
Abstract
Background
Various studies have been made about the most effective and safest type of treatment for vertebral compression fractures (VCFs). Long-term results are needed for qualitative evaluation.
Purpose
The purpose of the study is to evaluate the effectiveness of percutaneous vertebroplasty (PVP) and percutaneous kyphoplasty (PKP) procedures for VCFs.
Materials and Methods
Forty-nine patients who received either PVP or PKP between 2002 and 2015 returned a specially developed questionnaire and were included in a cross-sectional outcome analysis. The questionnaire assessed pain development by use of a visual analog scale (VAS). Imaging data (CT scans) were retrospectively analyzed for identification of cement leakage.
Results
Patients’ VAS scores significantly decreased after treatment (7.0 ± 3.4 => 3.7 ± 3.4), (p < 0.001). The average pain reduction in patients treated with PVP was −3.3 ± 3.8 (p < 0.001) (median −3.5) and −4.0 ± 3.9 (p < 0.001) (median −4.5) in patients treated with PKP. Fifteen Patients (41.7%) receiving PVP and four patients (30.7%) receiving PKP experienced recurrence of pain. Cement leakage occurred in 10 patients (22.73%). Patients with cement leakage showed comparable VAS scores after treatment (6.8 ± 3.5 => 1.4 ± 1.6), (p = 0.008). Thirty-nine patients reported an increase in mobility (79.6%) and 41 patients an improvement in quality of life (83.7%).
Conclusion
Pain reduction by means of PVP or PKP in patients with VCFs was discernible over the period of observation. Percutaneous vertebroplasty and PKP contribute to the desired treatment results. However, the level of low pain may not remain constant.
Introduction
More than 200 million people worldwide suffer from osteoporosis. This disease is destined to become an increasingly common problem for society and public health as the incidence increases continuously due to the ever rising life expectancy and growing world population.1,2 The spine is particularly affected with the occurrence of vertebral compression fractures (VCFs), 3 mainly caused by bone mineral loss in patients with osteoporosis or infiltrative tumors.4,5 Patients with osteoporotic VCFs often suffer from chronic pain, clinical depression, and decreased quality of life.6,7 Vertebral compression fractures can be treated in a minimally invasive fashion by percutaneous vertebroplasty (PVP) and percutaneous kyphoplasty (PKP).8–10 They are used for immediate stabilization of the affected vertebral body by means of image-guided cement injection.11,12
For treatment of traumatic fractures of the spine, controversial statements have been made about the most effective and safest type of treatment.12,13 In particular, several publications addressed the potential complications of cement leakages associated with PVP and PKP.14,15 For clinical decision-making, well-designed trials are needed. 16 Additionally, an important criterion in the successful treatment of VCFs is the long-term prognosis. Therefore, the aim of our investigation was to analyze the success rate of PVP and PKP, to determine the rate of cement leakage and its associated consequences. We performed the study to evaluate pain reduction.
Material and methods
Patients
This investigation was carried out in a cross-sectional outcome analysis and retrospective manner. It was approved by the clinical ethics committee of the medical department, with special consideration of the Federal Data Protection Act (BDSG). The study was conducted in accordance to the current version of the Helsinki Declaration and in compliance with the ICH-GCP guidelines. All patients gave written informed consent before being included in this study. For the cross-sectional data collection, a special questionnaire was developed including patient information and the declaration of consent. In March 2015, the questionnaire was sent to all patients who were treated in our university hospital from January 2002 to February 2015 receiving either PVP or PKP. Patients with more than one procedure were excluded. Also excluded were patients who participated in a previous study.
Patients were informed that their disease-related data would be stored in a pseudonymized form, and all final data would be anonymized for scientific publications.
Inclusion criteria
A period of 24 months was set for data acquisition. At the end (March 2016), a total of 49 envelopes were returned containing the completed questionnaires and the signed declarations of consent.
