
Abstract
Craniopharyngiomas are benign neoplasms with two histological subtypes: adamantinomatous and papillary. Papillary craniopharyngiomas are rare in children, and those with a pituitary abscess within are even rarer. Herein, we present the case of a 14-year-old boy with a papillary craniopharyngioma and a coexisting intratumoral abscess, who was hospitalized for persistent pyrexia, polyuria, and polydipsia. The absence of calcification on computed tomography, high signal intensity inside the tumor on diffusion-weighted imaging, and clinical findings such as fever, a high inflammatory response, and meningitis, as well as short-term morphological changes on imaging, could aid in diagnosis.
Keywords
Introduction
Craniopharyngiomas are benign neoplasms (World Health Organization [WHO] grade I) that typically arise in the sellar to suprasellar regions. 1 They account for approximately 1–5% of the primary brain tumors in patients of all ages. 1 In Japan, craniopharyngiomas are the fourth most common (10.6%) pediatric brain tumors. 2 They have two histological subtypes 1 : the adamantinomatous subtype accounts for most pediatric cases, while the papillary subtype is diagnosed almost exclusively in adults 3 and is rare in children. 4
Pituitary abscesses are rare 5 and are either primary (developing de novo inside a normal pituitary gland) or secondary (forming within a diseased gland, such as a pituitary adenoma and a Rathke’s cleft cyst). 6 Secondary pituitary abscesses are hypothesized to be caused by tumors that disrupt the local blood circulation and impair the immune response, which in turn disrupt the control of infection. Furthermore, these tumors may have necrotic areas, which can make them more susceptible to infections. 7 While few adult cases presenting with an abscess inside a craniopharyngioma have been reported,5,6,8–12 no pediatric case has been reported yet.
Herein, we report a case of a pediatric patient with a histopathologically confirmed papillary craniopharyngioma with a coexisting intratumoral abscess. We demonstrate its rarity through a review of the literature and compare the radiological findings of papillary craniopharyngiomas and pituitary abscesses between children and adults.
Case report
A 14-year-old boy was referred to our hospital for a 2-month history of polydipsia and polyuria; for 1 month before presentation, he had experienced persistent fever, worsening polyuria, and worsened polydipsia causing nocturnal urination and insomnia. He was diagnosed with diabetes insipidus. The clinical symptom comprised bitemporal hemianopia, with no other obvious neurological abnormalities. While he had a history of treatment for frontal sinusitis, there was no relevant family medical history.
Computed tomography (CT) revealed a 31 × 22 × 20-mm heterogeneously enhancing mass extending from the sella turcica to the suprasellar region. The sella turcica was slightly enlarged by the mass, and its floor had thinned. No calcification was observed in the mass (Fig. 1). He had sinusitis in his frontal and maxillary sinuses (not shown), but his sphenoidal sinus was clear (Fig. 1). Non-contrast axial CT reveals the cystic mass in the suprasellar region. There is no calcification in the tumor (a; arrow). After contrast administration, an irregular ring-like enhancement is seen (b; arrow). Contrast-enhanced sagittal CT reveals that the sella turcica is slightly enlarged by the mass and its floor is thinned (c; arrow). CT: computed tomography.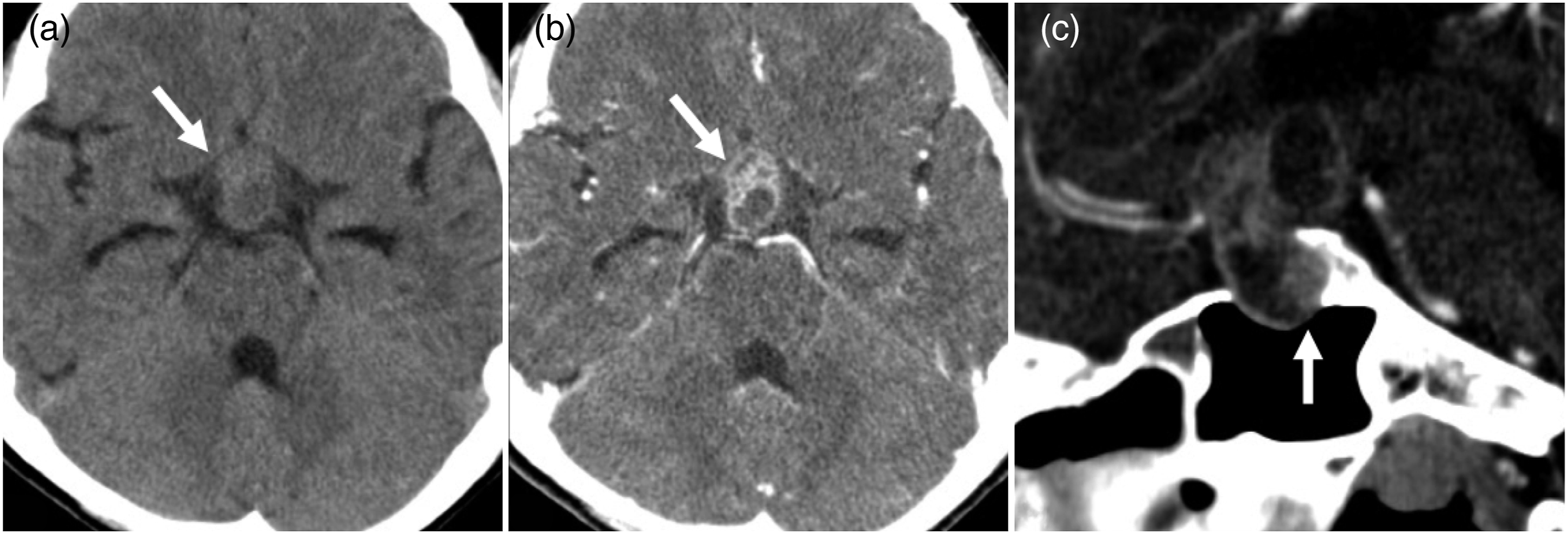
