
Abstract
Intracranial abnormalities are commonly suspected findings on antenatal ultrasound that require evaluation by magnetic resonance imaging. This review depicts multiple abnormalities imaged as a means to guide clinicians in proper diagnosis.
Introduction
Magnetic resonance imaging (MRI) is an important adjunctive tool used to evaluate the fetus in cases of suspected anomalies detected by ultrasound (US). Recent improvements in magnetic field strength and scan time in addition to parallel imaging techniques result in decreased acquisition times, optimized specific absorption rates (SAR), improved signal-to-noise ratio, and improved dielectric/non-uniformity artifacts. While 1.5-T imaging was long-considered the standard in fetal imaging, MRI of the fetus performed at 3-T is no longer uncommon (1–3).
The most common indications for fetal brain MRI are ventriculomegaly (VM), agenesis/dysgenesis of the corpus callosum, and posterior fossa abnormalities. Antenatal management of many of these disorders is typically expectant, but fetal MRI may provide information that can guide appropriate follow-up in the post-partum setting. Presented here are a series of intracranial abnormalities commonly encountered in mothers presenting with abnormal antenatal ultrasound exams.
Case series
Agenesis of the corpus callosum
The corpus callosum (CC) is the largest white matter commissure in the brain comprising the rostrum and genu anteriorly, the body centrally, and the splenium posteriorly. Since multiple chromosomal loci contribute to the formation and myelination of the corpus callosum, callosal dysgenesis and agenesis may be caused by an extensive list of genetic syndromes and mutations. There is a known association with Dandy-Walker malformation (DWM), fetal body anomalies, and aneuploidy (4). Often, callosal dygenesis occurs in association with interhemispheric cyst/lipoma. In addition, metabolic derangements, infection, and toxicity are known to contribute.
The reported incidence of callosal agenesis is approximately 1:4000 live births (5) with a male predominance. A child with agenesis of the corpus callosum may develop normally; however, the morbidity of callosal disorders is worsened in the setting of other anatomic abnormalities and/or syndromes.
Imaging findings are characteristic, with parallel orientation of the ventricles, “longhorn” sign on coronal imaging, and radially oriented midline sulci (Fig. 1). The third ventricle is high in location and communicates with the interhemispheric fissure. White matter loss and colpocephaly are common.
MRI findings of agenesis of the corpus callosum in a 30-week, 0-day fetus. (a) Sagittal HASTE image demonstrates absence of the corpus callosum (black arrow) and radial pattern of the parasagittal gyri. (b) Coronal HASTE image shows the “longhorn” configuration of the lateral ventricles (white arrows).
Aqueductal stenosis
Aqueductal stenosis (AS) causes VM of the lateral and third ventricles due to obstruction of outflow from the third ventricle into the fourth ventricle, which is normal in size. AS is the second most common cause of VM after Chiari malformation. It has been associated with neonatal mortality in up to 25% of affected fetuses (6).
On fetal MRI, the cerebral aqueduct is effaced (Fig. 2). The remaining findings relate to hydrocephalus, notably prominent lateral VM and, to a lesser extent, third VM. The septum pellucidum is absent or incomplete and the corpus callosum is often thinned and/or superiorly displaced.
MRI findings of aqueductal stenosis in a 38-week, 1-day fetus. (a) Sagittal HASTE image displays lack of a normal cerebral aqueduct and normal size of the fourth ventricle in the posterior fossa (black arrow). (b) Axial HASTE image demonstrates marked ventriculomegaly (white arrows).
Chiari 2 malformation
Chiari 2 malformation is characterized by downward translation of the cerebellar tonsils in the setting of a small posterior fossa and open neural tube defect with a lumbar myelomeningocele (Fig. 3). This condition is a common cause of antenatal and neonatal hydrocephalus and occurs in 0.5–1 per 1000 live births (7). MRI can demonstrate inferiorly displaced posterior fossa contents, small cerebellum with mass effect, hydrocephalus, frontal bone concavity, and myelomeningocele. Also better evaluated at MRI are the many associated anomalies which include agenesis of the corpus callosum and gray matter heterotopia. Fetal MRI has been shown to provide increased sensitivity and specificity compared to US with significant influence on management decisions (8).
MRI findings of Chiari 2 malformation in a 26-week, 5-day fetus. (a) Sagittal HASTE image reveals an open neural tube defect (black arrow) and downward translation of the cerebellar tonsils (white arrow). (b) Axial HASTE image shows enlarged ventricular atria (asterisks).