Retrospective analysis
The following parameters were retrospectively collected from existing patient charts: date of surgical intervention, age of patient, sex of patient, type of intervention (PVP and PKP), number of vertebral bodies with fracture, quality, and type of augmentation associated with complications. Using periprocedural computed tomography (CT) imaging data, a retrospective evaluation of procedure was performed to determine the occurrence of cement leakage. CT scans were performed before and immediately after the intervention. The leaks were assessed by two radiologists with 25 years of experience in musculoskeletal imaging. They were subdivided according to the general classification of vertebral body cement leakage into the following three types: Type-B leakage: cement into the basovertebral vein. Type-S leakage: cement into segmental veins. Type-C leakage: cortical defect.
17
Percutaneous vertebroplasty
Percutaneous Vertebroplasty is an interventional radiological procedure in which polymethyl methacrylate (PMMA) is injected into the fractured vertebral body. It involves venous embolization of the vertebral body under imaging guidance. A bone biopsy needle is inserted into the center of the affected vertebral body via bone fenestration. Polymethyl methacrylate is injected very slowly under continuous imaging. CT scan is performed to evaluate final distribution of cement identifying possible leakages.
Percutaneous kyphoplasty
Percutaneous kyphoplasty is an interventional technique in which loss of height of a collapsed vertebral body is corrected by inflation of a balloon tampon prior to cement deposition.
Percutaneous kyphoplasty is a variant of the PVP approach that is not only designed to ensure fracture fixation but also for reconstruction of the vertebral anatomy and correction of kyphotic spinal deformity.
Questionnaire
The questionnaire was related to pain development and the resulting functional limitation of the spine. The questionnaire used the visual analog scale (VAS) to record patients' subjective complaints, divided into levels zero (no pain) to ten (maximum pain). The questionnaire was subdivided into part A (general questions), part B (pre-therapy questions), and part C (post-therapy questions). Part A gathered general patient data, including size, weight, age, and sex. Part B addressed the patient’s situation prior to treatment (PVP or PKP), while subjective pain perception was determined according to the VAS score. Part C was set up to assess subjective success after treatment, focusing on pain development (VAS score) and individual improvement in mobility.
