
Abstract
Background
Whole-body magnetic resonance imaging (WB-MRI) is a useful tool for revealing the disease-specific distribution of affected muscles and clinically asymptomatic muscle involvements in idiopathic inflammatory myopathies (IIMs).
Purpose
To examine inflammatory changes in the systemic skeletal muscles, including the thoracoabdominal trunk, in IIMs using WB-MRI.
Material and Methods
We prospectively obtained WB-MRI axial images from 10 patients with IIMs, including antisynthetase syndrome (ASS), immune-mediated necrotizing myopathy (IMNM), sporadic inclusion body myositis, and myopathy associated with antimitochondrial antibody. We evaluated 108 systemic skeletal muscles in short-tau inversion recovery (STIR) images and rated changes in signal intensity using a semiquantitative scale. Correlations between STIR sum score, peak creatine kinase (CK) and muscle strength were examined. We also investigated the correlation between STIR sum score within the thoracoabdominal trunk and forced vital capacity.
Results
High STIR signal changes were frequently identified in asymptomatic and routinely unexamined muscles. Thoracoabdominal trunk muscles were frequently involved in ASS and IMNM. Peak CK was positively correlated with the STIR sum score (R2 = 0.62, p < .01). There was no significant correlation between the STIR sum score within the thoracoabdominal trunk and forced vital capacity.
Conclusion
WB-MRI can detect subclinical muscle inflammation in the systemic muscles including the trunk muscles. STIR sum score is positively correlated with serum peak CK level; therefore, it could be a biomarker of overall muscle inflammation.
Keywords
Introduction
Idiopathic inflammatory myopathies (IIMs) are a group of rare diseases with heterogenous autoimmune mechanisms. IIMs are characterized by muscle inflammation and weakness, increases in serum muscle enzymes, presence of serum antibodies, and lymphocytic infiltrates in muscle biopsies. 1 In recent years, detection of novel autoantibodies and progress in pathological studies have revealed much about the pathophysiological processes in various subtypes of IIMs; however, the exact cause of each disease remains unclear. Traditionally, IIM patients were classified as having dermatomyositis with a characteristic rash and as having polymyositis without a rash. However, with the discovery of serum biomarkers, the spectrum of IIMs has been significantly changed and extended. According to contemporary criteria, many patients previously diagnosed with dermatomyositis are classified as having antisynthetase syndrome (ASS). 2 Dermatomyositis has been redefined based on the specific pathology and autoantibodies associated with unique clinical phenotypes.2,3 Other main subtypes of IIMs include immune-mediated necrotizing myopathy (IMNM) 4 and sporadic inclusion body myositis (sIBM).
Except for sIBM, major subtypes of IIMs present with acute or subacute onset of symmetric proximal muscle weakness. Regarding the distribution of muscle weakness in IIMs, the involvement of the thoracoabdominal trunk muscles has not been fully investigated because the weakness is less likely to appear as a symptom and is seldom evaluated by manual muscle testing or needle electromyography.
Given its excellent soft-tissue contrast, magnetic resonance imaging (MRI) is the most sensitive imaging method for detecting skeletal muscle abnormalities related to IIMs.5,6 Active muscle inflammation can be sensitively detected by short-tau inversion recovery (STIR) imaging, and fat infiltration in the chronic stage can be detected by T1-weighted imaging. 7 Whole-body MRI (WB-MRI) was recently reported to be useful in revealing the disease-specific distribution of affected muscles and clinically asymptomatic muscle involvements in some subtypes of IIMs.8,9 To clarify the involvement of the thoracoabdominal trunk muscles in IIMs, we evaluated systemic skeletal muscles, focusing not only on the limbs but also on the trunk, by applying WB-MRI STIR images in 10 Japanese patients with IIMs.