Magnetic resonance imaging (MRI) identified a 29 × 25 × 21-mm heterogeneously enhancing mass with cystic components mainly in the sellar to suprasellar regions (Fig. 2). T1-weighted imaging (T1WI) and T2-weighted imaging (T2WI) revealed a mass with heterogeneous signals (mixed high and low intensity signals). The optic chiasm was squeezed upward and thinned due to the mass. Post-contrast fluid-attenuated inversion recovery images showed wall enhancement in the left lateral ventricle and the third and fourth ventricles, indicating ventriculitis. Hydrocephalus was also observed. Diffusion-weighted imaging (DWI) showed a partially high signal intensity area in the mass. The minimum apparent diffusion coefficient (ADC) in the cystic area was 0.66 × 10−3 mm2/s. Follow-up MRI revealed an obvious increase in size after 2 weeks. Germinoma, Rathke’s cleft cyst, pituitary adenoma, pituitary xanthogranuloma, and Langerhans cell histiocytosis were considered as the differential diagnoses. However, because this case was of a tumor with a cystic and solid component, craniopharyngioma was suspected from the high frequency. Based on the restricted diffusion and short-term increase in size, we diagnosed the patient with an abscess within the craniopharyngioma. However, due to the patient’s young age, we expected an adamantinomatous type and not a papillary type. On non-contrast axial T1WI, the mass shows a heterogeneous signal intensity. The optic chiasm is squeezed upward and thinned due the effect of the mass (a; arrow). On contrast-enhanced axial T1WI, the mass shows an irregular ring-like enhancement (b; arrow). On DWI with b = 1000 s/mm2, the mass shows a high signal intensity (c; arrow), and the ADC value of this area is 0.66 × 10−3 mm2/s (image not shown). Contrast-enhanced FLAIR image shows wall enhancement of the 3rd (d; arrow) and left lateral ventricles (d; arrowhead), indicating ventriculitis. Contrast-enhanced sagittal T1WI reveals a heterogeneous enhancing mass with cystic components mainly in the sellar to suprasellar regions (e and f; arrows). A dorsal cystic component becomes more enlarged (e; arrowhead) as compared to 2 weeks earlier (f; arrowhead). ADC: apparent diffusion coefficient; DWI: diffusion-weighted imaging; FLAIR: fluid-attenuated inversion recovery; T1WI: T1-weighted imaging.
An emergency surgery was performed via the transsphenoidal approach for the parasellar tumor with an abscess. The dura mater of the sella turcica was incised, and pus was drained from the tumor. A papillary solid component was observed in the deep part; this was biopsied, and histopathological analysis confirmed the diagnosis of a papillary craniopharyngioma. Due to the presence of meningitis and ventriculitis, the initial surgery was limited to abscess drainage and biopsy to avoid surgical adhesions and cerebrospinal fluid leakage. After the inflammation was improved with antibiotic treatment for 1 month, the residual tumor was totally resected during a second surgery.