Statistical analysis
Statistical evaluation was performed by non-parametric tests (Wilcoxon matched-pairs test and Wilcoxon–Mann–Whitney U test) and by 4-field test. Statistical evaluation was performed using a dedicated statistical software (MedCalc, Ostende, Belgium).
Results
Among the 49 patients included, there were 33 (67.3%) women and 16 (32.7%) men. Mean age was 74 ± 11.7 (median 75) years (range 38–90 years). Mean high was 165.7 ± 9.3 (median 165) cm and mean weight was 70.4 ± 13.8 (median 70) kg.
Assessment of pain intensity
Out of the 49 patients, 36 (73.5%) had undergone PVP and 13 (26.5%) PKP. The overall mean pre-therapeutic VAS score was 7.0 ± 3.4 (median 8.0). The mean post-therapeutic VAS score was 3.7 ± 3.4 (median 3.0) (Fig. 1) indicating a decrease of the VAS score by 47%. The change in pain, calculated by the difference between the VAS (before therapy) and the VAS (after therapy), was around −3.5 ± 3.8 (VAS-diff). The median was −4.0. (boxplot) VAS before/after therapy. Representation of VAS (0–10) before and after therapy. Boxes show the upper and lower quartiles. The median is represented by a vertical bar in the center of each box. Minimal and maximal values are represented by the whiskers. VAS: visual analog scale.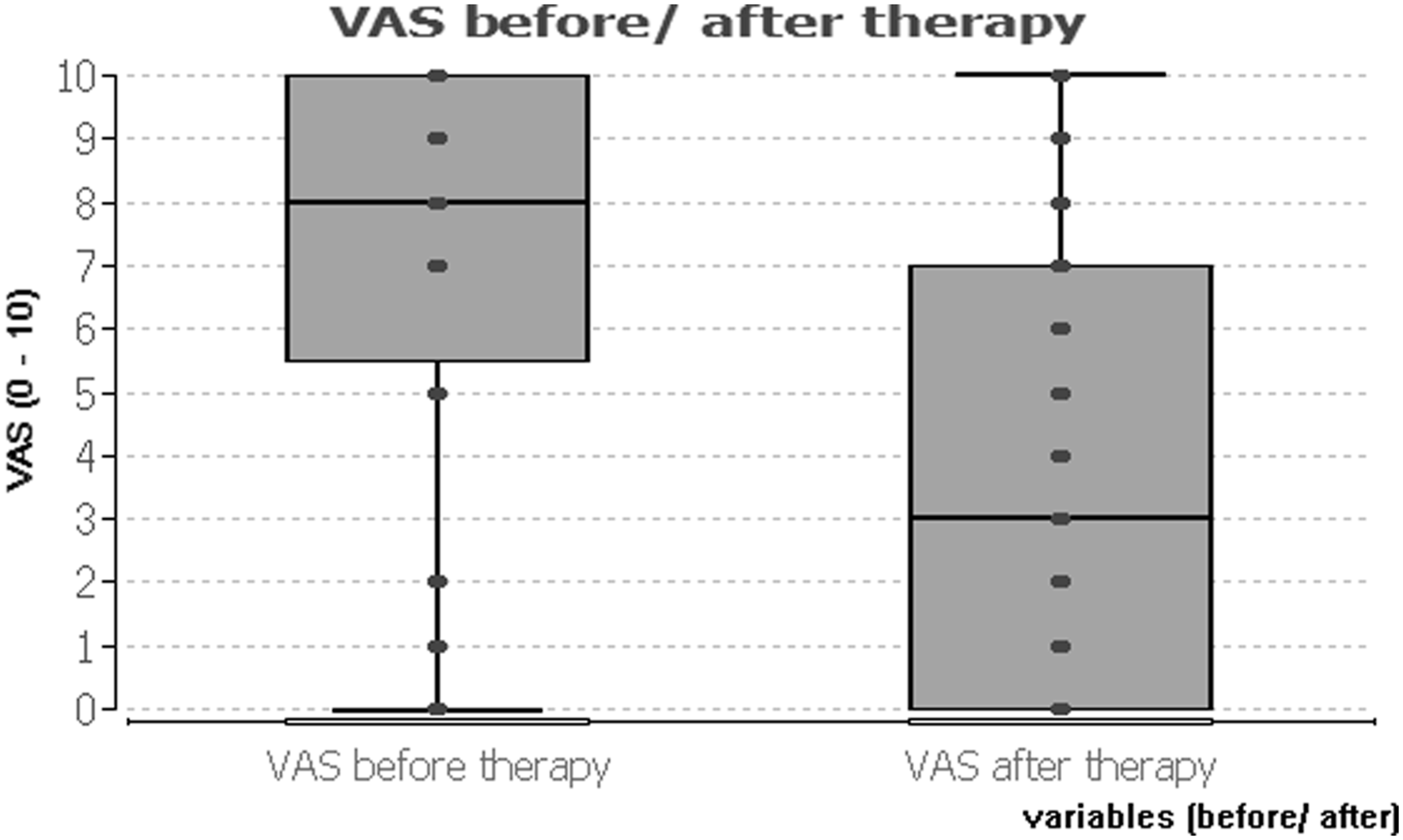
On patient level, the fraction of patients with decreased VAS scores were 35 (71.4%), with stable scores eleven (22.4%) and with increased scores three (6.1%).
The reduction in pain was statistically significant (p < 0.001) by using the Wilcoxon matched-pairs test.
The average pain reduction in patients treated with PVP was −3.3 ± 3.8 (median −3.5) and −4.0 ± 3.9 (median −4.5) in patients treated with PKP. The decrease in VAS score was significant for both therapies (p < 0.001). The fraction of patients treated with PVP with decreased VAS scores were 23 (63.9%), with stable scores 10 (27.8%) and with increased scores 2 (5.6%). The fraction of patients treated with PKP with decreased VAS scores were eleven (84.6%), with stable scores one (7.7%) and with increased scores one (7.7%). There was no significant difference in reduction of pain between the two therapies (p = 0.328) by using the Mann–Whitney U test (Fig. 2). (boxplot) VAS before/after therapy (grouped into PVP/PKP). Representation of VAS (0–10) divided into the periods before and after therapy, grouped by type of procedure (PVP/PKP). PVP: percutaneous vertebroplasty; PKP: percutaneous kyphoplasty; VAS: visual analog scale.
