
Abstract
Background
Despite increases in the incidence of coagulopathy-related soft-tissue hematoma (CRSH), the relationship between computed tomography (CT) features and clinical severity remains unclear.
Purpose
To retrospectively evaluate the correlation between CT findings and clinical outcomes in CRSH.
Material and Methods
We retrospectively reviewed data of patients diagnosed with CRSH between March 2011 and March 2018. CRSH was morphologically classified according to the presence or absence of the fluid level pattern and was also divided into groups with or without extravasation as per CT findings. These CT findings were compared with the patients’ vital signs and laboratory investigation results.
Results
A total of 47 patients with CRSH were examined. Fluid level and non-fluid level patterns were observed in 28 (60%) and 19 (40%) patients, respectively. Anticoagulant therapy and extravasation were significantly correlated with the fluid level pattern. However, other clinicolaboratory outcomes, including shock index, hemoglobin, hematocrit, platelet count, and coagulation factors, showed no significant difference between the two patterns. In the comparison of hematomas with and without extravasation, none of the clinicolaboratory outcomes except for anticoagulant therapy showed significant differences.
Conclusion
CRSH with a fluid level pattern is significantly associated with extravasation. However, extravasation, which is generally suggestive of active bleeding, does not seem to be related to clinical severity in CRSH.
Introduction
Spontaneous hematoma is defined as the presence of hemorrhage from a non-traumatic and non-iatrogenic cause. Among the various etiologies, hemorrhage due to anticoagulation or bleeding diatheses typically presents as soft-tissue hematoma (1,2). With the aging population and the increased use of anticoagulation treatments, the incidence of coagulopathy-related soft-tissue hematoma (CRSH) has been increasing annually (3).
The clinical symptoms of spontaneous soft-tissue hematoma are usually non-specific, and the diagnosis is made on the basis of radiological findings, particularly those of computed tomography (CT). Typically, the location of CRSH as observed on CT images is at sites such as the rectus abdominal muscle and iliopsoas muscle, and the “hematocrit effect” (linear separation of cellular and liquid components of blood) is a specific sign of the lesion (1,2). However, there is no standard guidelines for the management of CRSH. Most cases are self-limiting and can be managed by conservative therapy alone (4–7). Nevertheless, when contrast-enhanced CT displays extravasation in the hematoma, physicians might be concerned about how to treat this hematoma that seems to reflect active bleeding.
Although several studies have recently reported the efficacy of transarterial embolization (TAE) for CRSH (3,8–17), the correlation between CT findings and clinical outcomes remain unclear. The aim of the present study was to characterize patients with CRSH by comparison of the morphological features on CT and clinical severity, to aid physicians in therapeutic decisions.
Material and Methods
Patient selection
Our institutional review board approved this single-institution, retrospective study. The institutional radiology database was screened for consecutive patients with CT-detected CRSH identified in our institution between March 2011 and March 2018. Exclusion criteria were as follows: (i) intraperitoneal or intrapleural hematoma; (ii) intraparenchymal visceral bleeding; and (iii) hematoma related to a traumatic or iatrogenic injury. In the remaining patients with spontaneous hematomas, the etiology of the hematoma was grouped as follows: (i) neoplasms (e.g. renal angiomyolipoma, renal cell carcinoma); (ii) vascular causes (e.g. renal aneurysm, abdominal aortic aneurysms); and (iii) CRSH (due to anticoagulation and bleeding diathesis). Finally, patients with CRSH were selected for this study.
Analytical items and definitions
CT findings of the hematoma
The location of the hematoma was confirmed by multidetector-row CT. First, hematomas were divided into two patterns based on morphological features: those with a fluid level pattern and those with a non-fluid level pattern (Figs. 1 and 2). A fluid level pattern was defined by the presence of single or multiple linear separations caused by the setting of cellular elements in the dependent portion, with the liquid portion in the upper layer of the lesion. A non-fluid level pattern was defined by the absence of linear separations. Morphological changes in hematoma patterns were also evaluated during follow-up CT examinations. Second, hematomas were also classified as being with or without extravasation. Intravenous administration of contrast medium was decided at the discretion of the attending physician depending on the patient’s condition, and the presence of extravasation was assessed on contrast-enhanced (CE) CT.
