
Abstract
Background
A triple-coaxial (triaxial) system, which consists of a small microcatheter, a large microcatheter, and a 4-Fr. catheter, has been reported to allow super-selective catheterization. A 1.6-Fr. microcatheter has recently become available as the small microcatheter for the triaxial system, in addition to 0.014-in. pushable bare platinum coils that may be introduced into the 1.6-Fr. microcatheter.
Purpose
The purpose of the present study was to evaluate the feasibility of 0.014-in. pushable bare platinum coils in embolization through the 1.6-Fr. microcatheter of the triaxial system.
Material and Methods
Between November 2015 and October 2019, 19 embolizations were performed on 18 patients, 9 males and 9 females with a median age of 77 years (range, 41–88 years), using 0.014-in. pushable bare platinum coils through the 1.6-Fr. microcatheter of the triaxial system. The technical success rate, clinical success rate, and complications associated with the procedure were assessed. Technical success was defined as the successful delivery and placement of 0.014-in. pushable bare platinum coils, and clinical success as the immediate postembolic complete cessation of blood flow confirmed by digital subtraction angiography.
Results
Eighty-four 0.014-in. pushable bare platinum coils were delivered and 19 arteries were successfully embolized. The median number of 0.014-in. pushable bare platinum coils was 4 (range, 1–12). The technical success rate was 100% (84/84) and the clinical success rate was also 100% (19/19). There were no complications associated with the procedures.
Conclusion
The use of 0.014-in. pushable bare platinum coils in super-selective embolization through the 1.6-Fr. microcatheter of the triaxial system appears to be feasible and safe.
Keywords
Introduction
Super-selective catheterization is necessary in various transarterial procedures, such as embolization for gastrointestinal bleeding, hemoptysis, and type II endoleaks following endovascular aneurysm repair (EVAR), and transcatheter arterial chemoembolization (TACE) for hepatocellular carcinoma (HCC),1–4 but may be challenging to perform due to the tortuosity of vessels. A triple-coaxial (triaxial) system, which consists of a small microcatheter, a large microcatheter, and a 4-Fr. catheter, is useful for super-selective catheterization because it has been shown to prevent the kick-back of small microcatheters by providing good support from the large microcatheter. 5 A 1.6-Fr. microcatheter has recently become available as a small microcatheter for the triaxial system and may facilitate super-selective catheterization. However, since the inner diameter of the 1.6-Fr. microcatheter for embolization is so small, there have been no pushable coils that are introducible into the 1.6-Fr. microcatheter. Therefore, only electrically detachable coils were available in this triaxial system, which were not cost effective. However, 0.014-in. pushable bare platinum coils that can be introduced into the 1.6-Fr. microcatheter have recently become available in Japan. The purpose of the present study was to evaluate the feasibility of 0.014-in. pushable bare platinum coils in super-selective embolization through the 1.6-Fr. microcatheter of the triaxial system.
Material and Methods
This retrospective study was approved by the Institutional Review Board. Written informed consent for the procedure was obtained from all patients. Between November 2015 and October 2019, 19 embolizations were performed on 18 patients, 9 males and 9 females with a median age of 77 years (range, 41–88 years), using 0.014-in. pushable bare platinum coils through the 1.6-Fr. microcatheter of the triaxial system. In all cases, the triaxial system was introduced initially, because the target arteries appeared to be small and/or tortuous based on preprocedural CT images. Etiologies were as follows: pseudoaneurysm of the visceral artery in seven, gastrointestinal bleeding in six, type II endoleak after EVAR in three, altered blood flow in TACE in two, and retroperitoneal arteriovenous fistula in one. Medical records and images were reviewed, and the technical success rate, clinical success rate, and complications associated with the procedure were evaluated. Technical success was defined as the successful delivery and placement of 0.014-in. pushable bare platinum coils, and clinical success as the immediate postembolic complete cessation of blood flow confirmed by digital subtraction angiography. All images were interpreted by two radiologists with more than 10 years of experience in diagnostic and interventional radiology. Any discrepancies were resolved by consensus. Complications requiring prolonged hospitalization, permanent adverse sequelae, and death were classified as major complications, and the remaining complications were considered to be minor.