Over the treatment period from January 2002 to February 2015, there was no significant difference in the distribution of VAS-diff. It was on average −3.5 ± 3.8 (median −4.0) over the observation period.
Cement leaks
Review of imaging data revealed ten patients with cement leaks out of the total 49 patients, resulting in a 20.4% incidence. Three patients (6.67%) suffered a cortical defect (type C leakage). Four patients (8.16%) showed leakage of cement into segmental veins (type S Leakage). One patient (2.04%) suffered from leakage of cement into the basovertebral vein (type B leakage). Two patients suffered from both, type B and type S (4.08%). The percent distribution of leakages was 30% for type C, 60% for type S, and 30% for type B (Fig. 3). With regards to the utilized procedure type, six patients (16.67%) who had received PVP and four patients (30.77%) who had received PKP suffered from cement leakage. There was no significant difference in the rate of occurrence of cement leakage between the procedure types (p = 0.667). Furthermore, there was no significant difference in the occurrence of cement leakage and the age of the patients (p = 0.531). (bar chart) Distribution of leakages. Representation of the relative frequency of different types of cement leaks.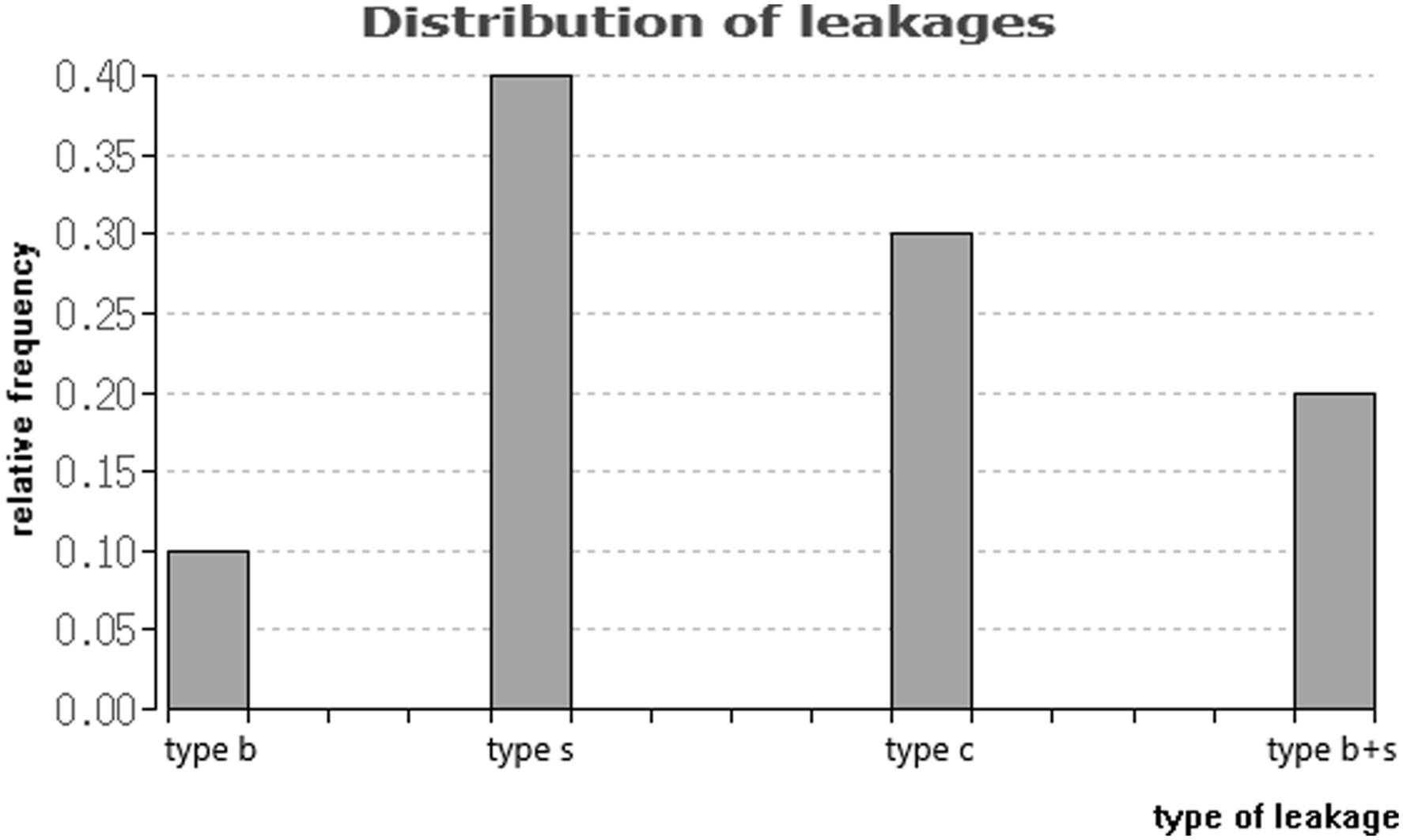
In the 10 patients with cement leaks, the mean pre-therapeutic VAS score was 6.8 ± 3.5 (median 7.5). The mean post-therapeutic VAS score was 1.4 ± 1.6 (median 1.0) (Fig. 4). The reduction in pain was statistically significant (p = 0.008). (boxplot) VAS before/after therapy (grouped into occurrence of leakage). Representation of VAS (0–10) divided into the periods before and after therapy, grouped by occurrence of cement leakage. VAS: visual analog scale.