
Abstract
Background
There is no standardized brain computed tomography (CT) reference line that can be determined on both scout and reformatted sagittal CT images. Here, a tangential line from the anterior edge of the lower eyelid to the inner table of the occipital base (LEL/O line) appears nearly parallel to the Talairach–Tournoux (T/T) line, which shows a consistent intracranial anatomical relationship among subjects, and acts as a standard reference line for magnetic resonance (MR) imaging.
Purpose
To quantitatively validate the LEL/O line as a new standard brain CT reference line.
Material and Methods
We measured: angle 1 = the LEL/O line on scout images from the LEL/O line on parasagittal CT images (n=93); and angle 2 = the LEL/O line on scout images from the T/T line on high resolution midsagittal MR images (n=97). Angles in a clockwise direction were defined as positive and were expressed as mean±SD with the 95% confidence interval (CI) of the SD. Angle 2 was measured independently by two observers and intraclass correlation coefficients (ICCs) were calculated.
Results
Angle 1 was –0.4°±1.2° (95% CI of SD 1.1°–1.5°); angle 2 was –0.4°±2.0° (95% CI of SD, 1.8°–2.4°). The ICC in the angle 2 measurement was 0.780 (P<0.001), which indicated high inter-observer reliability.
Conclusion
The LEL/O lines on scout and parasagittal CT images show practically the same gradient, and these LEL/O lines are almost parallel to the T/T line. Use of the LEL/O line either for direct scanning or reformation can minimize intra- and inter-subject variations on CT images and mismatch between CT and MR images.
Keywords
Introduction
The orbito-meatal (OM) line, which was originally defined according to external soft-tissue landmarks (i.e. the lateral canthus and center of the external auditory meatus), used to be the traditional reference line utilized for computed tomography (CT) of the brain. To create images referencing this line, the technologist needs to adjust the angle of the individual’s head and tilt the CT gantry so that the guide light beam connects the landmarks demarcating the line. However, this procedure is rarely used these days because of the following drawbacks: (i) it is often difficult to obtain the desired angle between the individual’s head and the gantry; and (ii) the scout image, which is vital to the functioning of the autoexposure control and organ-based tube current modulation (which reduces the output dose to the eye lenses), cannot be obtained with a tilted gantry (1,2).
Nevertheless, the scout images, from which the scanning angle can be determined, do not allow identification of the OM line landmarks. Furthermore, the angle for the axial CT images has been frequently determined on reformatted sagittal CT images using the multiplanar reformation (MPR) technique in recent years. Therefore, to obtain consistent axial images, a reference line, which can also be readily drawn on sagittal CT images, is essential.
However, from our perspective, a standardized axial reference line that can be determined on both the scout and sagittal CT images has not yet been established, and the section angles are precariously determined by technologists. In fact, the section angles can vary significantly among technologists even in the same institution. The variation interferes with quantitative analysis, even when comparing images of the same subject obtained at different time points (3,4).
A tangential line from the anterior edge of the lower eyelid to the inner table of the occipital base (LEL/O line) can be determined on both scout and parasagittal CT images (Figs. 1a, 1b, and 2a). Moreover, as the occipital base is flat in the mediolateral direction, the LEL/O line on a scout image appears to correspond to that on a parasagittal CT image. We use the LEL/O line as a reference line for brain CT at our institution and find that it provides consistent images with a regular section angle. The importance of using a consistent section angle is illustrated in Fig. 3.

(a) A tangential line from the anterior edge of the lower eyelid to the inner table of the occipital base (LEL/O line) and a tangential line from the nasolabial junction to the inferior aspect of the sella turcica (NS line) on a scout image. (b) The LEL/O line on a parasagittal CT image of the same individual. (c) The LEL/O line (projected from the parasagittal image) and the NS line on a midsagittal CT image of the same individual.