Technique of super-selective embolization using 0.014-in. pushable bare platinum coils through the 1.6-Fr. microcatheter of the triaxial system
All 19 procedures were performed via the femoral artery with a sheath and a 4-Fr. catheter. A large microcatheter (2.7-Fr. Sniper 2 high-flow in 15, Terumo, Tokyo, Japan, 2.85-Fr. Carry Leon High-flow in 3, UTM, Toyohashi, Japan; 2.9-Fr. Leonis Mova in 1, Sumitomo, Tokyo, Japan) and a small microcatheter (1.6-Fr. MARVEL-S, Tokai Medical, Kasugai, Japan) were then introduced. The 1.6-Fr. microcatheter was advanced along the 0.014-in. micro guidewire (BEGIN; ASAHI INTEC, Nagoya, Japan), and the large microcatheter was then advanced along the 1.6-Fr. microcatheter. Therefore, with good support from the large microcatheter, the 1.6-Fr. microcatheter was advanced deeply. After placement of the 1.6-Fr. microcatheter at the aimed position, coil embolization was initiated. Electrically detachable coils were initially placed in 15 out of the 19 procedures, followed by the introduction of 0.014-in. pushable bare platinum coils (C-Stopper 14; Piolax, Kanagawa, Japan). Only 0.014-in. pushable bare platinum coils were used in the remaining four procedures. In all procedures, 0.014-in. pushable coils were introduced using a 0.014-in. coil-pusher (C-STOPPER COIL PUSHER, Piolax). The use of other embolic materials, such as gelatin sponges or N-butyl-2-cyanoacrylate (NBCA), was decided by the operator.
Results
Details on embolization and the results obtained are shown in Table 1. Eighty-four 0.014-in. pushable bare platinum coils were used for embolization. The median number of 0.014-in. pushable bare platinum coils was 4 (range, 1–12). All 0.014-in. pushable bare platinum coils were successfully delivered and placed at the aimed position without any technical issues, such as coil migration, unraveling, and jams in the microcatheter. Therefore, the technical success rate was 100% (84/84) (Figs 1 and 2). The 19 arteries subjected to embolization were as follows: a branch of the renal artery in 3, a branch of the posterior superior pancreaticoduodenal artery, a branch of the left colic artery, the inferior mesenteric artery, and right gastroepiploic artery in 2 each, and the left gastric artery, a branch of the splenic artery, the hepatic falciform artery, a branch of the ileocolic artery, a branch of the right colic artery, left deep iliac circumflex artery, right 4th lumber artery, and left hepatic artery in 1 each. In four cases, other embolic materials were added: NBCA in three and gelatin sponges in one. In all procedures, the immediate postembolic complete cessation of blood flow was confirmed, and, thus, the clinical success rate was also 100% (19/19). Furthermore, no complications, such as ischemia of the organ, were observed following embolization in any case.
Details of embolization using 0.014-in. pushable bare platinum coils.

AVF: arteriovenous fistula; EVAR: endovascular aortic repair; GS: gelatin sponge; ICA: ileocolic artery; IMA: inferior mesenteric artery; LCA: left colic artery; LGA: left gastric artery; NBCA: N-butyl-2-cyanoacrylate; PSPDA: posterior superior pancreaticoduodenal artery; RA: renal artery; RCA: right colic artery; SPA: splenic artery; TACE: transcatheter arterial chemoembolization.