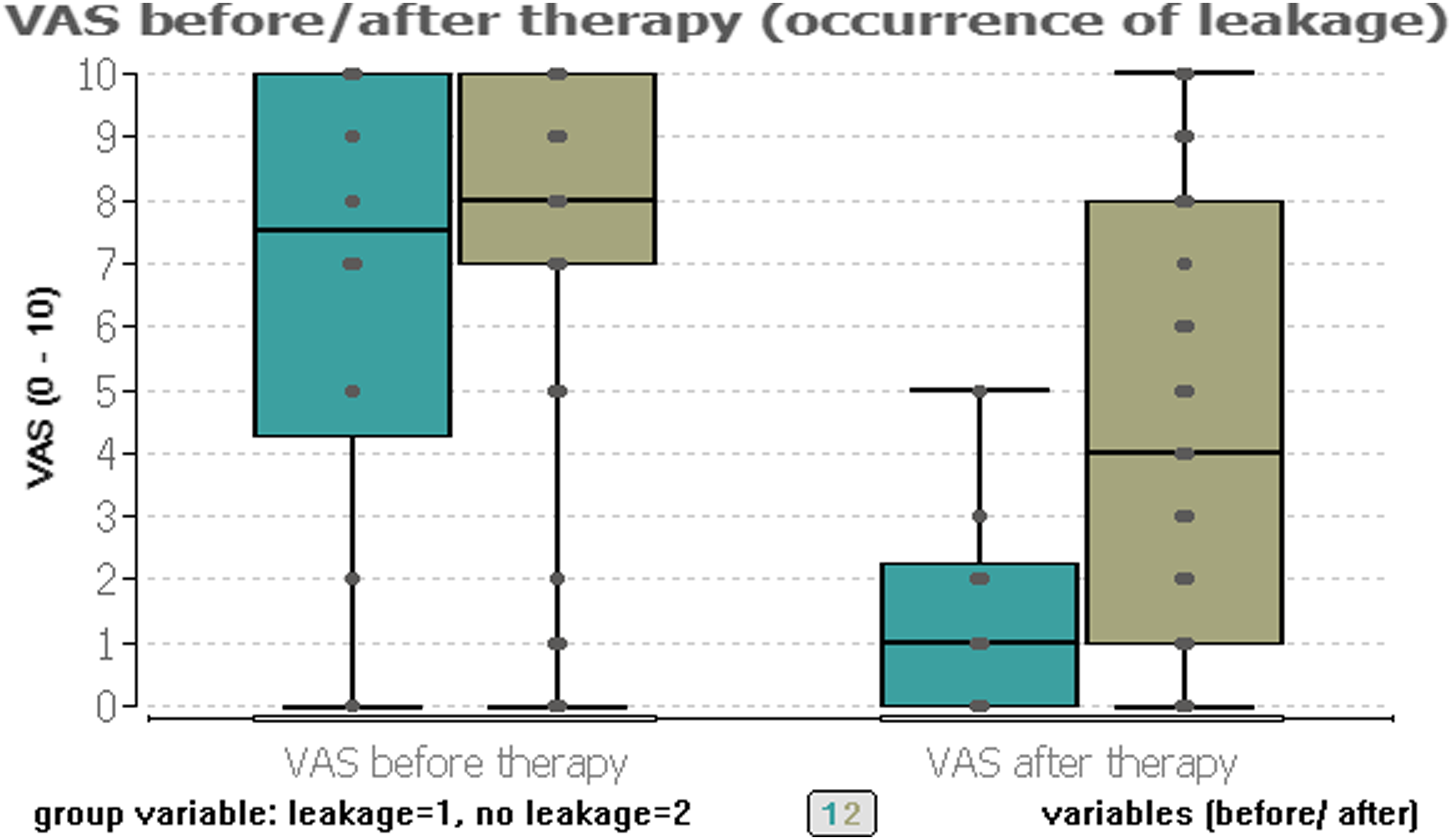
Recurrence of pain
Of the 49 patients, 19 (38.8%) reported they experienced a recurrence of pain on the treated vertebral body at least three months after the intervention. Fifteen of these patients (41.7%) had received PVP and four patients (30.7%) had received PKP. Of the 10 patients who showed cement leakage, one patient (10%) reported a postprocedural increase in pain.
Mobility and quality of life
Thirty-nine out of the 49 enrolled patients (79.6%) reported a postprocedural increase in mobility, which was also analyzed by comparing the pre- and post-therapeutic VAS values. The increased mobility was statistically significant (p < 0.001). Nine patients (90%) with cement leakage reported an increase in mobility. Out of the 49 patients, 41 (83.7%) reported an improvement in quality of life. After intervention all 39 patients who had an increase in mobility also experienced an improvement in quality of life.
Time span
Data were collected from patients who underwent procedures at our institution between January 2002 and February 2015, resulting in a period of 157 months (approximately 13 years). The mean time interval between the treatments and the clinical assessment was in between the years 2009 (median 2008) to 2015 (data acquisition). For patients treated with PVP, it was from 2007 (median 2007) to 2015 and treated with PKP, it was from 2013 (median 2013) to 2015.
