T2-weighted images for arachnoid plane (AP) grading are shown. (a) AP around the left fronto-parietal mass shows whole presence (grade 1) (red arrowed). (b) AP around the right frontal mass shows over half presence (grade 2) (red arrowed is AP positive, white arrowed is AP negative). (c) AP around the left frontal mass shows up to half presence (grade 3) (red arrowed is AP positive, white arrowed is AP negative). (d) AP around the left temporal mass shows absence (grade 4) (white arrowed).


MIB1-LI grading
All tumor samples were classified into histological subtypes according to the WHO classification for tumors of the CNS. MIB1-LI grade was classified into four groups: grade 1 (up to 1%), grade 2 (2%–3%), grade 3 (4%–9%), and grade 4 (10% or more).
Statistical analysis
Statistical analysis of the differences between the PBS and non-PBS groups in the six parameters (tumor size, tumor location, PTBE grade, AP grade, PTFVs, and MIB1-LI grade) was performed using the Mann–Whitney U test.
For the differentiation of the PBS group from the non-PBS group, cutoff values that provided the optimal combination of sensitivity and specificity for each parameter were selected using receiver operating characteristic (ROC) curve analysis. Cutoff values were determined using the Youden index. We determined the accuracy, sensitivity, specificity, positive predictive value, and negative predictive value of each parameter using chi-square analysis. The area under the ROC curve (Az) for each parameter was also evaluated. For the differentiation of the PBS group from the non-PBS group, we adapted statistically useful parameters among the following five parameters using MRI: tumor size, tumor location, PTBE grade, AP grade, and PTFVs for the evaluation of the MSS. All cases were scored as either 1 (PBS) or 0 (non-PBS) for each selected parameter according to the threshold. These individual scores were totaled for each subject, yielding a combined score for each case. To evaluate the properties of the scoring system, we calculated the accuracy, sensitivity, and specificity of the MSS with possible cutoff values using chi-square analysis. In addition, ROC curve analysis was performed to obtain a cutoff value for the MSS. Statistical significance was set at a p-value of < .05. All statistical analyses were performed using IBM SPSS Statistics version 26.
Results
Vascularity from meningeal vessels was observed in all 46 tumors, of which 16 had both a meningeal supply and pial supply. The tumors with a double supply were classified to PBS group, and the tumors with only a meningeal supply were classified to non-PBS group.
Differences between the pial blood supply and non-pial blood supply group in the six parameters.

Note. - PBS, pial blood supply; PTFV, peritumoral flow void; PTBE, peritumoral brain edema; AP, arachnoid plane; MIB-LI, MIB-1-labeling index.
Diagnostic tests of each adapted MRI parameter and the MSS in differentiating the pial supply group from non-pial supply group.

For the evaluation of the MSS, discriminating the PBS group from non-PBS group, we adapted the following three statistically useful parameters of each case obtained by MRI: PTBE grade, AP grade, and PTFV grade. Next, ROC curve was obtained by using adapted scores from the PBS and non-PBS groups. The MSS was classified into three cutoff values: MSS-1st, MSS-2nd, and MSS-3rd. For MSS-1st, the highest accuracy for discriminating the PBS group from the non-PBS group was 71%; the sensitivity and specificity were 81% and 60%, respectively; the positive and negative predictive values were 67% and 76%, respectively, at a cutoff value of 2. Pial blood supply diagnosis was indicated by at least two of the three parameters. At this threshold, cases with total scores of 0 and 1 indicated non-PBS and cases with total scores of 2 and 3 indicated PBS (Az 0.78). For the MSS-2nd, the second highest accuracy was 68%, and sensitivity was 100% at a cutoff value of 1; PBS diagnosis was indicated by at least one of the three parameters. Finally, for the MSS-3rd, the lowest accuracy was 62% and sensitivity was 31% at a cutoff value of 3; PBS diagnosis was indicated by all the three parameters.
Representative images of DSA and MRI for the non-PBS and PBS groups are shown in Figures 4 and 5, respectively. Representative images of a case with pial blood supply (PBS) are shown. (a) An axial T2-weighted image shows frontal mass with adjacent widely cerebral edema (PTBE grade 4), presence of peritumoral flow void of the mass (red arrowed) and arachnoid plane shows absence (AP grade 4). (b) Digital subtraction angiography image shows PBS of cerebral arteries (red arrowed). Representative images of a case with non-pial blood supply (non-PBS) are shown. (a) An axial T2-weighted image shows frontal mass (white arrowed) without adjacent cerebral edema (PTBE grade 1), the absence of peritumoral flow void of the mass and arachnoid plane shows over half presence of the mass (AP grade 2). (b) Digital subtraction angiography image shows non-PBS of cerebral arteries (white arrowed).

