
Abstract
Background
Magnetic resonance imaging (MRI) is used far less as an imaging-guided method for percutaneous biopsies than computed tomography (CT) and ultrasound (US), despite its imaging benefits, particularly in children.
Purpose
To evaluate the feasibility, accuracy and safety of MRI-guided biopsies in paediatric patient population.
Material and Methods
The retrospective study included 57 consecutive paediatric patients (<18 years old). A percutaneous core needle biopsy (PCNB) or trephine biopsy was performed in 53 cases, and an additional fine-needle aspiration biopsy (FNAB) in 26 cases. In 4 cases, a stand-alone FNAB was taken. Biopsies were performed with 0.23 T open and 1.5 T closed MRI scanners. Statistical methods used for confidence intervals and p-values were Wilson score method and chi-square test.
Results
The overall diagnostic accuracy of histologic biopsy was 0.94, with sensitivity 0.82, specificity 1.00, positive predictive value (PPV) 1.00 and negative predictive value (NPV) 0.92. In histological bone biopsies, diagnostic accuracy was 0.96, with sensitivity 0.86, specificity 1.00, PPV 1.00 and NPV 0.94. The FNAB sample diagnosis was associated with the histological diagnosis in 79% of cases. There were no major primary complications and only a few late complications. After biopsy, 83% of the children were ambulatory in 6 h. Anti-inflammatory drugs and paracetamol provided satisfactory pain relief in 96% of the patients after biopsy. Most outpatients (71%) were discharged from hospital either on the same day or 1 day later.
Conclusion
MRI is a technically feasible, accurate and safe guidance tool for performing percutaneous biopsies in children.
Introduction
In the past, open biopsy or surgery has been the preferred method to obtain histopathologic diagnoses of suspicious masses in children. 1 With image guidance, biopsies and procedures can be performed considerably less invasively than through open surgery.2,3 The potential complication risks associated with image-guided biopsies and open surgery do not significantly differ. 4 For children, despite its imaging benefits, magnetic resonance imaging (MRI) is far less used for image-guided percutaneous biopsies or as an intervention method than computed tomography (CT) and ultrasound (US). The advantages of MRI are excellent spatial and contrast resolution especially in soft tissue, good flow detection, multiplanar imaging and no radiation. MRI is well suited for the planning, guidance and monitoring of diagnostic and therapeutic procedures.2,5 For children, ALARA (As Low As Reasonably Achievable) is a crucial principle that aims to minimise radiation exposure. One main limitation of interventional MRI is the powerful magnetic field involved; all instruments and equipment must be compatible with the MRI environment. Other limitations are a longer procedure time due to the relatively long imaging time, higher costs and the limited availability of MRI scanners. Moreover, a closed bore MRI does not allow direct patient access during imaging. Implants can be contraindications and cause artefacts but are rarely a problem with children.2,5,6
With children, most studies on image-guided biopsies have focused on CT and US guidance.7–21 There are few publications on MRI-guided biopsies in children and published patient series are small (range 1–13 cases).4,22–25 The accuracy of MRI-guided bone biopsies correlates with open and CT-guided biopsies. 26 However, to our knowledge, there is only one study in adults that reported accuracy of MRI-guided bone biopsies in a larger population. 27
The purpose of this study was to evaluate the feasibility, accuracy and safety of MRI-guided biopsies in paediatric patient population.
Materials and Methods
Patients
This retrospective study was approved by the institutional ethical board and consisted of 57 consecutive paediatric MRI-guided percutaneous biopsies performed from May 1999 to November 2016. Inclusion criteria were: (1) age less than 18 years; (2) unconfirmed and possibly neoplastic bone or soft tissue lesion detected in a previous radiograph, US, CT, MRI, bone scan or combination of these modalities. Eight of 57 children had a known primary malignancy. Of these 8, seven were symptomless and with a stable follow-up phase. The patients’ age ranged from 3 months to 17 years (mean 12.2 years), with 32 girls and 25 boys. In 18 of 57 cases, the biopsy was taken during an MRI-guided therapeutic procedure of a bone lesion to ensure benignity. Patients with implants or medical hardware preventing the use of MRI as a guidance method were excluded.
Anatomical locations of target lesions.