Out of 49 patients, 19 patients (38.8%) were treated in 2015–2010, 26 patients (53.1%) in 2009–2005, and four patients (8.2%) in 2004–2002. When retrospectively comparing the reduction of symptoms at different time points, no significant variation in the level of pain reduction was found (p = 0.694) (Fig. 5). (single courses) VAS course. Representation of grouped single courses from VAS (before) to VAS (after) therapy, grouped by type of procedure (PVP/PKP), red line: median. PVP: percutaneous vertebroplasty; PKP: percutaneous kyphoplasty; VAS: visual analog scale.
Analyzing patients’ data over the time period revealed no significant difference in the recurrence of discomfort on the respective vertebral body (p = 0.438). The occurrence of cement leakage also led to no significant difference when considering the different time points of the corresponding procedure (p = 0.415).
Discussion
The aim of this study was to evaluate the effectiveness of the procedures PVP/PKP. We evaluated the examination of the treatment effects on osteoporotic VCFs. By analyzing the collected assess patient outcomes, we demonstrated PVP and PKP relieve pain in patients with VCFs significantly. Most patients in the investigated population reported a noticeable pain reduction with average VAS scores dropping from 7.0 to 3.7. Of the cohort, 71.4% reported noticeably pain reduction by lowered VAS scores. 22.4% had stable scores with no change in symptoms. Only 6.1% of patients showed increased VAS scores.