Furthermore, the LEL/O line determined on parasagittal magnetic resonance (MR) images (Fig. 2b) appears to be almost parallel to the Talairach–Tournoux (T/T) line (the original anterior commissure [AC]/posterior commissure [PC] line) that passes through the upper edge of the AC and the lower edge of the PC (Fig. 2c). It is well recognized that the T/T line-referenced images maintain a consistent intracranial anatomical correlation among subjects (i.e. inter-subject consistency). In addition to intra-subject consistency, inter-subject consistency is important to ensure the characterization of pathological conditions in imaging, which is why the T/T line is used as a standard reference line for routine clinical MR imaging (MRI) and in neuroscience research (3–9).

(a) A tangential line from the anterior edge of the lower eyelid to the inner table of the occipital base (LEL/O line) and a tangential line from the nasolabial junction to the inferior aspect of the sella turcica (NS line) on a scout image. (b) The LEL/O line on a parasagittal T2-weighted image of the same individual. (c) The LEL/O line (projected from the parasagittal image), the Talairach–Tournoux (T/T) line and the NS line on a mid-sagittal T2-weighted image of the same individual.
We hypothesized that the LEL/O line could be used as an alternative to the OM line as the standard reference line for brain CT. The aim of the present study was to validate the use of the LEL/O line by quantitatively demonstrating that the LEL/O lines are similar on scout and parasagittal CT images, and that the LEL/O line closely approximates the T/T line.
Material and Methods
Participants
Our Institutional Review Board approved the study protocol (No. 28–35). The requirement for informed consent was waived in view of the retrospective nature of the study.
Images suitable for analysis were retrieved from our PACS database and consecutively reviewed. CT scout images with incorrect head positioning (i.e. roll and yaw rotations) and MR images with blurring artifacts or intracranial lesions causing a mass effect on midline structures were excluded. The images of 190 participants (102 boys/men, 88 girls/women; age range = 3–95 years; mean age ± SD = 49.8 ± 26.0 years) which were taken during 2016–2018 were used in the analysis.
Image acquisition
The CT equipment used was a 16-detector or 64-detector row CT scanner (Somatom Emotion 16; Siemens Healthcare Erlangen, Germany or Aquilion TSX-101A; Toshiba Medical, Tochigi, Japan). Lateral scout images were obtained at tube settings of 120–130 kV and 25–50 mAs and were displayed using a wide window-width setting.
Sagittal CT images were reformatted from axial 0.75-mm sections obtained with the following technical parameters: collimation = 128 × 0.6 mm; interval = 0.4 mm; pitch = 0.55; 120 kV; and 530 effective mAs.
MRI was performed with either a 3-T or 1.5-T scanner (Achieva or Ingenia; Philips Medical System, Best, The Netherlands). The sagittal images analyzed were T2-weighted (T2W) images (fast spin-echo; TR/TE = 3000–5600/80–110 ms) obtained with the following imaging parameters: section thickness = 3–5 mm; field of view [FOV] = 230 × 230 mm; matrix size = 256 × 256; and number of excitations (NEX) = 1–3.
Co-registration between scout images and sagittal CT/MR images
A tangential line from the nasolabial junction to the inferior aspect of the sella turcica (NS line) was established as an angular benchmark to co-register between the scout images and sagittal CT/MR images (Figs. 1a, 1c, 2a, and 2c). The location of these NS line landmarks can be pinpointed on scout images and midsagittal CT/MR images. Furthermore, the two-dimensional (2D) position of these landmarks remains fixed on serial sagittal CT/MR images, so the NS line ensures accurate co-registration between 2D scout images and sagittal CT/MR image datasets.
Angle measurements
LEL/O line
The following angles were measured, depending on the images available for each individual: 1 = the LEL/O line on scout images from the LEL/O line on parasagittal CT images (n = 93; Fig. 1); and 2 = the LEL/O line on scout images from the T/T line on midsagittal T2W MR images (n = 97; Fig. 2a, 2c).