aA liver lesion, two pancreas lesions.
bA synovia of the knee, a popliteal lymph node, a tumour of the nape, a tumour of the piriformis muscle, a parapedicular soft tissue lesion, a soft tissue thickening around the periosteum.
Equipment
A 0.23 T open and a 1.5 T closed MRI scanner were used. Both scanners enabled real-time or near-real-time imaging during the biopsy and procedural control was achieved by taking images before and after moving the instrument.
Four different calibres of MRI-compatible trephine biopsy sets (2, 3, 4 and 6 mm) were used in bone biopsies. In recent years, a 4 mm set has been standard (Figure 1). A soft tissue PCNB was performed with a 12- to 18-gauge (G) needle. Instrumentation for MRI-guided bone biopsy (4 mm set). From left to right: 20-G puncture needle, needle and syringe (21 G/10 mL) for local anaesthetic, syringe for gadolinium-contrast agent (for skin entry point marking), manual spiral drill, two different kinds of cavity drill (one with ejector), trocar and mandrin for bone entry and top crosswise, a hammer. Note: MRI: magnetic resonance imaging.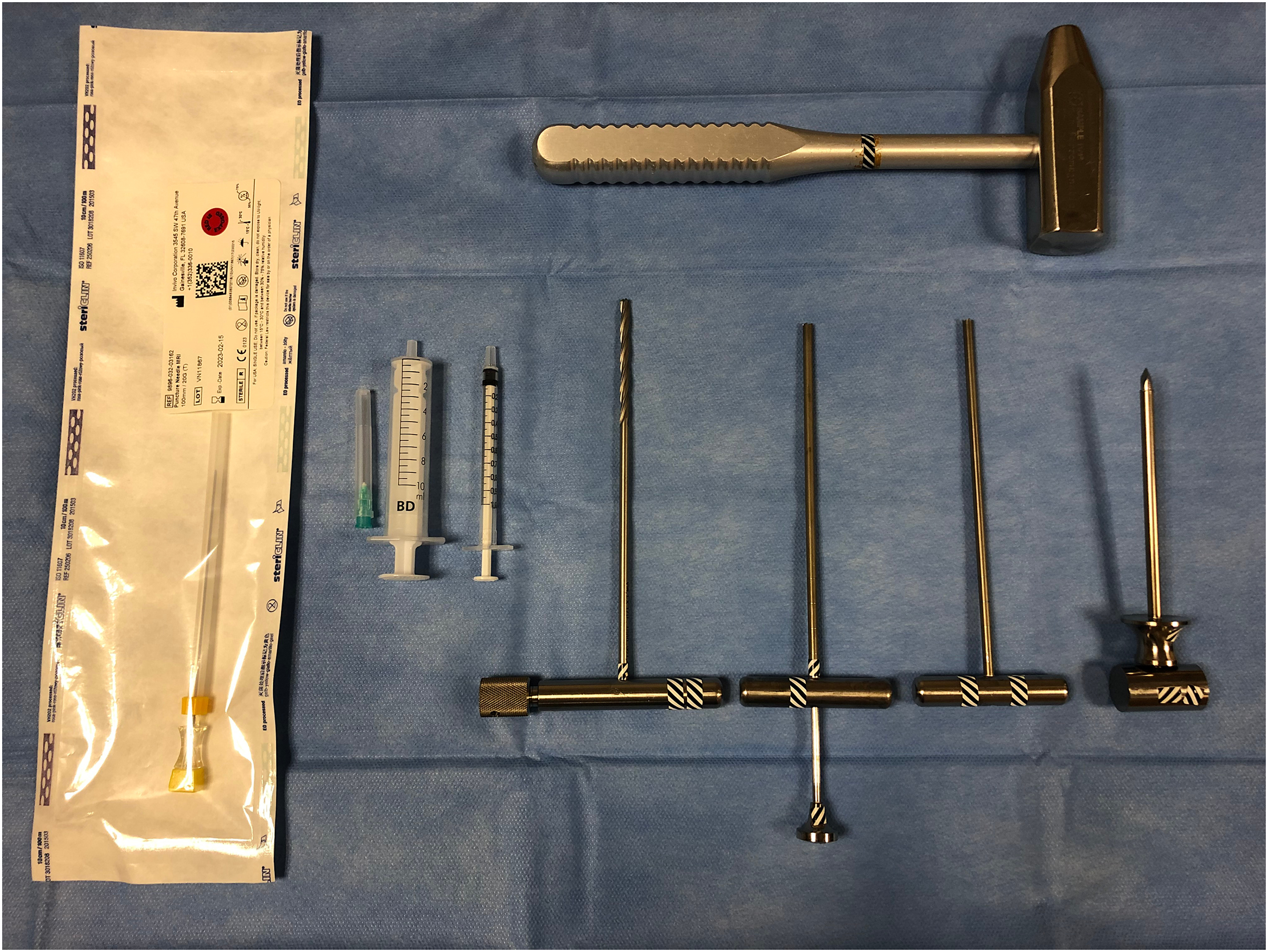
FNAB was performed through an MRI-compatible coaxial needle set with MRI-compatible 18- to 20-G needles. Part of the FNABs were combined with a trephine biopsy/PCNB; here, a semi-automated MRI-compatible true-cut needle and MRI-compatible coaxial needle were used.