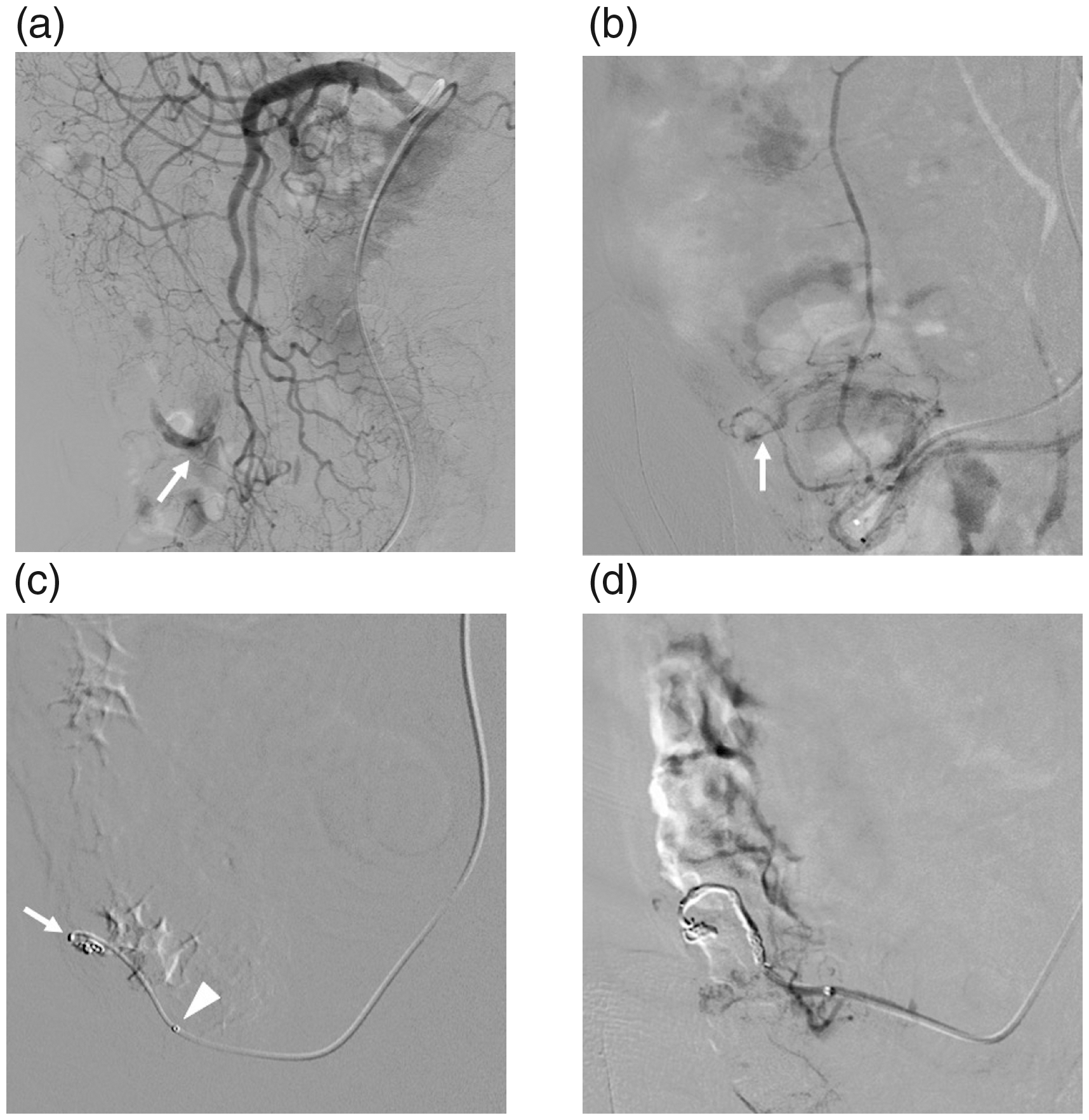
An 88-year-old man presented with bleeding from the ileal colon artery (ICA) due to diverticulum. (a) Angiography of the superior mesenteric artery shows extravasation (arrow) from the branch of the ICA. (b) Angiography from the 2.7-Fr. microcatheter advanced into the ICA shows extravasation (arrow). (c) The 1.6-Fr. microcatheter (arrow) was advanced deeply through the 2.7-Fr. microcatheter (arrow head) and embolization was initiated using 0.014-in. pushable bare platinum coils. (d) Five 0.014-in. pushable bare platinum coils were used and embolization was successfully accomplished.