Material and methods
Patients
The study was approved by the ethics committee of the University Hospital and conducted in compliance with the Declaration of Helsinki guidelines. Written informed consent was obtained from all patients. 10 consecutive patients with IIMs that were treated in our department between October 2016 and March 2020 were enrolled, after excluding two patients who did not provide informed consent. These patients were diagnosed with IIMs based on the 2004 European Neuromuscular Center criteria or Griggs’ criteria for sIBM.10,11 Our studies included four IIM subtypes (ASS, IMNM, sIBM, and myopathy associated with antimitochondrial antibody [MAMA]) based on the autoantibody profiles and muscle biopsy findings. MAMA is now recognized as another distinct subtype of IIMs. 12 The WB-MRI findings in one patient with ASS (patient 2) were previously described in a case report. 13
Muscle strength was evaluated with the Medical Research Council (MRC) scale. 14 The MRC sum score was obtained by summing the scores on the MRC scale for the following muscles on both sides: arm abduction, forearm flexion, wrist extension, leg flexion, knee extension, and foot dorsiflexion. The MRC sum score ranged from 0 (complete paresis) to 60 (normal). 15
Whole-body MRI examination protocol
WB-MRI was performed with a 3-Tesla MRI system (PET/MR Biograph mMR, Siemens Healthineers, Erlangen, Germany) using body coils with a field of view from the neck to legs. Different sequences were used for axial STIR images (TR = 3000 ms, TE = 69 ms, TI = 230 ms, slice thickness = 6 mm, slice gap = 21 mm) and axial T1-weighted images (TR = 450 ms, TE = 8.7 ms, slice thickness = 6 mm, and slice gap = 21 mm). In some cases, we added coronal STIR and T1-weighted images. The total scan time was 20–35 min.
Image analysis and STIR score
We evaluated the degree of muscle inflammation in skeletal muscles on axial STIR images based on the following principles: Muscle inflammation is known to increase extracellular and/or intracellular water, leading to high signal intensity changes on STIR images. Fat infiltration into the muscles leads to high signal intensity changes on T1-weighted images. We rated the degree of muscle inflammation on STIR images (quantified as the STIR score) using the following previously reported semiquantitative scale16,17: (0). Normal appearance (1). Patchy isolated high signal intensity changes (2). Patchy widespread high signal intensity changes (3). Diffuse homogenous high signal intensity changes
Examples of the evaluation criteria are shown in Figure 1. We also evaluated the presence of fascial involvements. Axial short-tau inversion recovery (STIR) images of the right thigh obtained from example cases (a–e). The white solid line indicates the vastus lateralis (VL) muscle. The muscle outline is not shown in E to visualize fascial involvement. The STIR score of the VL is 0 (normal) in a, 1 (patchy isolated high signal intensity changes) in b, 2 (patchy widespread high signal intensity changes) in c, and 3 (diffuse homogenous high signal intensity changes) in d. Fasciae of the thigh muscles in e show high STIR signals (yellow arrowheads).