Discussion
This study evaluated whether conventional MRI using MSS is a useful way to predict PBS. We evaluated MSS, and it could improve the diagnostic accuracy in differentiating the PBS group from the non-PBS group in terms of meningiomas. The analysis showed good test accuracy (71%) for PBS group versus non-PBS group differentiation using each parameter (PTBE grade 69%, AP grade 64%, and PTFV 68%). The highest accuracy was obtained using MSS-1st if at least two of the three parameters were positive for PBS. Conventional MRI using this scoring system to discriminate the PBS group from the non-PBS group may provide additional value to predict PBS in meningiomas without cerebral angiography.
Meningiomas are usually supplied by the external carotid artery branch (i.e., the middle meningeal artery). Moreover, they are sometimes supplied by the pial artery on brain tumor interfaces as the PBS. In meningiomas, the presence of PBS is associated with tumor adhesion to the brain parenchyma. Additionally, PBS can be associated with difficulties with intraoperative operation, increased recurrence rates, and intraoperative complications.12,13 Furthermore, it has been reported that embolization, which is often performed before surgery, is also difficult to perform in meningiomas with PBS. 23 Regarding factors associated with PBS, tumor size, tumor location, PTBE, PTFVs, AP, and high WHO grades have been reported.12,13 Our study revealed that PTBE grade, presence of PTFVs, AP grade, and MIB-LI grade were significantly useful factors for discriminating PBS from non-PBS, consistent with previous reports.7,8,12–19 Magnetic resonance imaging is a non-invasive examination that can be performed in almost all meningiomas, and it is useful to predict PBS using MRI findings before performing embolization or surgery.
T2-weighted flow voids, as feeder arteries for meningiomas, are often observed in the dural zone of the tumor. Flow voids may be observed on the brain surface, leptomeningeal membranes in contact with tumors, or even in the subcortical white matter, namely, PTFV. Peritumoral flow voids are thought to be correlated with PBS rather than blood flow from the external carotid branch. 13 Our study showed a significant correlation between PTFV and PBS. Therefore, PTFVs in meningiomas can provide helpful findings for predicting PBS.
Most meningiomas have rim-like structures, showing T2 high-signal intensity equal to that of cerebrospinal fluid (CSF) between the cerebral cortex and tumor, namely, the CSF rim, and this finding can be classified as an extra-axial tumor. However, PBS is associated with adhesion between tumors and brain parenchyma and obscure boundaries, and results in an incomplete CSF rim,13,14,18,19 which is representative of a high-AP-grade. Consistent with previous reports, our study revealed that a high AP grade could predict PBS.13,14,18,19
Peritumoral brain edema in meningiomas is considered vasogenic. Various degrees of PTBE have been observed.12,15 Many factors associated with PTBE, including tumor volume, tumor location, PBS, venous occlusion, pathological malignancy, vascular endothelial growth factor (VEGF), interleukin-6, and matrix metalloproteinase 9, have been reported.12,24,25 High Ki-67/MIB-LI has been reported to be associated with PTBE in meningiomas. Furthermore, MIB-LI score of ≥ 4% is correlated with PTBE.12,14 Our study showed that both high MIB-LI and high PTBE were associated with PBS and can be influenced by each other.
The CSF space and membrane structure between the tumor and brain parenchyma are important structures associated with PTBE in meningiomas. 14 In addition, VEGF is an important factor related to PTBE in meningiomas; released VEGF in meningiomas causes proliferation of pial blood vessels, which penetrate into the tumor to destroy its surrounding barrier.12,24,25 In this study, PTBE grade 3 and grade 4, namely, moderate to severe edema, were significantly correlated with PBS, which is consistent with the findings of previous reports.16,17 Hence, a high PTBE may be an important predictor of PBS.
Meningiomas are usually followed up periodically by MRI. Magnetic resonance imaging parameters of PTFV, AP, and PTBE are significant, and therefore, MSS using all these significant parameters may be useful in the clinical setting to determine the optimal MRI time intervals. When two of the three parameters, high AP grade (grade 3 or 4), high PTBE grade (grade 3 or 4), and positive PTFVs, were positive on MSS, PBS was more likely to be predicted. In these cases, neurosurgeons should consider a shortened follow-up duration or early surgery, even if the tumor is small. When the MSS score is 0, with low AP grade (grade 1 or 2), low PTBE grades (grade 1 or 2), and negative PTFVs, non-PBS is more likely to be predicted. In these cases, usual follow-up can be recommended.
Friconnet et al. 13 reported that in the MRI predictive score system of pial vascularization, a high score with PTFV and incomplete CSF rim is associated with pial supply, and our results are consistent with this. Additionally, our PTBE grade and AP grade are easily visualized systems for radiologists and neurosurgeons. Also, three MSS (MSS 1st, 2nd, and 3rd) in this study are useful predictive systems with three cutoff values, that is, three variated patterns of PTBE, AP, and PTFV.
Our study has several limitations. First, this study was conducted in a single hospital and the study population was small. Second, the acquisition of three different systems (GE1.5 T, Siemens 1.5 T, and 3.0 T) may be a limitation. However, the selected MRI parameters were not necessarily dependent on the system. Third, advanced DWI, PWI, and MRS imaging were not investigated. Because of these limitations, further validation with a larger number of cases is needed. Despite these limitations, in our view, this simple evaluation method using the MSS will be useful in determining PBS of meningiomas using conventional MRI.
In conclusion, MSS is a useful way to predict PBS in intracranial meningiomas on conventional MRI.
Footnotes
Acknowledgments
We are grateful for expert assistance given by members of the Department of Radiological Technology, Okayama City Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.