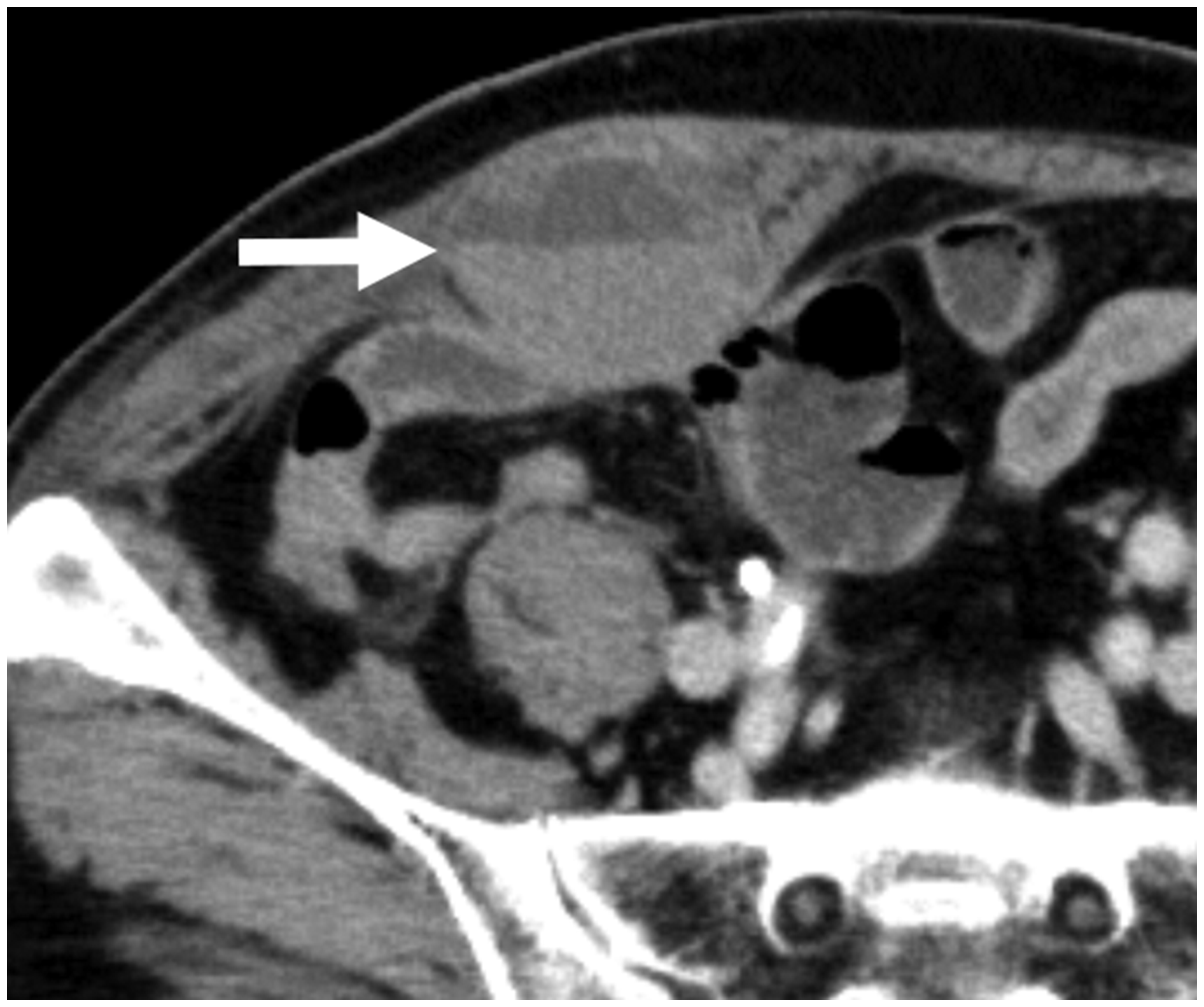
Fluid level pattern. Axial unenhanced computed tomography shows rectus abdominis muscle hematoma with cellular-fluid level (“hematocrit” sign, arrow).