Histopathological findings revealed a squamous epithelium abutting a fibrocollagenous stroma arranged in a sheet pattern (Fig. 3). Neither wet keratin nor calcification was observed. Immunohistochemistry revealed positive staining for the B-Raf proto-oncogene, serine/threonine kinase (BRAF) V600E, but not for nuclear translocation of β-catenin. Immunopositivity for Ki-67 in the squamous cells was largely restricted to the basal layer. No obvious abscess was noted due to the abscess drainage and antibiotic treatment. These features were compatible with the diagnosis of a papillary craniopharyngioma. H&E staining section shows a squamous epithelium abutting on a fibrocollagenous stroma arranged in a sheet pattern. Neither wet keratin nor calcification is present (a, b). On immunohistochemistry, β-catenin (c) is negative for nuclear translocation, but BRAF V600E is positive (d). No obvious abscess is noted because the specimen has been collected after abscess drainage and antibacterial treatment. BRAF: B-Raf proto-oncogene, serine/threonine kinase; H&E: hematoxylin and eosin.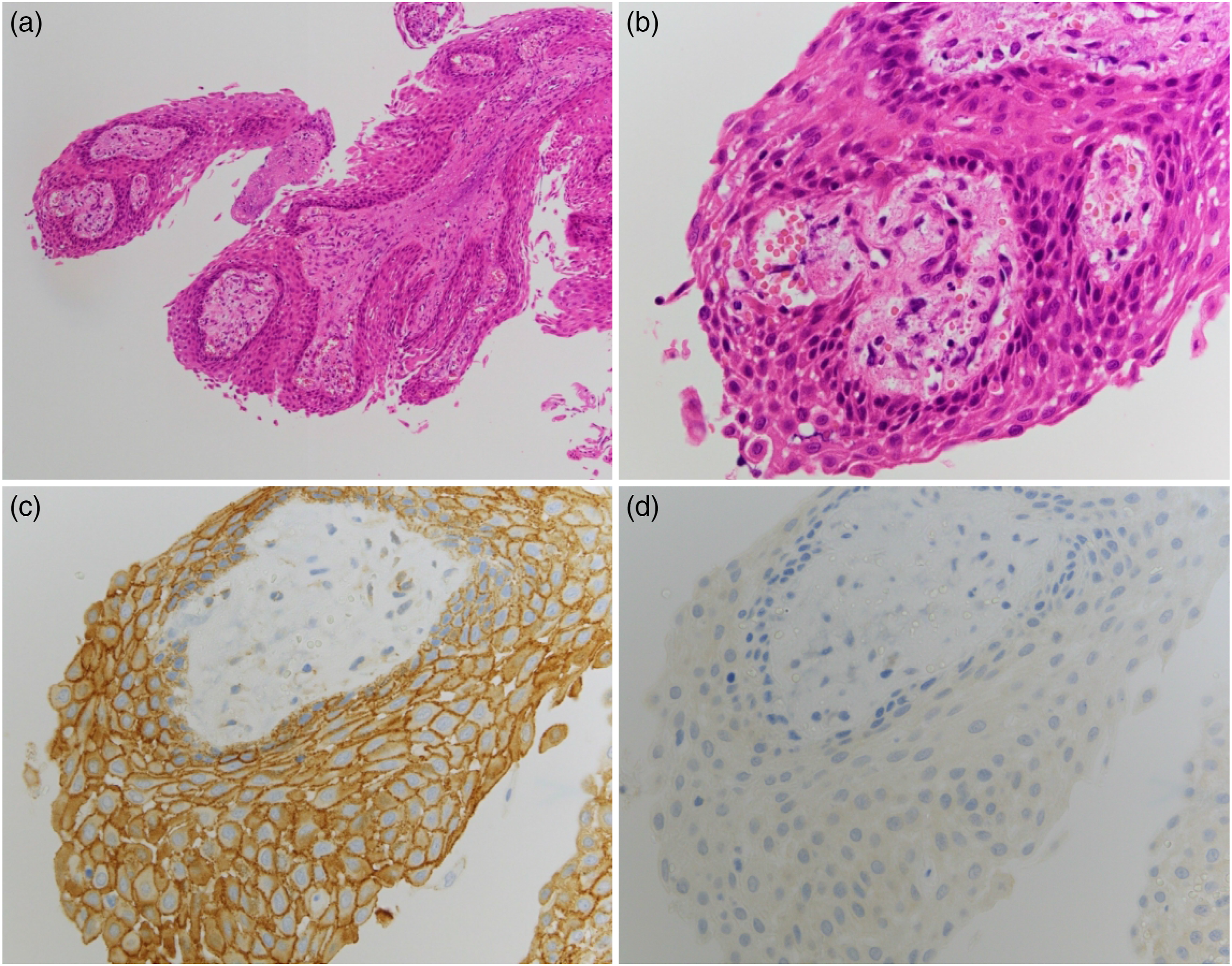
No apparent tumor recurrence or central nervous system infection was observed during follow-up MRI after 1 year. Hormone replacement therapy was administered due to hypopituitarism.
Discussion
Previous cases of pediatric papillary craniopharyngioma published in the literature.

BRAF: B-Raf proto-oncogene, serine/threonine kinase; Cal: calcification; CE: contrast enhancement; DWI: diffusion-weighted imaging; F: female; M: male; NA: not available; ref: reference; T1WI: T1-weighted imaging; T2WI: T2-weighted imaging; yr: year.
Previously published cases of an abscess inside a craniopharyngioma.