One neurologist with expertise in muscle MRI and one radiologist independently evaluated the WB-MRI and rated the STIR images. One of these raters was blinded to all clinical information, including diagnoses. The interrater agreement of the STIR scores for each muscle was quantified based on Cohen’s kappa coefficients: 0–0.2, poor; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, substantial; and 0.81–1.0, almost perfect.18,19 Data were analyzed by using statistical software (MATLAB). Averaged scores of the two raters were used for analyses.
Distribution of muscle inflammation by WB-MRI and clinical-radiological correlation
Based on Wattjes and Fischer,7 we selected the following 54 (bilaterally 108) reliably identifiable muscles (Figure 2); forearm muscles were not evaluated in this study because the image quality on WB-MRI was poor due to inhomogeneous fat suppression in the peripheral field of view7,20: Neck (4 pairs of muscles): sternocleidomastoid (SCM), trapezius (TR), levator scapulae (LSc), and cervical paraspinal (CPSp) muscles Upper arm (4 pairs of muscles): deltoid (DE), biceps brachii (BB), coracobrachialis (CB), and triceps brachii (TB) muscles Thoracic trunk (9 pairs of muscles): pectoralis major (PMa), pectoralis minor (PMi), supraspinatus (SS), infraspinatus (IS), subscapularis (SSc), latissimus dorsi (LD), serratus anterior (SA), rhomboid (RH), and thoracic paraspinal (TPSp) muscles Abdominal trunk (6 pairs of muscles): rectus abdominis (RA), external oblique abdominis (EOA), internal oblique abdominis (IOA), transversus abdominis (TrA), quadratus lumborum (QL), and lumbar paraspinal (LPSp) muscles Pelvis (10 pairs of muscles): psoas (PS), iliacus (IL), gluteus maximus (GMa), gluteus medius (GMe), gluteus minimus (GMm), piriformis (PI), pectineus (PE), obturator externus (OE), obturator internus (OI), and quadratus femoris (QF) muscles Thigh (14 pairs of muscles): rectus femoris (RF), vastus intermedius (VI), vastus lateralis (VL), vastus medialis (VM), tensor fasciae latae (TFL), sartorius (SA), gracilis (GR), adductor brevis (AB), adductor longus (AL), adductor magnus (AM), biceps femoris long head (BL), biceps femoris short head (BS), semimembranosus (SM), and semitendinosus (ST) muscles Calf (7 pairs of muscles): tibialis anterior (TA), extensor digitorum longus (EDL), peroneus longus (PL), tibialis posterior (TP), soleus (SO), lateral gastrocnemius (GL), and medial gastrocnemius (GM) muscles Axial images of the 54 muscles identified and evaluated in the present study: (a) neck, (b) shoulder and thoracic trunk, (c) upper arm and thoracic trunk, (d) abdominal trunk, (e, f) pelvis, (g) thigh, and (h) calf. Abbreviations are described in the text.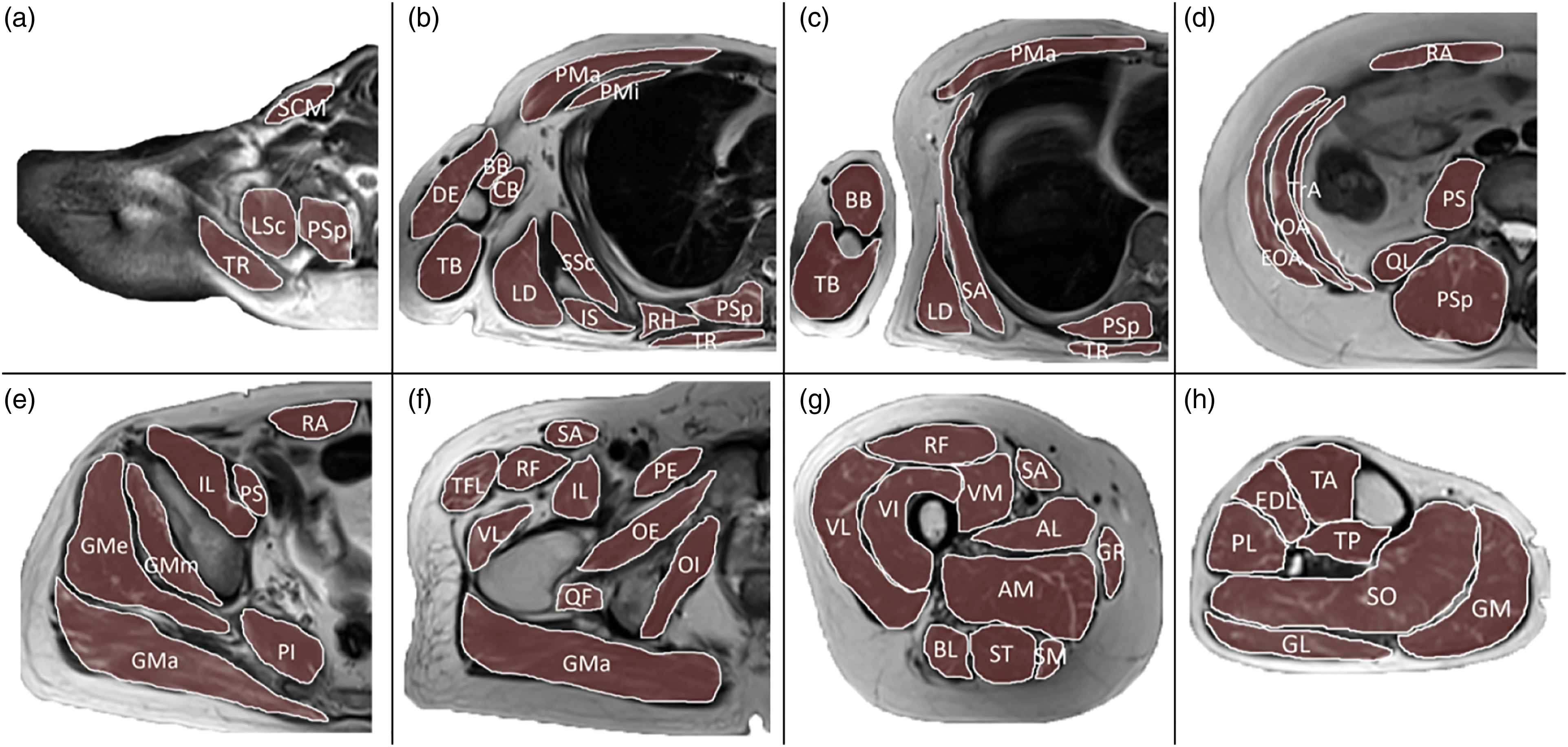
Some muscles were technically difficult to identify in some patients due to imaging artifacts; those muscles were excluded from this study. The following muscles were included bilaterally in this analysis for changes in STIR signals: neck, TR and CPSp; upper arm, DE, BB, CB, and TB; trunk, PMa, PMi, IS, SSc, LD, SA, RH, TPSp, EOA, IOA, TrA, QL, and LPSp; pelvis, PS, IL, GMa, GMe, GMm, PI, PE, OI, and QF; thigh, RF, VI, VL, VM, TFL, SA, GR, AB, AL, AM, BL, BS, SM, and ST; and calf, TA, EDL, PL, TP, SO, GL, and GM. As an indicator of overall muscle inflammation, we calculated the STIR sum score of the above-described bilaterally 98 muscles that were reliably rated by the two