
Abstract
Background
Shoulder dislocation is a common injury, particularly in the younger population. Common long-term sequelae include pain, recurrence, and shoulder arthritis. Immediate and correct diagnosis following shoulder dislocation is key to achieving optimum outcomes. Although magnetic resonance arthrography (MRA) is frequently used for diagnosing shoulder instabilities, arthroscopy is still considered the gold standard.
Purpose
This study aims to compare the diagnostic value of arthroscopy and MRA of the shoulder joint.
Materials and methods
This retrospective study estimates the sensitivity and specificity of MRA of the shoulder. Data from patients who had undergone shoulder MRA and subsequent arthroscopy during a 5-year period were retrospectively collected. Sensitivity and specificity were calculated using the arthroscopic findings as the gold standard. Moreover, diagnostic accuracy was estimated using McNemar’s test.
Results
In total, 205 cases were included from which 372 pathological findings were uncovered during the arthroscopic procedures as opposed to 360 findings diagnosed from the MRA images. The glenoid labral tear was the most common finding reported by MRA and arthroscopy. For the detection of glenoid labral tears on MRA, the sensitivity was 0.955 but with eight missed lesions; the specificity was 0.679. Capsular tears, rotator cuff tears, and cartilage lesions proved the most difficult to correctly diagnose using MRA with sensitivities of 0.2, 0.346, and 0.366, respectively.
Conclusions
With a sensitivity of 95%, MRA is a valuable diagnostic tool for assessing shoulder instabilities, particularly when diagnosing labral lesions, including bony and soft-tissue Bankart lesions. Sensitivities and specificities for other glenohumeral lesions are less convincing, however.
Introduction
The glenohumeral joint has a higher degree of mobility than any other joint in the human body and may therefore be the most common of the large joints to dislocate and/or subluxate.1,2 The prevalence rate for traumatic shoulder dislocations is reported at 2% of which approximately 95% are anterior and 5% are posterior dislocations.3,4 For the younger and more active population, however, higher incidence rates of 3% have been suggested. 1
Instability following a dislocated glenohumeral joint is a commonly reported finding and can result in functional limitations and risk of recurrence. This is also reflected in patient-reported outcome studies, where shoulder instability has been associated with lower quality of life measurements. 1
Correct diagnosis and management are fundamental to successful recovery since immediate surgical stabilization, if indicated, may reduce the risk of re-dislocation. 3 The initial diagnosis of dislocation and subsequent reduction are traditionally made on radiographs. Osseous injuries such as impaction fractures of the humeral head (HillSachs lesions) and glenoid rim avulsions (Bankart lesions) may also be diagnosed on radiographs. More detailed visualization of osseous injury, ligamentous, capsular, and labral involvement can be obtained by computed tomography (CT) and/or magnetic resonance imaging (MRI). 1 MR arthrogram is an MRI preceded by intraarticular injection of a contrast media. An MRA is a minimally invasive procedure commonly used to assess shoulder instability.5,6 MRA has been reported to be more sensitive than standard MRI when diagnosing shoulder disorders.7,8 Despite the increased use of MRA, the arthroscopic procedure is still considered the gold standard for intraarticular shoulder pathologies.9,10 The overall advantage of arthroscopy is its therapeutic potential during the procedure. Conversely, arthroscopy is more invasive than MRA and is therefore associated with more potential complications also because it (arthroscopy) requires general anesthesia. 11
The overall aim of this study was to explore the diagnostic value of MRA of the shoulder using arthroscopy as a reference standard. The objectives were to estimate the sensitivity and specificity of MRA-diagnosed pathologies of the shoulder.
Materials and methods
This retrospective diagnostic accuracy study on patients with shoulder conditions was approved by the Danish Data Protection Agency (20/46309). Patients who had obtained an MRA of their shoulder during a 5-year period from September 2015 to September 2020 were eligible for inclusion. Patients were excluded if a follow-up arthroscopy was not performed or if the time span between the MRA and the arthroscopic procedure exceeded 6 months. Patients with prior shoulder surgery were also excluded.
Data on age, sex, and pathological findings as stated in the radiology report were retrospectively collected. Pathological findings diagnosed during the arthroscopic procedure were obtained from the surgical notes. For the purpose of this study, the arthroscopic findings were defined as the reference standard.
MRA procedure
Definitions of MRA sequences.

AP: anterior–posterior; LR: left-right; N/A: not applicable; HF: head-feet; FH: feet-head; RL: right-left.