Non-fluid level pattern. Axial unenhanced computed tomography shows rectus abdominis muscle hematoma, without cellular-fluid levels (arrow).
Clinical and laboratory outcomes
The causes of coagulopathy-related hematoma were identified based on electronic hospital records. The following outcomes were evaluated in terms of clinicolaboratory findings. The shock index (SI; the patient’s heart rate [HR] divided by systolic blood pressure [SBP]), hemoglobin (Hb), hematocrit (Ht), and platelet (Plt) levels, activated partial thromboplastin time ratio (APTT-R), and prothrombin time-international normalized ratio (PT-INR) were assessed. Patients who underwent TAE were examined. Mortality within 30 days after the onset of CRSH was also retrospectively evaluated.
Statistical analysis
The relationship between hematoma features on CT and clinicolaboratory outcomes were assessed using the Mann–Whitney U test for continuous variables and Fisher’s exact test for categorical variables. All statistical analyses were performed using Statcel4 (OMS Publishing Inc., Saitama, Japan). P values <0.05 were considered statistically significant.
Results
Patient characteristics
The present study identified 47 patients with CRSH meeting the inclusion criteria identified in our database during the study period. The patient characteristics are summarized in Table 1. CT allowed a rapid diagnosis of soft-tissue hematoma in all cases. Most hematomas were located in the iliopsoas muscle (53%), rectus abdominus muscle (26%), and perirenal space (13%). In terms of the etiology of CRSH, anticoagulant-related hematoma accounted for 72%, and bleeding diathesis, including disseminated intravascular coagulation (DIC), accounted for 28%. CECT was performed in 30 patients and extravasation was found in 16 patients. All patients were initially treated with fluid infusion and normalization of coagulation parameters was attempted.
Baseline characteristics of all patients with coagulopathy-related soft-tissue hematomas (n = 47).
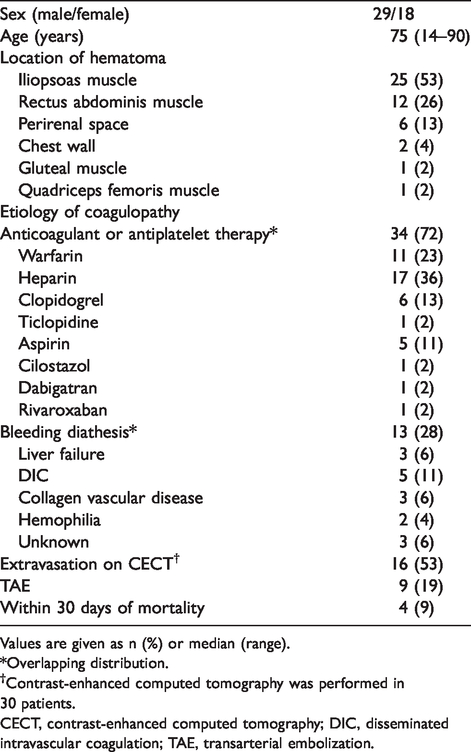
Values are given as n (%) or median (range).
*Overlapping distribution.
†Contrast-enhanced computed tomography was performed in 30 patients.
CECT, contrast-enhanced computed tomography; DIC, disseminated intravascular coagulation; TAE, transarterial embolization.
Indications for TAE were discussed between interventional radiologists and the attending physicians of each case. Nine patients were treated with TAE in an emergency setting. In these nine patients with TAE, extravasation on CECT was noted in eight patients. The remaining patient underwent TAE because of unstable vital signs, although extravasation was not observed. Among TAE patients, an additional surgical procedure was subsequently performed in one patient to remove an iliopsoas hematoma that caused nerve palsy after the bleeding had ceased.