raters. To examine clinical-radiological correlations, we compared the STIR sum score as measured on the MRC sum score and peak serum creatine kinase (CK) level by linear regression analysis. Additionally, we examined the correlation between STIR sum score within the thoracoabdominal trunk and forced vital capacity in nine patients. Patient 1 was excluded from the respiratory function analysis due to interstitial lung disease. Data were analyzed by using statistical software (SPSS, version 27). In all analyses, p < .05 was defined as statistically significant.
Results
Patients
Demographic and clinical characteristics of 10 patients with idiopathic inflammatory myopathies (IIMs).

Abbreviations: AMA: antimitochondrial antibody; ASS: antisynthetase syndrome; CK: creatine kinase; F: female; FVC: forced vital capacity; HMGCR: 3-hydroxy-3-methylglutaryl-coenzyme A reductase; IMNM: immune-mediated necrotizing myopathy; M: male; MAA: myositis-associated antibody; MAMA: myopathy associated with antimitochondrial antibody; MRC: Medical Research Council; MSA: myositis-specific antibody; PSL: prednisolone; sIBM: sporadic inclusion body myositis; SRP: signal recognition particle; TAC: tacrolimus.
Representative cases
Patient 1: ASS
A 19-year-old woman noticed myalgia and difficulty climbing stairs over the previous 2 weeks. Physical examination revealed mechanic’s hand and mild polyarthropathy. The neurological examination showed MRC grade 4 weakness in the iliopsoas muscles. In the laboratory examination, the serum CK was abnormally elevated and anti-Jo-1 antibody was detected. We diagnosed her as having anti-Jo-1 myopathy with interstitial lung disease. Her symptoms improved after corticosteroid and cyclosporine treatment. WB-MRI detected high STIR signal intensity changes in the muscles and fascia of the lower limbs, pelvis, and abdominal trunk (Figure 3). Whole-body MRI in two patients with antisynthetase syndrome (ASS): a 19-year-old woman (patient 1) (a)–(d) and a 33-year-old woman (patient 2) (e)–(h) in the acute phase. High STIR signals were widely observed in muscles of the trunk (a), (e), (f), pelvis (b), (g), thigh (c), (h), and calf (d). Fascia showed high signal intensity changes in the abdominal, pelvic, and thigh muscles (yellow arrowheads).
Patient 5: IMNM
An 83-year-old man with a history of hypertension and bronchial asthma developed proximal limb weakness with hyperCKemia over the previous 2 months. He showed MRC grade 3–4 weakness in the proximal limb muscles. The left RF muscle biopsy revealed necrotizing myopathy with minimal lymphocytic infiltration. His serum was positive for anti-HMGCR antibody. Under the diagnosis of IMNM, he was treated with oral corticosteroid, tacrolimus, and intravenous immunoglobulin. WB-MRI revealed widespread systemic muscle inflammation on STIR images (Figure 4). Whole-body MRI of a patient with anti-HMGCR (3-hydroxy-3-methylglutaryl-coenzyme A reductase) antibody-positive immune-mediated necrotizing myopathy (IMNM) (patient 5). STIR (a–c) and T1-weighted (d, e) images. High STIR signal intensity changes are present in the pelvic, thigh, and calf muscles on coronal (a) and axial (b, c) images. Fat infiltration is confirmed on T1-weighted images (d, e). Quadriceps femoris muscles showed atrophic changes (yellow arrows in b).