Angle 1 (i.e. the LEL/O line on scout images from the LEL/O line on parasagittal CT images) was measured by retrospective review of data from consecutive individuals who underwent CT studies for head trauma, performed during a six-week period at our institution. The LEL/O line was determined on the parasagittal CT images that depicted the vicinity of the origin of the optic nerve (Fig. 1b) and then projected onto the mid-sagittal CT images, where the angle between the LEL/O line and the NS line was measured (Fig. 1c). This angle was compared with the angle between the LEL/O line and the NS line on scout images (Fig. 1a).
Angle 2 (i.e. the LEL/O line on scout images from the T/T line) was measured by retrospective review of data from consecutive individuals who underwent both CT and MR studies for suspected brain tumors/neurodegenerative diseases/cerebritis, performed during a 34-month period at our institution. As the AC and PC cannot be defined on mid-sagittal CT images, mid-sagittal T2W MR images, which provide the best contrast to delineate the AC and PC, were used to determine the T/T line gradient, and the angle between the T/T line and the NS line was measured (Fig. 2c). This angle was compared with the angle between the LEL/O line and the NS line on scout images (Fig. 2a).
OM line
Angles of the OM line from the T/T line was measured in 43 participants, i.e. a consecutive subset of the cohort (n = 97) in which angle 2 was measured, and in whom both the lateral canthus and the introitus of the external auditory meatus were clearly visible on the parasagittal T2W images. These OM line landmarks were projected onto the mid-sagittal T2W images. The OM line was then determined and the angle from the T/T line was measured.
Processing and statistical analysis
Angles were measured using a DICOM viewer (Radiforce RX340; EIZO; Hakusan, Japan; 21 inches, 5-MP screen) interlinked to a PACS.
The angles in a clockwise direction were defined as positive in accordance with previous studies (3,4,6,7,10) and are expressed here as the mean ± SD with the 95% confidence interval (CI) of the SD.
The full angular analysis was initially performed by a certified diagnostic radiologist (HI). Angle 2 (i.e. the LEL/O line on scout images from the T/T line) was reviewed independently by a radiological technologist (KY with six years of experience). The intraclass correlation coefficients (ICCs) were used to examine the inter-observer reliability.
Levene’s test was performed to evaluate the significance of differences in the SD values of angles and the multiplicity of the test was corrected using the Bonferroni method. A P value < 0.05 was considered significant.
The statistical analysis was performed using SPSS Statistics version 24 (IBM Corp., Armonk, NY, USA).
Results
LEL/O line
The angles were as follows: 1 = the LEL/O line on scout images from the LEL/O line on parasagittal CT images: –0.4° ± 1.2° (95% CI of SD = 1.1°–1.5°); and 2 = the LEL/O line on scout images from the T/T line: –0.4°±2.0° (95% CI of SD = 1.8°–2.4°).
The mean inter-observer difference in the angular measurement 2 was 0.4° ± 1.3°. The ICC was 0.780 (P < 0.001) which indicated high reliability.
OM line
The angle of the OM line from the T/T line was 1.6° ± 3.5° (95% CI of SD = 2.9°–4.4°) and showed a significantly larger SD than that of the LEL/O line (Levene’s test, P < 0.001; Fig. 4).
Discussion
The LEL/O line can be easily determined on correctly positioned scout images and parasagittal CT images and can thus contribute to reproducible brain CT images. The anterior edge of the lower eyelid on scout images can be clearly identified using a wide window-width setting. Although the inner table of the occipital base on scout images is rarely indistinct because of overlapping mastoid cells, the location is still identifiable because of its continuity with the other portion of the occipital bone.
The results of the present study revealed that the angular differences between the LEL/O line on scout images and the LEL/O line on parasagittal CT images are negligibly small. Therefore, the same axial images can be obtained either by direct scanning using the LEL/O line on scout images or by the MPR technique using the LEL/O line on parasagittal CT images. This enables standardization of axial imaging angles regardless of the procedure used for data acquisition.
We found that the LEL/O line gradient on scout images closely approximated the T/T line gradient with a small SD (i.e. inter-subject variations in angles from the T/T line) of 2.0° This indicates that LEL/O line-referenced brain CT images exhibit little inter-subject variation in brain anatomy. Concomitantly, LEL/O line-referenced brain CT images correspond to T/T line-referenced MR images, facilitating more accurate comparison and CT-MR fusion imaging (Fig. 3a and 3e).