On the other hand, 38 patients underwent conservative therapy with monitoring of clinical and laboratory findings. In these 38 patients, CECT was performed in 21 patients and extravasation was observed in eight patients. Among all 47 patients, four patients suffered mortality within 30 days, and the causes of death were cerebral hemorrhage (n = 2), heart failure (n = 1), and septic shock (n = 1), respectively. There was no mortality related to progressive CRSH.
Morphological features of the hematoma
The hematomas of all 47 patients were classified based on the morphological features on CT images. Fluid level and non-fluid level patterns were observed in 28 (60%) and 19 (40%) patients, respectively. The comparison between morphological patterns and clinicolaboratory outcomes are summarized in Table 2. Clinicolaboratory outcomes, including SI, Hb, Ht, Plt, APTT-R, and PT-INR, showed no significant differences between the two patterns. However, the use of anticoagulant/antiplatelet therapy and extravasation on CECT were significantly correlated with the fluid level pattern. Follow-up CT images were available for 36 of the 47 patients. Changes in the morphological pattern of the hematoma were observed in six patients. Transition from a fluid level pattern to a non-fluid level pattern was observed in four patients, while the opposite change was observed for two patients (Fig. 3).
Comparison between fluid level and non-fluid level patterns.

Values are given as n (%) or median (range).
*CECT was performed in 30 patients.
†Follow-up CT (1–20 days later) was performed in 36 patients.
APTT-R, activated partial thromboplastin time ratio; CECT, contrast-enhanced computed tomography; Hb, hemoglobin; Ht, hematocrit; Plt, platelet; PT-INR, prothrombin time-international normalized ratio; SI, shock index.
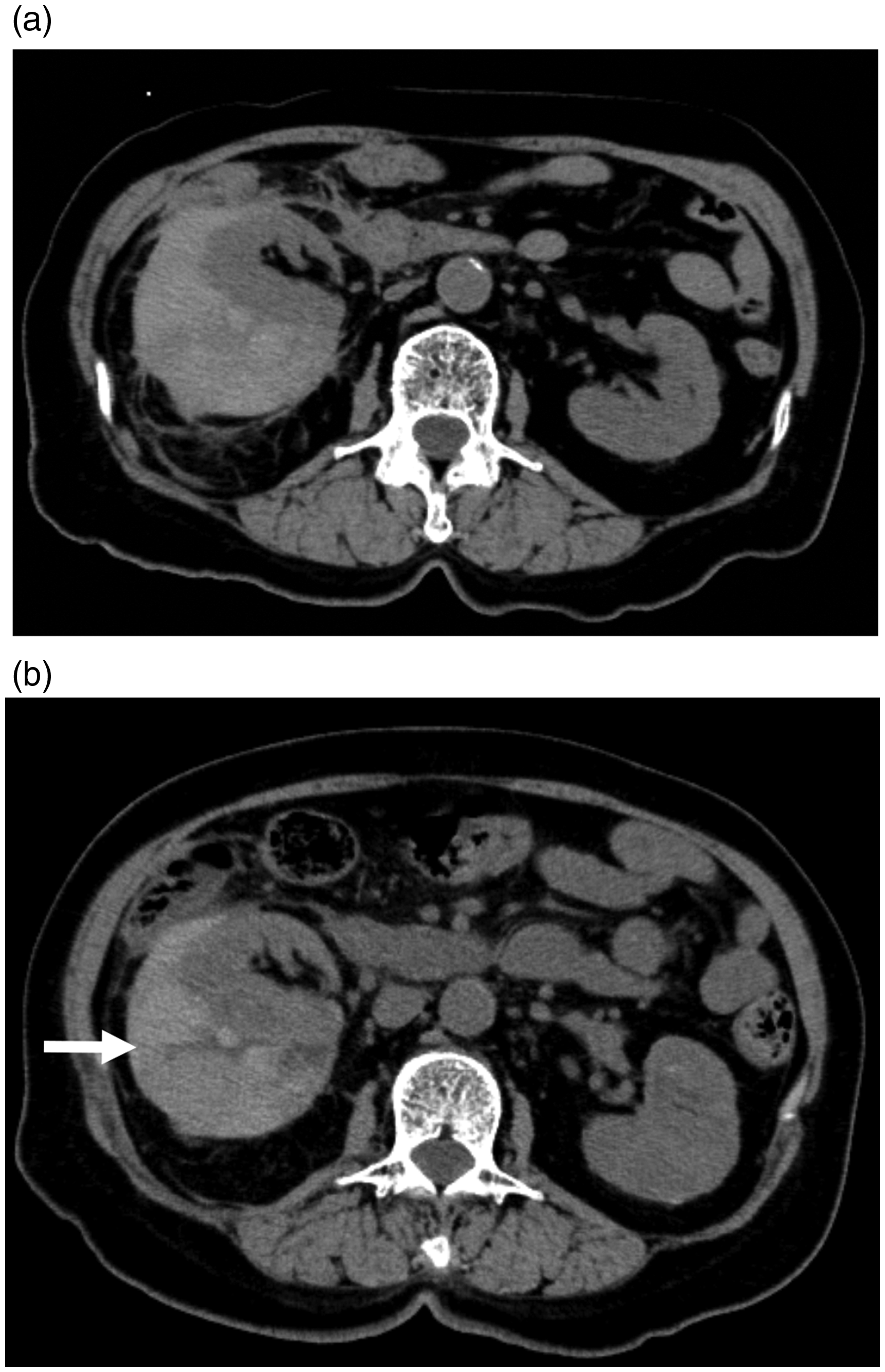
A 76-year-old woman treated with dabigatran for atrial fibrillation, visited the hospital because of abdominal pain. (a) Axial unenhanced computed tomography showed right perirenal space hematoma, which had no cellular-fluid levels (non-fluid level pattern). (b) On the follow–up CT (two days later), this non-fluid level pattern changed into a fluid level pattern (arrow). CT, computed tomography.