Procedure
Open MR imaging sequences used.

Closed MR imaging sequences used.

Before the biopsy, the entry point on the skin was localised. Antiseptic skin preparation, skin coverage and safety issues were completed. The biopsy route and the entry point were determined by placing the tracker-mounted instrument26,28 or gadolinium-filled syringe close to the skin
2
and evaluating the marker, target and route from consecutive images before entry. Local anaesthetic (usually lidocaine) was infiltrated intra- and subcutaneously. Through a skin incision, the coaxial needle was advanced to the region of interest with the help of the instrument-generated susceptibility artefact (Figure 2). The trocar and mandrin were removed from the coaxial cannula after target contact and samples were collected. If necessary, a manual MRI-compatible spiral drill (In Vivo Corporation, Gainesville, USA) was used in deeper targets for bone channelling before the actual biopsy. Soft tissue lesions were biopsied with a semi-automated MRI-compatible side-cutting biopsy gun (In Vivo Corporation, Gainesville, USA and Somatex, Berlin, Germany). Bone biopsies were taken with a cylindrical trephine (In Vivo Corporation, Gainesville, USA). The biopsy was repeated if the sample seemed macroscopically insufficient. In cases of PCNB or trephine biopsy, the combined FNAB was aspirated through the cannula after the initial biopsy. A stand-alone FNAB was taken in a similar manner through a smaller diameter coaxial needle. MRI-guided biopsy of a well-defined lesion located in the distal femur just below the epiphyseal plate. On the left side, coronal plane (T1 TSE) and on the right side, axial plane (T1 TSE). The thicker arrow points to the tip of the biopsy needle (including trocar and mandrin) and the thinner arrow to the biopsy target, which is 1.5 cm in diameter. The lesion was an enchondroma. Note: MRI: magnetic resonance imaging; TSE: turbo spin echo.
There was no pre-established practice in the use of prophylactic antibiotics. Altogether, 14 (24.6%) cases received prophylactic antibiotics; all were bone biopsy cases. No contrast agent was used during the biopsies.
The choice of anaesthesia method was made by the anaesthesiologist in collaboration with a radiologist. All but two procedures were performed under general anaesthesia; there was one spinal and one local anaesthesia. All biopsies were performed by experienced interventional radiologists.
Outcome variables
Feasibility was evaluated by recognising any technical challenges during biopsy and by analysis of the needle and procedure time.
Biopsy accuracy was determined by using the histopathological diagnosis as a reference for the final diagnosis. The final diagnosis was based for all patients on imaging findings, MRI-guided biopsy and possible re-biopsy results, possible surgical biopsies and extirpations, follow-ups and clinical findings. The diagnostic relevance of the MRI-guided biopsy result was compared to the final diagnosis after follow-up. Based on the follow-up, the biopsy results were classified as true positive (TP), true negative (TN), false positive (FP) or false negative (FN). Considering all the biopsies, the minimum follow-up was 3 months (range 1 month–11 years). All samples were classified as either diagnostic or non-diagnostic, and a specific histopathological diagnosis was set by a pathologist. In cases where histopathology of primary or repeated biopsies showed no signs of malignancy or infection and remained partially non-specific despite the technical success of the biopsy procedure and sampling, the biopsy results were classified as diagnostic for a benign lesion, as long as no evidence of malignancy or infection was found during the follow-up or surgery.