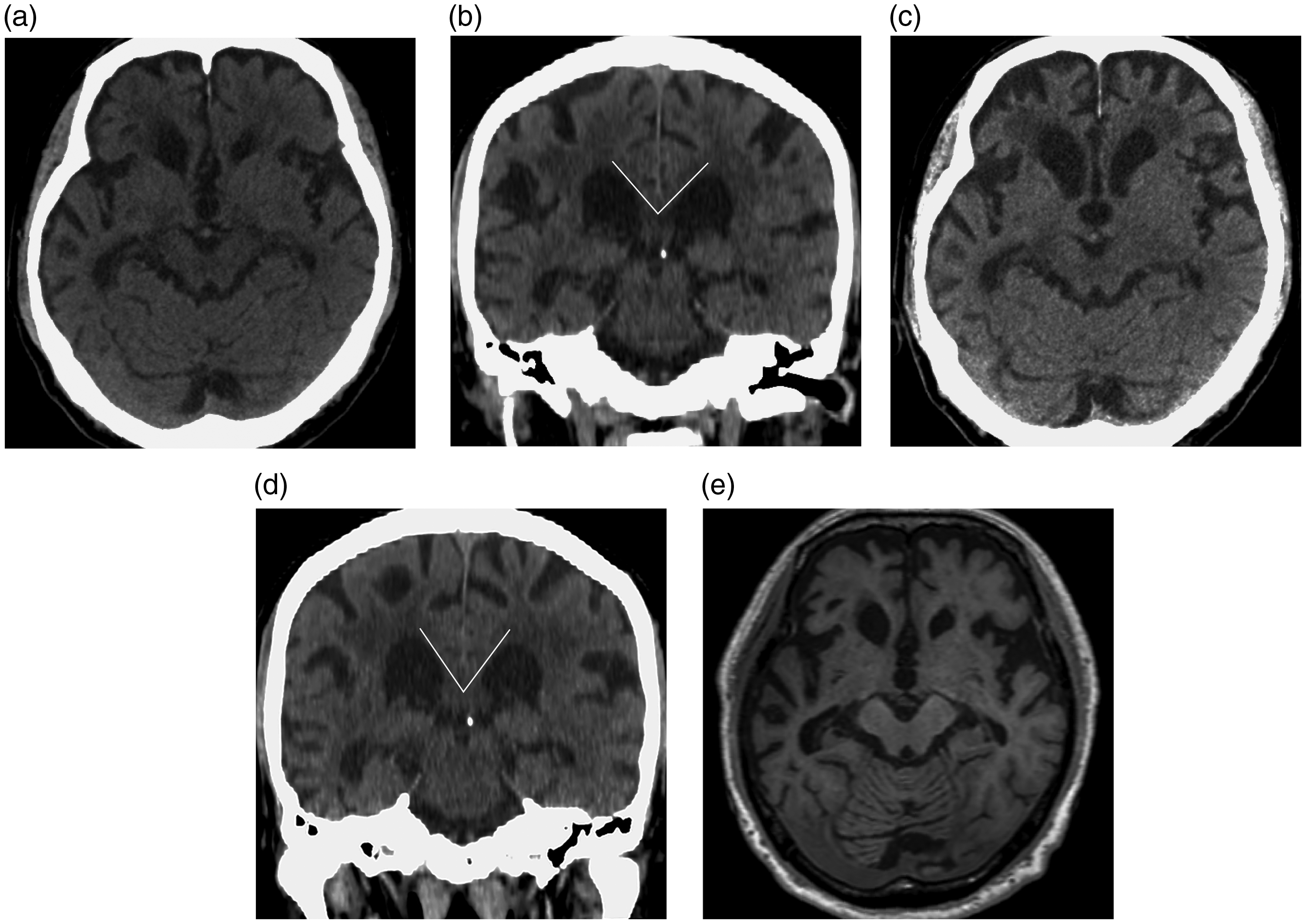
(a) Axial CT image traversing the aqueduct, referencing the lower eyelid to the inner occipital base (LEL/O) line of a patient with frontotemporal dementia. (b) Coronal CT image traversing the pineal gland, referencing a line perpendicular to the LEL/O line in the same patient. (c) Axial CT image traversing the aqueduct, referencing the orbito-meatal (OM) line in the same patient. The gradient of the OM line was determined from serial reformatted sagittal CT images. The inconsistency between images obtained referencing the LEL/O line (a) and OM line (c) interferes with quantitative analysis. (c) Coronal CT image traversing the pineal gland, referencing a line perpendicular to the OM line in the same patient. Note the difference in the callosal angle in comparison with (b). (e) Axial MR image traversing the aqueduct, referencing the Talairach–Tournoux (T/T) line of the same patient. This image corresponds closely to the LEL/O line-referenced axial CT image (a).