Cal: calcification; CE: contrast enhancement; DWI: diffusion-weighted imaging; F: female; M: male; NA: not available; ref: reference; T1WI: T1-weighted imaging; T2WI: T2-weighted imaging; yr: year.
Because papillary craniopharyngiomas are rare in children, we will discuss the imaging findings of craniopharyngiomas in adults. An analysis of 32 reported cases of papillary craniopharyngiomas3,19 revealed that 29 (91%), 2 (6%), and 1 (3%) tumors were located in the suprasellar region, intrasellar to suprasellar region, and third ventricle, respectively. Around 41%, 41%, and 18% of the tumors were solid, solid and cystic, and cystic, respectively. On non-contrast (NC) T1WI, the solid tumor parts showed iso- or slightly low signal intensity relative to that of the gray matter. On T2WI, the solid tumor parts showed an inhomogeneous, but high signal intensity. The signal intensity of the rare cystic tumor parts was mostly low on NC-T1WI and high on T2WI. A thin peripheral contrast-enhancing rim was visible on contrast-enhanced (CE) T1WI. Calcifications are the key imaging findings because no 3 or rare (<1%) 19 calcifications are seen in papillary craniopharyngiomas; conversely, the typical adamantinomatous craniopharyngiomas can be summarized by the “90% rule”: approximately 90% of the tumors are predominantly cystic, show more or less prominent calcifications, and show enhancement in the cyst walls. 13 In summary, a papillary craniopharyngioma is typically located in the suprasellar region and usually presents as a solid or predominantly solid enhancing mass without calcification in adult patients. In our patient’s case, there was no calcification in the tumor; however, the tumor components showed an irregular enhancing cystic mass. The reason for this finding was thought to be the effect of the intratumoral abscess.
Pituitary abscesses are classified as either primary (or de novo) and secondary (arising within preexisting pituitary lesions such as pituitary adenomas and craniopharyngiomas). 20 Secondary pituitary abscesses are hypothesized to be caused by tumors that disrupt the local blood circulation and impair the immune response, which in turn, disrupt the control of infection. 21 Furthermore, these tumors may have areas of necrosis, which can make them more susceptible to infection. 21 A retrospective analysis of the MRI features of 51 cases with pituitary abscesses by Wang et al. 22 revealed specific radiological features on MRI, including iso- or low signal intensity on T1WI (58.8%), iso- or high signal intensity on T2WI (76.5%), and the disappearance of the posterior pituitary bright spot in most cases; these findings are consistent with those of the present case. Furthermore, they observed rim or rim-like enhancement after contrast material injection in 82.4% of the patients; half of these showed typical rim enhancement, while the remaining half showed atypical rim enhancement with special signs, such as an enhancing, thick abscess wall and high intensity flocculent or cotton-like foci within the internal low signal intensity region. Other features described are evidence of pituitary stalk thickening and leptomeningeal enhancement. 23 Our patient showed a thick and irregular rim-like enhancement in the periphery of the lesion with ventricular wall enhancement on CE-T1WI. The pituitary stalk and pituitary gland could not be visualized.
DWI is widely used to differentiate cerebral abscesses from other necrotic masses. 24 Brain abscesses typically give a high intensity signal on DWI, with a decreased ADC value in the central region. However, the high signal intensity on DWI is not specific to pituitary abscesses, because pituitary apoplexy can also exhibit a high signal intensity on DWI, but with normal to high ADC values due to the T2 shine-through effect. 25 The accuracy of DWI in pituitary abscess identification remains controversial; however, clinical findings such as fever, a high inflammatory response, and meningitis, as well as short-term morphological changes on imaging, may help in accurate diagnosis.
In conclusion, we have reported a case of a teenager with a papillary craniopharyngioma coexisting with an intratumoral abscess. Papillary craniopharyngioma is located in the suprasellar region and is usually a solid or predominantly solid enhancing mass without calcification. Pituitary abscesses show high signal intensity on DWI, with a decreased ADC value in the central region, as well as rim-like enhancement. Clinical findings (fever, high inflammatory response, and meningitis) as well as short-term morphological changes on imaging could also be key to an accurate diagnosis.
Footnotes
Author contributions
Katsuhiro Takagi, Kazufumi Kikuchi, Akio Hiwatashi, Osamu Togao, and Kousei Ishigami drafted the manuscript and designed the figures. Yuhei Sangatsuda, Daisuke Kuga, and Masahiro Mizoguchi edited the surgical part. Hidetaka Yamamoto and Toru Iwaki edited the pathological part. All authors discussed the results and contributed to the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the JSPS KAKENHI (Grant Number 20K16791), Kaibara Morikazu Medical Science Promotion Foundation, and Kawano Masanori Memorial Public Interest Incorporated Foundation for Promotion of Pediatrics.