A 69-year-old woman presented with hepatocellular carcinoma (HCC) in the left medial segment and underwent transcatheter arterial chemoembolization (TACE). (a) Angiography of the left hepatic artery shows the hepatic falciform artery. We attempted to embolize the hepatic falciform artery in order to alter blood flow before TACE. (b) The 1.6-Fr. microcatheter (arrow) was advanced to the hepatic falciform artery through the 2.7-Fr. microcatheter (arrow head). (c) Embolization was performed using one 0.014-in. pushable bare platinum coil. Angiography shows HCC (arrows). (d) TACE for HCC in the left medial segment was successfully performed.
Discussion
In the present study, we achieved high technical and clinical success rates in super-selective embolization with 0.014-in. pushable bare platinum coils through the 1.6-Fr. microcatheter of the triaxial system without any coil complications. Due to advances in the development of microcatheters, we now use thin microcatheters, such as 1.7-Fr. or smaller.6–9 The triaxial system was previously shown to be useful for super-selective catheterization under various conditions. 5 In particular, it should be very effective for cases which definitely need super-selective catheterization, such as those with pseudoaneurysm, gastrointestinal bleeding, or type 2 endoleak after EVAR. Furthermore, 1.6-Fr. microcatheters have recently become available in the triaxial system and facilitate super-selective catheterization. The usefulness of 0.010-in. electrically detachable coils with 1.7-Fr. microcatheters in embolization of the visceral artery has been demonstrated. 6 The inner space of 1.7-Fr. microcatheters is small, which necessitates the use of 0.010-in. electrically detachable coils. However, the limitation of embolization with electrically detachable coils is its high cost, at approximately US$1200 per coil. Pushable coils cost approximately only US$100 per coil. Therefore, 0.014-in. pushable bare platinum coils enable super-selective and inexpensive coil embolization. The use of small pushable fibered coils (Tornado Embolization Microcoils; Cook, Bloomington, IN, USA) has been reported in 2.0- or 1.8-Fr. microcatheters. 10 In our experience, however, the pushable fibered coils cannot be inserted into the 1.6-Fr. microcatheter, although their diameter is the same as the diameter of C-Stopper 14 (0.014 in.). We think this should be due to the nature of the fiber. While the embolic power of fibered coils is stronger than that of bare platinum coils, we achieved a high clinical success rate with 0.014-in. pushable bare platinum coils and consider them to be useful, even without fibers.
In the present study, there were seven cases of pseudoaneurysms of the visceral artery and six of gastrointestinal bleeding. The use of 1.7-Fr. microcatheters with 0.010-in. electrically detachable coils has been reported in embolization for gastrointestinal bleeding, 7 , 8 for which the triaxial system was also shown to be useful. 11 Alterations in blood flow in TACE for HCC were performed in two cases in the present study. It is an important procedure because the embolization of non-hepatic branches originating from hepatic arteries or arterioportal shunts in tumor-bearing areas may reduce the adverse effects of TACE. 10 We also consider the triaxial system to be useful for super-selective TACE; however, since there were previously no pushable coils available for the triaxial system, we had to use expensive electrically detachable coils. Therefore, 0.014-in. pushable bare platinum coils resolved this issue, and coil embolization may now be performed during TACE using the triaxial system at a reasonable cost.
The present study has several limitations. First, it had a single-center retrospective design and the sample size was not large. Second, the etiologies of cases and embolized arteries varied, and, thus, the conditions of each embolization differed. Third, there was no single operator for embolization, and the procedure was not completely standardized. Fourth, in 79% (15/19) of the present cases, embolization was performed with not only 0.014-in. pushable bare platinum coils, but also with other embolic materials: electrically detachable coils, NBCA, and gelatin sponges. Fifth, use of 0.014-in. pushable bare platinum coils through the 1.6-Fr. microcatheters was out of instructions for use, and thus this procedure should be performed with the personal responsibility of each operator.
In conclusion, the use of 0.014-in. pushable bare platinum coils in super-selective embolization through the 1.6-Fr. microcatheter of the triaxial system appears to be feasible and safe.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.