Technical observations took into account the mean lesion diameter, size of the needle tip artefact, number of passages and post-procedural recovery. The need for additional biopsies was also reported.
Safety evaluation was based on adverse events.
Statistical method
The data of diagnostic performance are given as numbers of TP, TN, FP and FN. Diagnostic accuracy statistics (sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), diagnostic accuracy (DA)) with their 95% confidence intervals were calculated for each finding. The confidence intervals were calculated using Wilson score method without continuity correction. The p-values were calculated with chi-square test.
Results
Feasibility
The histological sampling was successful in every case, but in eight of 53 (15.1%) cases, there were some technical challenges. In two soft tissue lesions, technical challenges were related to the small size and rubber-like matrix of the lesion. In five bone lesions, the sclerotic hardness of a lesion, mild bleeding from the drill tract, poor distinctiveness of the nidus in a sclerotic lesion, limited steering properties of the drill regarding to the target and shape of the focus (patella) caused some technical challenges. In one case, a small piece of drill edge was lodged inside the bone lesion but was easily removed with the extension of the tract. In all 30 FNAB cases, the sampling was successful, although the small size of the lesion in one case caused a technical challenge.
PCNB and trephine biopsy time differences with and without technical challenges.

PCNB = percutaneous core needle biopsy.
Thirty FNABs were taken and in 26 of them, FNAB was combined with histological sampling. The needle time range was 10–40 min (mean 19.5 min, SD ± 14.0 min) when a stand-alone FNAB was performed, and 4–141 min (mean 49.7 min, SD ± 34.2 min) when FNAB was combined. The procedural time range in these groups was 32–61 min (mean 40.0 min, SD ± 14.0 min) and 7–164 min (mean 66.1 min, SD ± 38.0 min), respectively.
Accuracy
Fifty-one of 53 (96.2%) PCNBs and trephine biopsies were diagnostic. Twenty-four of 30 (80.0%) FNABs were diagnostic. Two of four samples were non-diagnostic in cases where only FNAB was taken. In two of 26 cases, where both PCNB/trephine biopsy and FNAB were taken, both histological and cytological samples were non-diagnostic, both soft tissue lesions. In 19 of the remaining 24 (79.2%) cases, the histology and cytology corresponded. In two of 5 cases where there was no correspondence, the PCNB/trephine biopsy was diagnostic, and the FNAB was undiagnostic.
Diagnostic performance of MRI-guided bone and soft tissue biopsies.

PCNB = percutaneous core needle biopsy, FNAB = fine needle aspiration biopsy, NOB = number of biopsies, N-D = non-diagnostic, TP = true positive, TN = true negative, FP = false positive, FN = false negative, PPV = positive predictive value, NPV = negative predictive value, DA = diagnostic accuracy, CI = confidence interval.
List of specific histopathological diagnoses.

aPost-traumatic lesions.
Technical observations
The mean lesion diameter + standard deviation (SD) was 3.8 cm ± 4.1 cm (range 0.3–19 cm). Five children underwent two biopsies; these were counted as individual biopsy cases.
The size of the needle tip artefact was typically 2–4 mm.
Forty-eight of 53 (90.6%) PCNBs or trephine biopsies were performed with one passage. When ignoring PCNBs of the soft tissue, 43 of 45 (95.6%) bone biopsies were performed with one passage.
Forty-seven of 57 (82.5%) children were ambulatory after a two- to 6-h post-biopsy rest.
Excluding nine children who needed intensive hospitalisation at the time of biopsy due to their severe clinical condition, mean hospital time in the outpatient group was 2 days (range 1–6 days, SD ± 1.07 days), including the biopsy day. Thirty-four of 48 (70.8%) outpatients were discharged from the hospital either on the same day or 1 day after the procedure. Forty-six of 48 (95.8%) outpatients needed only anti-inflammatory drugs and paracetamol for post-biopsy pain relief.
Additional biopsies
A repeated image-guided biopsy was needed in 2 cases, a surgical open biopsy in 4 cases and a surgical extirpation in 5 cases. In two of four surgical open biopsies and in three of five surgical extirpation cases, surgery provided additional information (confirmation of diagnosis).