Dandy-Walker continuum
Dandy-Walker continuum is a disorder of the posterior fossa with classic DWM representing the most severe end of the spectrum (Fig. 4). In classic DWM, there is complete or partial vermian agenesis, cystic dilatation of the fourth ventricle, large posterior fossa, and elevated torcula. Mild vermian hypoplasia may be considered the least severe end of the continuum. The term “Dandy Walker variant” is vague and thus less utilized. Dandy-Walker continuum disorders are often components of other syndromes (e.g. Walker-Warburg, Meckel-Gruber, etc.). The reported incidence is 1:30,000 (9).
MRI findings of Dandy-Walker continuum in a 21-week, 5-day fetus. (a) Sagittal HASTE image exhibits a small vermis (white arrow) with expansion of the posterior fossa. (b) Axial HASTE image reveals communication between the fourth ventricle and prominent posterior fossa cerebrospinal fluid (black arrow).
Elements in describing Dandy-Walker continuum disorders in utero include determining the extent of vermian maturity and assessing the tegmento-vermian angle. Differential considerations include persistent Blake pouch cyst and mega cisterna magna, which some consider even milder forms of the continuum, as well as arachnoid cyst (10).
Cephalocele
Cephaloceles occur when there is a calvarial defect with extracranial extension of intracranial structures covered by skin (Fig. 5). Meningoencephaloceles (extracranial extension of brain, meninges, and cerebrospinal fluid [CSF]) are a common subtype. Cephaloceles account for 10%–20% of dysraphisms, and the estimated prevalence is 0.8–4.0 per 10,000 live births (11). Most cases are sporadic; however, there are genetic and non-genetic syndromes associated with cephaloceles in addition to environmental exposures. The majority (80%) are occipital in location, though parietal and midline frontal cephaloceles have been seen (12).
MRI findings of encephalocele in a 35-week, 1-day fetus. (a) Sagittal HASTE image demonstrates meninges and brain tissue (white arrow) protruding through a posterior calvarial defect. (b) Axial HASTE image exhibits extension of the supratentorial brain through the occipital calvarial defect (black arrows).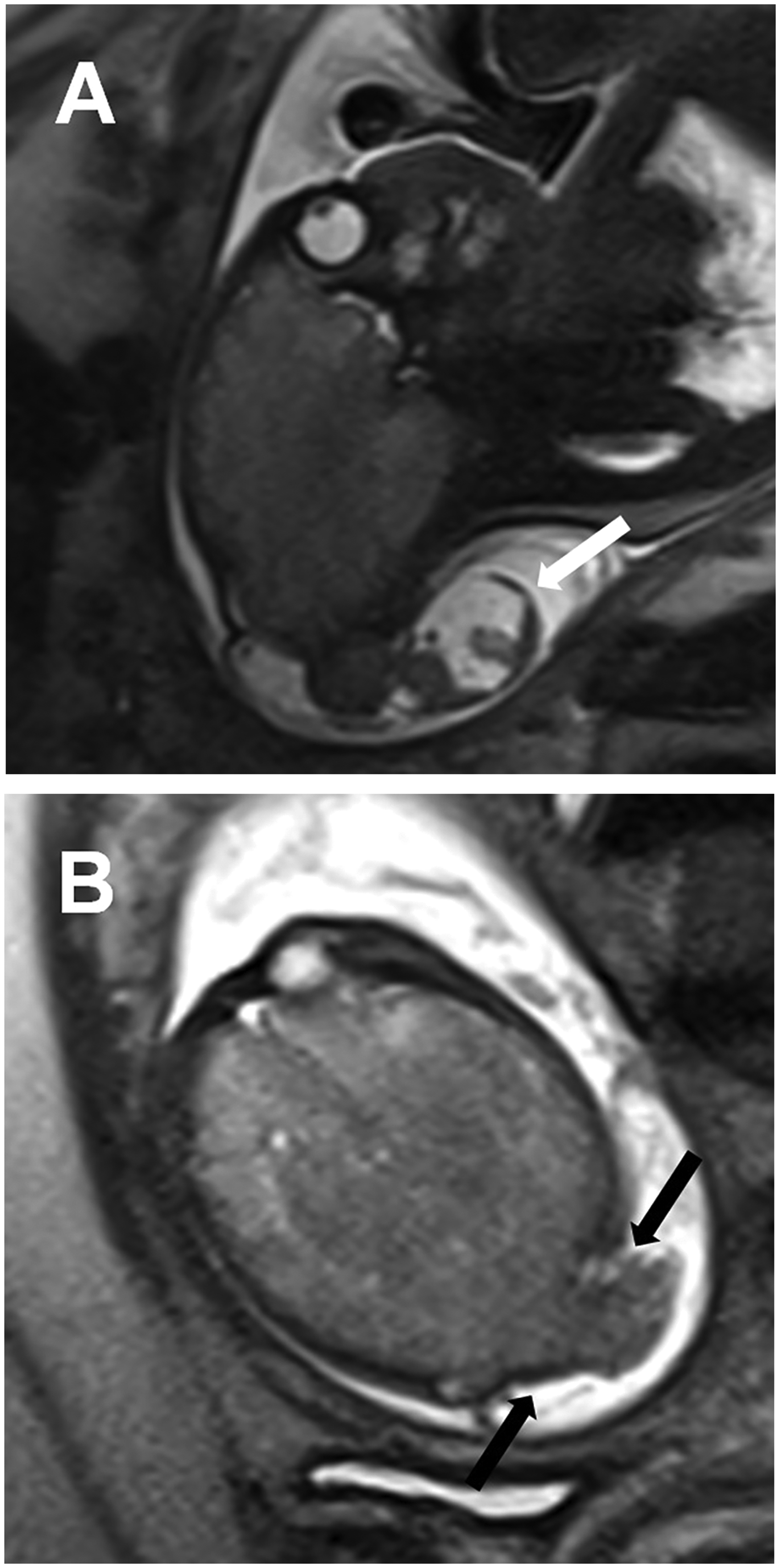