Our study covered data from the interventional treatment of patients over a time span from 2002 to 2015 with a mean time interval of 7 years in between treatment and clinical assessment. As our investigation covered interventions that were performed within a long frame of time in an elderly population, only a proportion of patients could successfully be contacted and were able to return the designated questionnaire. A large proportion of the patients died before the beginning of our study due to such factors as the advanced age.
The complication that occurred during or after a PVP/PKP was cement leakage. In our study, a total of 10 patients (22.73%) had at least one cement leakage. Cement leakage was reported in six patients (16.67%) who received PVP and in four patients (30.77%) who received PKP. In the review study by Zhao et al. (2016), PKP proved to show lower risk of cement leakage than PVP; however, this result also could not be substantiated by statistical analysis. 18 The rate of detected cement leakage during PVP and PKP may be increased if identification is made by a CT scan which is a more accurate process than fluoroscopy or postoperative radiography.19,20
We demonstrated patients with leakage also had a decrease in pain. Visual analog scale dropped from 6.8 to 1.4. This effect was noticeable over the whole period of observation with no increase in VAS.
A limitation is the lack of a comparison with non-interventional fracture treatment (sole conservative therapy) or a placebo group that could have been used to study comparative efficacy in the same system.
Several previous studies have shown the benefits by lowered VAS scores in patients treated with PVP/PKP. Similar to our findings, Klezl et al. (2011) also found that patients had a nearly 50% reduction in pain scores immediately after the intervention. 21 According to the systematic review study by Hulme et al. (2006), 92% of patients receiving PKP and 87% of patients receiving PVP experienced significant pain relief. 22 These effects were documented shortly after the end of intervention.
Our survey has shown the positive development in pain after data collection. After one year, the results were documented and evaluated. There were different time intervals between the treatments (2002–2015) and the clinical assessment, which may have resulted in inaccurate results. Additionally, due to the high average age of the patients, other interventions had overlapped with the therapeutic approach documented in this study. There could have been potential bias through concomitant diseases.
The review by Taylor et al. (2006) showed both methods were effective therapies for the treatment of patients with symptomatic VCFs, although PKP appeared to offer the better profile in pain reduction. 23 In accordance, our study indicates 63.9% in patients treated with PVP and 84.6% in patients treated with PKP experienced pain relief. Thus, PKP appeared to be slightly better than PVP in the effectiveness of pain reduction. Recurrence of pain was higher with PVP (41.7%) than with PKP (30.7%). Because of different mean time intervals between the treatments and the clinical assessment (PVP 7 years and PKP 3 years), there could have been a bias by analyzing pain development. However, there was no statistically significant difference.
Our study showed that both PVP and PKP contribute to an increased mobility. In total, 39 of all participating patients (79.6%) reported an overall increase in mechanical spinal body function. This is in accordance with the studies by Luo et al. (2009) and Wardlaw et al. (2009) in which PVP and PKP proved to be equally effective in restoring mechanical function.24,25 The study by Landham et al. (2015) also showed that PKP was better able to restore vertebral height and reverse wedge deformity. 26 Similar results were shown by the study of Wang et al. (2018). Restoring the vertebral height and local kyphotic angle corrections of PKP were comparatively better than those of PVP. 27 In our study the kyphotic angle and pre- and post-anterior vertebral height were not measured. We focused on the development of VAS for pain assessment as a marker of treatment response.
In our study, there was a significant correlation between the increase in quality of life and the increased mobility. It was also confirmed that the decrease in VAS was significantly correlated with an increase in the quality of life.
In conclusion, our study represents an evaluation of the results of PVP and PKP. Both methods contribute to the desired treatment results, partially even after a period of more than 10 years. The effectiveness of PVP and PKP was shown by lowered VAS scores. However, the level of low pain did not remain constant for all patients. As these findings represent a small clinical evaluation, additional studies are required to further explore long-term outcomes to give an assessment of the prognosis for PVP and PKP.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.