An example of a commonly diagnosed pathological finding on the MRA images is an osteochondral tear (Figure 1). MRI T1 Dixon transversal image showing an anterior osteochondral tear in the labrum of the right shoulder.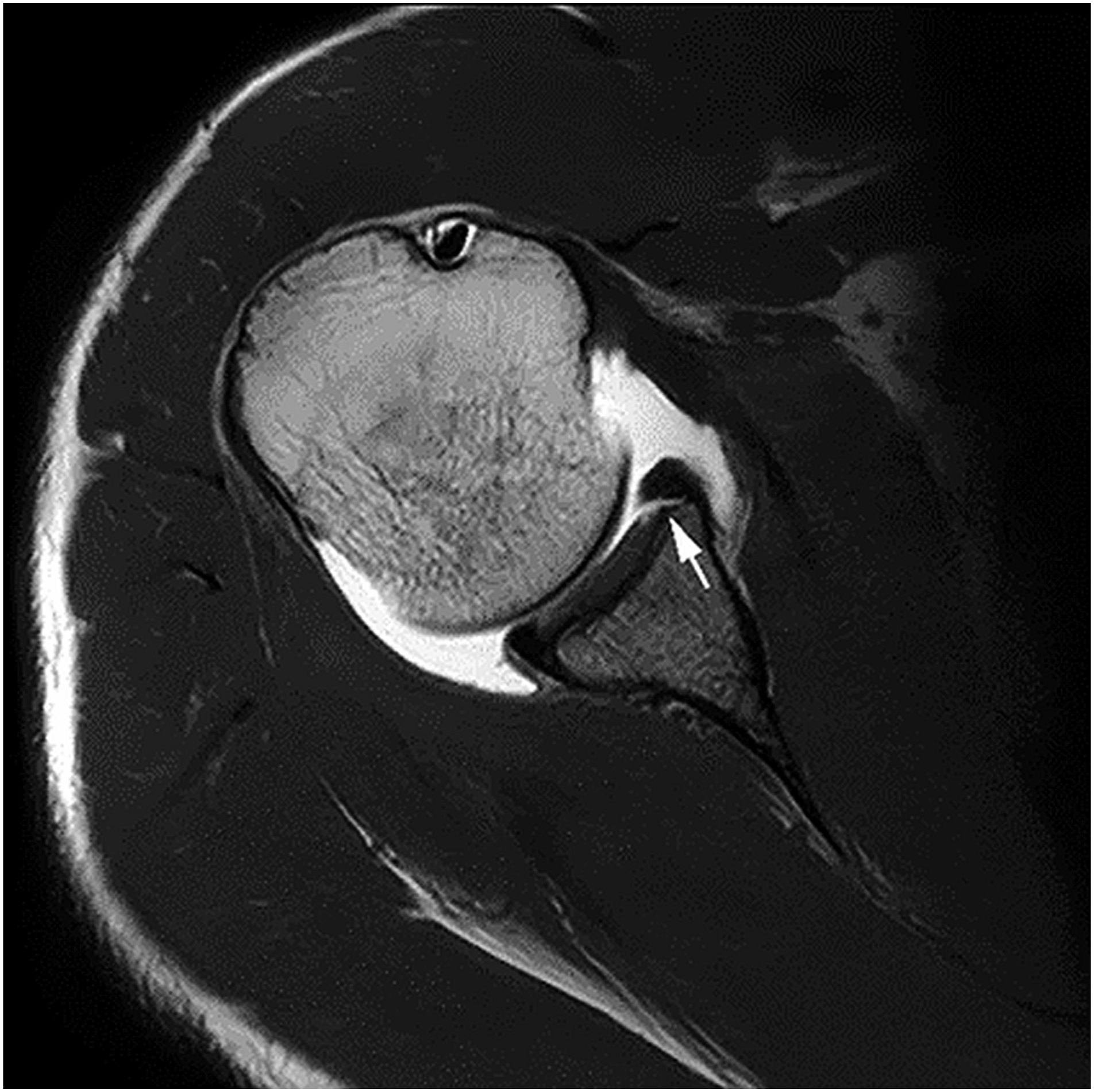
Shoulder arthroscopy technique
The arthroscopies were performed in the beach chair position, with posterior access. The posterior portal was at the soft spot, approximately 2 cm medial and 2 cm distal to the posterior lateral border of the acromion. For visualization of tears and lesions, the glenohumeral joint was expanded with an inflow of isotonic saline. The joint was then systematically examined for tears and lesions. The procedure was performed in general anesthesia using a scope (Stryker, Kalamazoo, Michigan, USA). The arthroscopic procedures were undertaken by three highly skilled consultant orthopedic shoulder surgeons, all with more than 20 years of experience.
Statistical analysis
The arthroscopic findings were defined as the reference standard for the purpose of all statistical analyses. Sensitivity and specificity were calculated for all included types of lesions. McNemar’s test was used to estimate the diagnostic accuracy of MRA. Statistical significance was set at p < 0.05. The STATA version 16 (StataCorp. 2019, Texas) was used for all statistical analyses.
Results
Patient demographics
A total of 870 patients had undergone shoulder MRA during the 5-year inclusion period. Of these, 320 patients subsequently underwent arthroscopic procedures. Forty-three patients were excluded as they had undergone previous shoulder surgery, and 72 patients were excluded because the time span between MRA and arthroscopy exceeded 6 months. Out of the 870 examinations eligible for inclusion, 205 were ultimately included. Flowchart of inclusion/exclusion is depicted in Figure 2. Flowchart of the data collection according to inclusion and exclusion criteria.