Patient 7: MAMA
A 61-year-old man with chronic heart failure was referred to our department with a complaint of chronic proximal limb weakness and elevated serum CK. His serum was positive for antimitochondrial M2 antibody. A left BB biopsy revealed marked variation in the sizes of muscle fibers and a mixture of necrotic and regenerating fibers. We diagnosed him as MAMA combined with cardiomyopathy and primary biliary cirrhosis. WB-MRI showed high STIR signals in the muscles of the abdominal wall, pelvis, and thigh (Figure 5). The IL exhibited particularly remarkable signal changes. Whole-body MRI in two patients with myopathy associated with antimitochondrial antibody (MAMA): a 61-year-old man (patient 7) (a)–(c) and a 69-year-old man (patient 8) (d), (e). Coronal STIR image showed remarkable high signal intensity changes in the iliacus muscles (yellow arrowheads). (a) Axial STIR images depicted increased signal intensities in the iliacus (yellow arrowheads) and abdominal muscles (yellow arrows) in both patients (b, d). The iliacus muscles appeared isointense on axial T1-weighted images, suggesting acute inflammation without fatty replacement (c, e).
STIR score and distribution of muscle inflammation
Whole-body MRI findings of 10 patients with IIMs.

Inflammatory changes in short-tau inversion recovery (STIR) images were rated from 0 to 3 (right/left; see main text for details). The table lists the average STIR scores of two independent raters. *, p < .05; **, p < .01, ***, p < .001. Abbreviations: Cohen’s κ: Cohen’s kappa coefficient; F: high STIR signal in the fascia; trunk STIR sum score: STIR sum score within thoracic and abdominal trunk. Abbreviations the muscles are defined in the main text.
amuscles included when calculating the STIR sum score.
Relationships between STIR sum score, muscle strength, peak CK and forced vital capacity
The serum peak CK level is known to be correlated with the activity of IIMs; thus, peak CK may be predictive of the MRI correlates of muscle inflammation. We examined this possibility by conducting a linear regression analysis, which produced a significant regression equation (STIR sum score = 3.05×10−2 peak CK + 43.4; F(1, 8) = 14.2, p < .01) with an R2 of 0.62 (Figure 6(a)). A simple linear regression to predict the STIR sum score based on the MRC sum score was not significant (R2 = 0.18, p = .22) (Figure 6(b)). STIR sum score within the thoracoabdominal trunk was not significantly correlated with forced vital capacity (R2 = 0.28, p = .058). Scatter plots showing the relationships between peak creatine kinase (CK) and STIR sum score (a) and between MRC sum score and STIR sum score (b). The regression line in (a) indicates a significant linear relationship (R2 = 0.62, p < .01). There was no significant relationship between the MRC and STIR sum scores (R2 = 0.18, p = .22). Symbols represent subtypes of IIMs: ASS (squares), IMNM (circles), MAMA (triangles), and sIBM (diamonds).
Discussion
We evaluated the systemic skeletal muscles in 10 Japanese patients with IIMs using WB-MRI. The utility of WB-MRI in IIMs has been reported previously8,21; however, the use of coronal MRI sections in those studies made it difficult to accurately identify muscles. The use of whole-body axial images in our study allowed evaluations of 54 (bilaterally 108) muscles in most patients and 49 (bilaterally 98) muscles in all patients. Changes in STIR signals were detectable in the asymptomatic muscles and in muscles whose strengths are difficult to measure. Our study emphasized that subclinical inflammation of the thoracoabdominal trunk muscles was unexpectedly frequent and underestimated in routine clinical practice. The number of patients for each IIM subtype in our study was small; thus, our conclusions are only preliminary.