Four cases led to surgical open biopsy; two were soft tissue and two bone lesions. Of soft tissue lesions, one was a tumour of the nape, where both histological and cytological MRI-guided biopsy samples suggested a benign hamartomatous or cartilaginous tumour. In this case, a surgical open biopsy did not provide additional information and diagnosis was confirmed in surgical extirpation (benign hamartomatous tumour). The second was a soft tissue thickening around the periosteum in suspected osteomyelitis of a toe where a histological bone biopsy was not technically possible (bone diameter 3 mm) and the MRI-guided cytological sample was non-diagnostic, a surgical biopsy confirmed the diagnosis of osteomyelitis. Of bone lesions, the first was a case of osteomyelitis where diagnosis was initially reached with MRI-guided biopsy (histological sample) but faster analysed cytological sample was non-diagnostic leading to surgery where the diagnosis of osteomyelitis was confirmed. The other was a case where MRI-guided histological and cytological samples suggested a benign lesion and diagnosis was confirmed in surgery (myofibromatosis).
Two of the five lesions that led to surgical extirpation were bone biopsy cases. In both cases, MRI-guided biopsies provided diagnoses (osteoid osteoma), but extirpation was performed for therapeutic purposes. The remaining 3 cases that led to surgical extirpation were soft tissue lesions. One was a lesion of the nape, described in more detail above. One was a PCNB (MRI-guided) missed malignancy of the pancreas (metastasis of nephroblastoma), which turned out to be a suspected malignancy in FNAB (MRI-guided) and surgery confirmed malignancy. The third was a case of thickened synovia of the knee; MRI-guided histological and cytological samples were diagnostic, but operative decision led to extirpation of the lesion and confirmed the benign diagnosis.
Safety
There were no major primary complications and only two later-stage complications; a pathologic fracture appeared 7 days after femoral biopsy (a bone marrow filling enchondroma), and cellulitis 8 days after an ulnar biopsy (osteomyelitis).
Discussion
This study shows that MRI-guided biopsy is a feasible, accurate and safe guidance method in paediatric patient population to determine the nature of bone and soft tissue lesions. In our study, histological and cytological sampling was successfully performed in every case. Biopsy complications were rare. Also, the immobilisation and discharge time after the procedure was short.
In our opinion, our results highlight the potential utility and safety of MRI guidance in performing these sometimes complex procedures in children and adolescents.
The results of our study are line with previous US-, CT and MRI-guided studies in paediatric population.4,7–25 Fritz et al. 22 reported mean MRI-guided trephine biopsy length 77 min and Schulz et al. 25 estimated overall MRI-guided procedural time to be roughly 60 min. In our study, the mean procedural time of a histological biopsy without any technical challenges was shorter (48 min). The results of this study are also in line with a previous MRI guidance study in an adult population; Kerimaa et al. 27 showed a 93% accuracy, 89% sensitivity, 98% specificity, 97% PPV and 91% NPV in histological bone and soft tissue biopsies. The results of our study were in concurrence to previous CT-guided bone biopsy studies in adults. Leffler and Chew 29 demonstrated an 82% PPV and 100% NPV in their CT-guided FNAB combined bone biopsy study. Tikkakoski et al. 30 reported in their CT-guided bone biopsy study 93% diagnostic and 84% exact diagnoses rates in trephine biopsy, with the same rates in FNAB were 97% and 90%. However, the percentage of malignant lesions was clearly higher than in our study. In non-malignant bone lesion cases, there are few tissue cells but blood in the trephine biopsy channel where FNAB is collected; blood was the typical finding in non-diagnostic FNAB samples from bone in our study, too. Previous US- and CT-guided PCNB studies of soft tissue lesions in children show on average an 80–90% success rate for diagnosis.7–21 The soft tissue lesion results of our study are in line with previous US- and CT-guided studies, although an exact histopathological diagnosis was not always achieved. The low percentage of specific histopathological diagnoses (60.4%) of histological samples is probably explained, at least in part, by the small proportion of malignant lesions (n = 3), as the nature of benign lesions cannot always be specified exactly by histopathology. For example, in the case of osteomyelitis, where the histopathological finding is usually normal bone and the definitive diagnosis is based on culture analysis. Two of three patients with malignant biopsy results died during the follow-up. The remaining patient is alive after 11 years’ follow-up. Biopsy complications were rare, corresponding to US- and CT-guided studies in children.7–21 Fritz et al. 22 showed in their study that MRI guidance is an accurate and feasible biopsy method in children with chronic nonbacterial osteomyelitis. Their study focused on bone lesions which were visible on MRI but occult on CT. Koenig et al. 31 reported that MRI has slightly better visualisation of small bone marrow lesions than CT. Ueno et al. 24 had a similar result in their study, where a scintigraphy-positive bone lesion was depicted only in MRI and a subsequent MRI-guided biopsy revealed a bone marrow metastasis. These data indicate that especially in bone marrow cases, MRI may be the best possible guidance method option. In our material, all bone marrow lesions were detected in MRI. Smith et al. 23 reported in their MRI-guided liver biopsy study (n = 5) that MRI is an accurate, feasible and safe guidance method in children and young adults. We had only one liver biopsy case in our study; the biopsy was technically successful, including exact histological and cytological diagnoses.