Extravasation of the hematoma
Among the 47 patients, the presence of extravasation was evaluated in 30 patients in whom CECT was performed (Table 3). The clinicolaboratory outcomes, including SI, Hb, Ht, Plt, APTT-R, and PT-INR, showed no statistically significant difference in the comparison of hematomas with and those without extravasation. On the other hand, only anticoagulant therapy was significantly correlated with hematomas with extravasation.
Comparison of hematomas between with and without extravasation on CECT.

Values are given as n (%) or median (range).
APTT-R, activated partial thromboplastin time ratio; CECT, contrast-enhanced computed tomography; Hb, hemoglobin; Ht, hematocrit; Plt, platelet; PT-INR, prothrombin time-international normalized ratio; SI, shock index.
Discussion
Coagulopathy-related hemorrhage commonly involves soft-tissue compartments, such as the rectus sheath or the iliopsoas muscle, and abdominal viscera are less commonly the sites of coagulopathic hemorrhage (1,18). The pathophysiology of coagulopathy-related hemorrhage is unclear, but it is assumed that the disturbance of physiological coagulation pathways and microangiopathy causes the bleeding (11,19,20). Moreover, micro-trauma (closed glottis straining, muscle contractions) could even trigger bleeding (3). Bleeding points usually involve multiple small branches from various territories concurrently (3,5), supporting this pathophysiology.
CRSH includes hemorrhage due to anticoagulation or bleeding diatheses. In our study, anticoagulation accounted for 72% of CRSHs. The continued increase in the prescription of various anticoagulants and antiplatelets has led to the increase in the incidence of CRSH (11). However, the symptoms of CRSH are non-specific and the diagnosis of CRSH is challenging. Furthermore, the management for CRSH is highly dependent on the local settings and remains controversial.