Sixty-two patients were female (30%) and 143 were males (70%). Mean age was 28.7 years (range: 16–70 years). Mean time from MRA to arthroscopy was 2 months and 24 days, ranging from 10 days to 5 months and 28 days.
Pathological findings
Findings of arthroscopy and MRA. Patients in total, n = 205.

aIncluding Bankart lesions.
FP: false positive; FN: false negative; SLAP: superior labrum anterior to posterior lesions.
p-value McNemar’s test. Sensitivity and specificity calculated using arthroscopy as the reference standard.
Discussion
Using arthroscopy as the reference standard, the current study estimated diagnostic accuracy including sensitivity and specificity of MRA for the following lesions: glenoid labral tears (incl. Bankart lesions), cartilage lesions, SLAP lesions, rotator cuff tears, capsular tears, and HillSachs lesions.
In keeping with previous studies, the most prevalent finding in the current study was the glenoid labral tear. Previously, prevalence rates of 87–100% for labral tears have been reported.12,13 Within the current study population, the prevalence rate for glenoid labral tears was 86%. Arthroscopy and MRA, respectively, diagnosed 177 and 178 glenoid labral tears. The similar number of labral tears diagnosed by MRA and arthroscopy suggested that there was no significant difference in diagnostic accuracy between the two methods when diagnosing glenoid labral tears (p = 1). This does not, however, reflect the entire truth. Although MRA exhibited a sensitivity of 0.955, nine labral tears found during subsequent arthroscopy were not diagnosed on the MRA images. Moreover, MRA diagnosed eight patients with a glenoid labral tear that subsequently proved to be false positives during the arthroscopic procedure.
Correctly identifying capsular tears, rotator cuff tears, and cartilage lesions proved difficult on MRA images with sensitivities of 0.2, 0.346, and 0.366, respectively. The anatomically close relation between the labrum and the cartilage layer in the shoulder joint might explain this discrepancy between MRA and arthroscopy.
Indications for surgery can be first-time dislocations by physically active young patients and patients with recurrent dislocations or complex injuries. Timely diagnosis and intervention may, however, prevent persistent symptoms and recurrent instability. 1 As an example, misdiagnosed tears in the rotator cuff tendons may lead to prolonged periods of symptoms and/or disability. 14 Bearing in mind that MRA diagnosed only 35% of all rotator cuff tears, approximately 72% of the HillSachs lesions, and almost 37% of the cartilage lesions, the MRA should probably not be the primary tool for diagnosing shoulder instabilities based on our data. This finding is supported by Jonas et al. 11 who even put forward the idea of possibly reducing the use of MRA, at least until improved imaging techniques which can increase the diagnostic accuracy of MRA become available.
Compared to MRA and arthroscopy, ultrasound of the shoulder is a non-invasive relatively low-cost examination that may also be valuable in relation to shoulder instabilities. 15 Compared to MRA however, ultrasound has shown slightly lower sensitivities and specificities in the detection of rotator cuff tears though. 16 This may in part be explained by the operator dependency associated with an ultrasound examination. It has been suggested, though, that ultrasound is valuable for pathologies of the rotator cuff and that MRA could be used when ultrasound does not provide the diagnosis. 17 Prospective studies examining sensitivity and specificity of ultrasound using shoulder arthroscopy as the gold standard would be beneficial in the evaluation of ultrasound in relation to shoulder instabilities.
An inherent limitation of this study is the retrospective design, which meant that the MRA radiology reports were accessible to the orthopedic surgeon prior to the arthroscopic procedure. This could have introduced bias into the results since the surgeon was able to look specifically for the pathological findings mentioned in the radiology report. The time span ranging from 10 days to almost 6 months is another limiting factor since lesions may dissolve or be less perceptible during the 6-month period. The possibility of new lesions occurring during the period from MRA to arthroscopy cannot be excluded either. Moreover, it has been suggested that the accuracy of the MRA radiology report is observer-dependent, with experienced radiologists being more accurate. 10 In the current study, three dedicated and experienced musculoskeletal radiologists performed the MRA procedures and the subsequent reports. The radiology reports in the current study were therefore made by specialists and are presumably of high diagnostic quality and thus do not likely explain the inconsistencies shown between MRA and arthroscopy.
In conclusion, with a sensitivity of 95%, MRA is an important diagnostic tool for assessing shoulder instabilities, particularly when diagnosing labral lesions, including bony and soft-tissue Bankart lesions. In view of the results, MRA as a first-line modality in suspected shoulder instability is considered a very valuable diagnostic tool. Sensitivities and specificities for other glenohumeral lesions are, however, less convincing. Further studies, preferably prospective and blinded in design, are needed to evaluate the overall diagnostic accuracy of MRA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.