US is the primary image-guidance technique for soft tissue lesion biopsies. It is particularly useful in targeting superficial lesions, but has limitations, primarily acoustic shadowing from gas and bone, which can effectively prohibit biopsy in bone and lung. The use of contrast-enhanced US as a guidance tool has been limited. 32 CT and, historically, fluoroscopy have been the primary guiding techniques for bone biopsies.7,30,33 The superimposing normal anatomical structures and the lack of volumetric data pose a challenge to the use of fluoroscopy. CT is currently regarded as the gold standard guidance method for bone biopsy.7,29,30,33 However, modalities utilising x-rays involve radiation exposure, and the use of CT has been found to increase lifelong cancer mortality in children. 34 US is inherently performed in real-time. Real-time guidance can also be achieved with CT and MRI, but it typically requires technical add-ons that can add the expenses of the procedure. Needle artefact size in MRI guidance is larger than in CT guidance. However, beam hardening artefact in CT also limits the visibility of the needle tip. In this study, the size and attributes of the instrument-generated susceptibility artefact were similar to previous reports.35–37 There were no issues with artefact asymmetry or blooming. When possible, the image readout phase was adjusted to be parallel with the biopsy needle to minimise the artefact and possible blooming effect. Regardless of the guiding modality, children’s biopsies usually require general anaesthesia.
It has been shown that in some cases of musculoskeletal tumours, the use of gadolinium-contrast media may be useful in tumour targeting. 38 We did not use the contrast media during biopsies, and we did not experience any significant negative effect on biopsy efficacy. However, the ability to target a viable part of the tumour can be of advantage. In the future, positron emission tomography (PET-CT and PET-MRI) guidance may enable biopsies from the most metabolically active part of the lesion but the associated ionising radiation is a disadvantage. 8
In bone biopsy cases, it seems reasonable to combine FNAB with a histological biopsy .29,30 Often, initially non-diagnostic findings necessitate a repeated biopsy. 39 In our material, the repeated image-guided biopsy did not provide additional information.
Our study is one of the few studies that provides insight and information on performing MRI-guided biopsies in a larger set of paediatric patients. This study has some important clinical and pathophysiological implications that is confirmatory to previous literature. The present research supports the idea that bone biopsy with MRI guidance is an alternative to CT guidance in paediatric population. For soft tissue targets, MRI is a useful option when US’s limitations prohibit its use. CT is associated with ionising radiation and it is our view that the ALARA principle should be extended to performing paediatric biopsies, here MRI guidance could have a role. One obstacle to the generalisation of MRI use as a guidance method has been its higher costs compared to other modalities, although lower than open biopsy costs.40–44 Nevertheless, the economic arguments should not be the only consideration in utilising new medical innovations. We suggest that MRI guidance is useful as an added tool in large tertiary centres when planning the diagnostic management of paediatric patients with bone or soft tissue lesions requiring biopsy.
This study has limitations. First, the study comprises a retrospective patient series of consecutive paediatric patients without a control group. Second, the number of biopsies was still relatively small. The number of soft tissue biopsies was also limited and the number of diagnosed malignancies was low (n = 3). Moreover, only a few cases ended up with surgical open biopsy (7.0%) or extirpation (8.8%), and due to this, the direct comparison between MRI-guided biopsy and surgery obtained diagnoses was not possible in most cases.
In conclusion, MRI-guided percutaneous biopsy is a feasible, accurate and safe guidance method in paediatric cases requiring biopsy. However, further randomised and prospective studies in children comparing the accuracy of MRI-guided biopsy to that of other imaging-guided modalities are still needed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.