Prognosis relates to the amount and type of herniated intracranial contents. MRI has proven a useful adjunct to US to evaluate contents of the sac, including herniated dural venous sinuses, and to search for associated anomalies, which are present in 50% of cases. Diffusion-weighted imaging should be included to evaluate for ischemia.
Holoprosencephaly
Holoprosencephaly occurs when there is failed or incomplete cleavage of the prosencephalon (Fig. 6). MRI is indicated to define the severity of fusion and associated anomalies. The most severe form is alobar holoprosencephaly, which manifests as a primitive monoventricle, absent interhemispheric fissure, and thalamic fusion. In semilobar holoprosencephaly, the anterior frontal lobes are fused, but the posterior interhemispheric fissure is present, and there is at least partial fusion of the thalami. Rudimentary frontal horns are present. In lobar holoprosencephaly, only the basal frontal lobes are fused and the thalami are separated. There is also a form known as middle interhemispheric fusion (syntelencephaly) in which the poster frontal and parietal lobes are fused (13).
MRI findings of holoprosencephaly in a 34-week, 2-day fetus. (a) Axial HASTE image reveals fusion of the frontal lobes across the midline (white arrow). (b) Coronal HASTE image also depicts fusion of the frontal lobes across the midline (white arrow).
Holoprosencephaly has a prevalence of approximately 1 in 250 conceptions and an incidence of 1 in 10,000–20,000 live births (14). Multiple genetic mutations are known in this disorder, and many affected patients have an additional syndromic condition (15). Midline facial anomalies are common. In utero diagnosis should prompt karyotyping and genetic counseling.
Hydranencephaly
Hydranencephaly is reflected by a complete or near absence of cerebral cortex, generally due to circulatory compromise (e.g. anoxia, thrombus, toxin, twin–twin transfusion) (Fig. 7). The posterior fossa structures, thalami, and interhemispheric falx remain intact, and macrocephaly is common due to the persistent production of CSF. The majority of cases are sporadic, and the incidence is 1 in 10,000 births (16). MRI can aid in distinguishing this entity from hydrocephalus, schizencephaly, and holoprosencephaly, which are differential considerations.