The graph shows the SD of the angle of the lower eyelid to the inner occipital base (LEL/O) line from the Talairach–Tournoux (T/T) line as well as of the angle of the orbito-meatal (OM) line from the T/T line. The error bars indicate the 95% confidence interval of the SD.
In the present study, the OM line, even when accurately determined (it is difficult to determine the OM line accurately in routine clinical settings), showed a significantly larger SD (i.e. inter-subject variations in angles from the T/T line), compared with the LEL/O line. The previous studies have also demonstrated that the OM line showed relatively an inconsistent relationship to the T/T line (3–7,10). For example, the OM line gradient (determined by using surface markers) has been reported steeper than the T/T line gradient, at an average 2.7° and a relatively large SD of 3.4° (10). Further studies on three-dimensional (3D) datasets of the Montreal Neurological Institute (MNI) brain reported an approximate difference of 9° (3,8).
To the best of our knowledge, two previous studies proposed reference lines that can be used on scout and sagittal CT images, as alternatives to the OM line. One study reported that the line along the superior cortical surface of the hard palate (HP line) correlates well with the T/T line (–12° ± 6.1°); the authors thus proposed a reference line tilted 12° clockwise from the HP line (4). However, the practical complexity of applying this line has prohibited its wide use. An additional study advocated the line connecting the external or internal occipital protuberances with the tuberculum sellae, because the gradient of this line is similar to that of the Schaltenbrand line (0.3° ± 4.5°) (6). The Schaltenbrand line is a modified AC/PC line that connects the middle of the AC and PC, although it is less commonly used than the T/T line (3,4,7,11). However, a considerable number of participants in our cohort showed unclear peaks of these protuberances, suggesting their unsuitability to be used as landmarks. Most importantly of all, these proposed reference lines mentioned above exhibit larger SD values (i.e. inter-subject variations in angles from the AC/PC line) compared with the LEL/O line.
One disadvantage of the LEL/O line and other reference lines discussed above is that the eye lenses are included in the radiation field when whole-brain direct scanning is performed using these lines. Direct scanning using the reference line that joins the orbital superior margin and the skull base (supra-orbital line) on scout images has been recommended in order to minimize radiation dose to the eye lenses, especially in cases requiring repeated brain studies and in children (12,13). In such cases, it would be theoretically easy to reformat and standardize these 3D data to LEL/O line-referenced images based on the angular difference between the supra-orbital line and the LEL/O line on scout images.
The present study has some limitations: first, it is difficult to accurately determine the anterior edge of the lower eyelid on scout images with rotated head positioning; and second, the small number of young children included as participants, in whom the craniocerebral structures are still in a formative stage.
In conclusion, the LEL/O line is a unique reference line that can be simply and accurately determined both on scout and parasagittal CT images; it parallels the T/T line closely as compared to other reference lines. Therefore, use of the LEL/O line either for direct scanning or reformation readily minimizes intra- and inter-subject variations on CT images and mismatch of CT/MR images.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.