Abnormal high STIR signals were diffusely distributed in ASS and IMNM, whereas involved muscles were less extensive and more selective in MAMA and sIBM (Table 2). Although inflammation of trunk muscles has received little attention previously in IIMs, the thoracoabdominal trunk muscles showed STIR high signal changes in ASS, IMNM, and MAMA in this study. The trunk muscle disturbance was correlated to lower general mobility, impairment of balance, and use of ventilatory support in muscular dystrophy; however, no systematic study has been conducted on trunk weakness in patients with IIMs. Moreover, since the trunk muscles are rarely examined by the MMT and seldom evaluated by needle electromyography, involvement of the trunk muscles in IIMs appears to be clinically underestimated. There is a need for more studies on trunk muscle involvement in IIMs, including various subtypes, with larger cohorts.
The abdominal wall and pelvic muscles were preferentially involved in MAMA, consistent with previous reports.22,23 In addition, IL exhibited prominent high STIR signal intensities in MAMA patients, which has not been reported previously (Figure 5). In ASS and IMNM, the lower leg muscles exhibited high STIR signals despite having normal strength. Subclinical inflammation in the lower leg muscles has also been reported in previous imaging studies.24,25 Although proximal weakness is a well-established clinical feature of IIMs, MRI may sensitively detect subclinical distal muscle involvements. We found that muscle inflammation detected using STIR images was more localized and less severe in sIBM compared with other IIM subtypes, consistent with previous papers. 26
The STIR sum score is a global MRI measure of muscle inflammation; it showed a linear relationship with peak CK (Figure 6(a)). Therefore, gross changes in STIR signals in IIMs can be predicted from a given peak CK value. In contrast, the MRC sum score was not a good predictor of changes in STIR signals (Figure 6(b)). Although we predicted that inflammation of the thoracic and abdominal trunk muscles would affect respiratory function, the STIR sum score within the thoracoabdominal trunk was not significantly correlated with forced vital capacity in our study. There are several possible explanations for dissociation between trunk muscle involvement and respiratory impairment. First, the number of patients with IIMs in our study was too small to determine a statistically significant difference. Second, we could not examine STIR signal changes in the diaphragm, which is responsible for more than two-thirds of the ventilatory effort; therefore, the diaphragm might be spared in many cases. Third, MRI might detect asymptomatic trunk muscle lesions with high sensitivity.
In IIMs, patients generally receive immunotherapy with corticosteroid. Some of our findings may be related to corticosteroid treatment. In patients with relapsed ASS who received long-term corticosteroids (patients 3 and 4), patchy inflammation was observed with a wide distribution without involving the fascia. Such findings were not observed in de novo patients with ASS, which suggests that the pathological processes differ between the initial and recurrent phases under the influence of immunotherapy.
This study had several limitations. First, this was a single-institution study with a small sample. Second, the MRI findings of IIMs may be influenced by many factors, such as disease stage and treatment phase, which we could not control. Third, our WB-MRI method depends on semiquantitative evaluations based on visual inspection, so the results are not completely free of bias. More quantitative measures should be developed.
In conclusion, WB-MRI is sensitive in detecting muscles involved in IIMs, even in the absence of muscle weakness. The STIR sum score is positively correlated with peak serum CK level; therefore, it could be used as a biomarker of overall muscle inflammation. Our studies suggest that the subclinical inflammation of the trunk muscles was overlooked in some subtypes of IIMs. However, further research is required to establish objective and quantitative measurement methods and clarify the frequency of trunk muscle involvement based on WB-MRI in IIMs.
Footnotes
Author Contributions
Conceptualization: Nozomu Matsuda.
Data curation: Nozomu Matsuda, Kenji Yoshida, and Kazuaki Kanai.
Formal analysis: Nozomu Matsuda, Shunsuke Kobayashi, and Osamu Hasegawa.
Methodology: Nozomu Matsuda, Shunsuke Kobayashi, and Hitoshi Kubo.
Supervision: Yoshikazu Ugawa and Kazuaki Kanani.
Writing – original draft: Nozomu Matsuda and Shunsuke Kobayashi.
Writing – review and editing: Nozomu Matsuda, Shunsuke Kobayashi, Yoshikazu Ugawa, and Kazuaki Kanani.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the ethics committee of Fukushima Medical University Hospital (Approval number 2803) and conducted in compliance with the Declaration of Helsinki guidelines.