MRI findings of hydranencephaly in a 31-week, 5-day fetus. (a) Coronal HASTE image reveals intact thalami (white arrow). (b) Axial HASTE image shows near complete absence of the cerebral hemispheres (black arrow).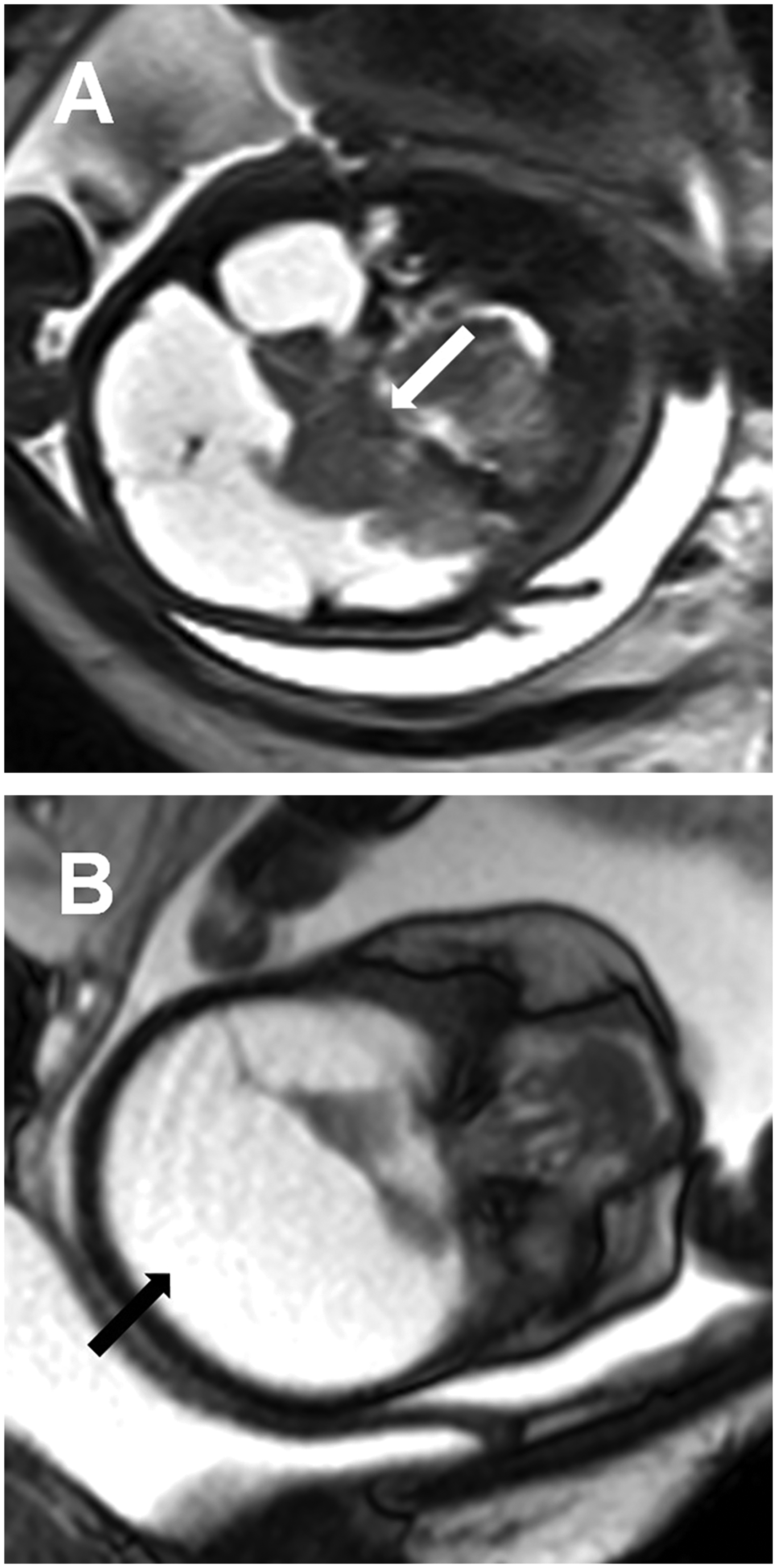
Schizencephaly
Schizencephaly refers to a cleft in the brain parenchyma extending from the ependymal surface to the pia mater and is commonly segregated into two types: open-lipped and closed-lipped. Open-lipped schizencephaly refers to a schizencephalic defect in which the cleft walls are separated by a CSF-containing cavity (Fig. 8). The cleft walls are apposed in closed-lipped schizencephaly. The walls of the cleft are lined by gray matter. Schizencephaly is distinguished from encephaloclastic porencephaly in which the cavity is lined by white matter. This can often be discerned by MRI. It is caused by an abnormality of neuronal migration and may be the result of an insult early in development; however, some associations with genetic mutations have been identified.
MRI findings of schizencephaly in a 37-week, 0-day fetus. (a) Axial HASTE image demonstrates prominent cerebrospinal fluid within a cleft in the right cerebral hemisphere which communicates with the right lateral ventricle (white arrow). (b) Coronal HASTE image reveals that the parenchymal cleft is lined by gray matter (black arrow).
The incidence of schizencephaly is approximately 1 in 65,000 live births (17). There are associations with other abnormalities including septo-optic dysplasia (17). It can be unilateral or bilateral with the frontal and parietal lobes as the most common sites (18). As is the case with other brain malformations, the extent of symptoms depends on the location and extent of the disease. Seizures, motor disorders, and developmental delay are common.
In conclusion, MRI is an important complementary tool in the evaluation of fetal brain malformations. Precise and accurate diagnoses in these patients is important for treatment planning and parental counseling.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.