The present study was a single-institution retrospective analysis of CRSH, comparing CT findings and clinical severity. Upon morphological analysis of CRSH, the fluid level pattern was observed in 60% of cases in the present study. This fluid level pattern consists of cellular-fluid level caused by the stratification of heavier cellular elements and supernatant serous fluid; this pattern is reported to be a highly sensitive (87%) marker of coagulopathic hemorrhage (1,2,18). When CECT detects extravasation in the CRSH, the contrast medium was observed at the boundary between the fluid and cellular components (21). Ibukuro et al. (21) explained this phenomenon based on the specific gravity of each component and the contrast medium in liquefied hematoma. They called this extravasation a “signal flare phenomenon,” which is a significant sign indicating active bleeding in CRSHs. In the present study, several clinicolaboratory factors were compared between the fluid level pattern and non-fluid level pattern. We found that both anticoagulation and extravasation on CECT were significantly associated with the fluid level pattern compared to the non-fluid level pattern (P < 0.05). Based on these findings, the hematomas with a fluid level pattern are assumed to involve more liquid and it would be more difficult to achieve hemostasis in these hematomas than in those with the non-fluid level pattern. Therefore, we speculated that the fluid level pattern hematoma is more strongly related to clinical morbidity. However, other clinicolaboratory findings, such as the SI, Hb, Ht, Plt, APTT-R, and PT-INR, showed no statistically significant difference between these two patterns. It could be speculated that the reasons are as follows. First, soft-tissue hematoma has a self-tamponade effect that limits the expansion into the muscular component. Therefore, active bleeding might not necessarily result in severe blood loss (22). Second, the bleeding point is a distal branch of micro-vessels in the case of CRSH. Unlike traumatic hematoma, blood loss via CRSH is thought to be slower. Accordingly, this situation would not induce clinical severity. Third, the fluid level and non-fluid level patterns might potentially be related to the same hemorrhage, and the formation of these two patterns might depend on the speed of the initial bleed. In the present study, morphological transitions between these patterns were observed in some cases.
For the diagnosis for CRSH, CT plays an important role in detecting the hematoma and evaluating the extension of the hematoma (23). Furthermore, extravasation on CECT suggests active bleeding. However, extravasation on CECT cannot detect all active bleeding because coagulopathy-related bleeding is intermittent and is influenced by spasm, hypotension, and soft-tissue tamponade in elderly atherosclerotic patients (8,9,11,24). In our comparison of CRSHs with and without extravasation, there was no significant difference in clinicolaboratory factors. Based on our results, the extravasation in CRSH noted on CECT was not related to clinical severity, and the extravasation in CRSH was assumed not to have a greater clinical impact, unlike the extravasation in traumatic injury. Therefore, both CRSHs with and without extravasation should be observed carefully in the same way. Nevertheless, the usefulness of TAE has been reported, CRSH is associated with a poor prognosis and Touma et al. (11) reported an all-cause 30-day mortality rate of 22.7% in their systematic review. When physicians encounter patients with CRSH, attention should be paid to the underlying morbidity, in addition to the bleeding.
The present study has some limitations. First, the present study was a retrospective analysis at a single institution and involved a small sample size. Therefore, the results are of limited clinical utility. Second, some recent advances in anticoagulant therapy could not show abnormal laboratory coagulation findings. Therefore, coagulation findings might not be suitable factors for the evaluation of clinical severity. Third, fluid level and non-fluid level patterns might not appear as distinctly different entities in the morphological analysis of CRSH, because transitions between patterns can occur over a longer follow-up period. Finally, patient activity before the CT examination may have affected the formation of these patterns. Further experimental studies should investigate the mechanisms underlying this morphological difference.
In conclusion, soft-tissue hematoma with a fluid level pattern suggests anticoagulant therapy-induced hemorrhage, and it tends to be associated with extravasation on CECT. However, extravasation does not have a statistically significant correlation with either vital signs or laboratory findings. Therefore, the management strategy remains the same for lesions with the fluid level pattern and those with the non-fluid level pattern. The underlying co-morbidity as well as the management of hemorrhage should be kept in mind. However, larger studies will be needed to confirm the management of CRSH.
Footnotes
Acknowledgements
The authors thank Yasunobu Nakamura (Department of Medical Statistics, Satista Co., Ltd, Uji, Japan, www.satista.jp) for his assistance with statistical analysis and to Editage (![]() ) for English language editing.
) for English language editing.
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.