
Abstract
We present the case of a 53-year-old woman with a known history of hereditary multiple exostosis disease referred for further imaging work-up after ultrasound and computed tomography leading to the suspicion of malignant transformation of an osteochondroma (exostosis) located on the posteromedial aspect of the right proximal femur. Imaging examinations suggested an ischiofemoral impingement resulting in a secondary bursitis associated with the development of an internal lipoma arborescens. This rare association explained the complexity of the diagnosis. Magnetic resonance imaging (MRI) played a key role in correctly identifying this benign complication of the osteochondroma and in distinguishing those observations from a secondary exostotic chondrosarcoma. MRI findings were subsequently confirmed at surgery and pathological examination.
Introduction
Hereditary multiple exostosis (HME) disease is a well described condition characterized by the proliferation of multiple osteochondromas (OC) (1). It predisposes the patient to several secondary benign pathologies including growth disturbance, joint deformities, compression and impingement syndromes, as well as secondary malignancies. The main concern in HME patients is indeed the potential development of a malignant transformation of an OC. Ultrasound (US) and magnetic resonance imaging (MRI) are the imaging modalities of choice to assess patients with HME as well as for the work-up of a clinical suspicion of malignant degeneration characterized by an abnormal thickening of the cartilage cap (2–4). Nevertheless, MRI examination of the cartilaginous cap of the OCs may prove difficult or confusing, especially in case of soft-tissue anomalies adjacent to the tumor.
Ischiofemoral impingement (IFI) is now recognized as an often-overlooked cause of hip pain (5). The incidence of IFI has been shown to be higher in the HME population (6). This condition may lead to a reduced ischiofemoral space (IFS) with subsequent muscle entrapment and bursitis, which may be identified with MRI.
Lipoma arborescens (LA) is a rare benign intra-articular lesion usually described in the knee (7). It may be observed in association with chronic joint irritation and effusion of various origins. Rare observations were made within chronic bursitis (8,9). Its observation in the case of bursitis outside of an articulation supports the hypothesis of chronic inflammation inducing synovial hypertrophy and subsequent adipose differentiation (10).
We report the case of an extra-articular LA developed in a chronic bursitis associated with IFI due to a femoral OC in a patient with HME disease. The patient had been referred because of the appearance of a mass in the proximal thigh and reduced hip mobility, leading to a high clinical suspicion of malignant transformation of an OC. MRI demonstrated the absence of an abnormal pathologic cartilage cap covering the OC, proved the IFI, and enabled the recognition of a “neo-bursitis” associated with the presence of an LA. This case underlines the key role of MRI to highlight the benign nature of the mass and to rule out malignant transformation in an exostotic chrondrosarcoma.
This uncommon association was confirmed at pathologic analysis after surgery had been performed due to an unrelated post-traumatic femoral neck fracture.
Case report
A 53-year-old woman was referred to our center for a suspicion of malignant transformation of an OC of the right proximal femur. She had a long history of HME disease with an extensive involvement of both hips, resulting in deformities and limited bilateral hip motion. She was limited in her walking ability and had to use crutches for longer walks. She had a history of previous resection of OCs at both knees. She had also been in remission for years having previously been treated for breast cancer.
More recently, she experienced a decrease in mobility of her right hip and, most importantly, observed the appearance of a mass in the anterior aspect of the proximal right thigh, which turned out to be painful at palpation. Physical examination confirmed the limited range of motion of the right hip, especially in extension and external rotation.
Initial radiological investigations performed in another institution showed multiple deformities related to HME disease and an OC of the right femoral neck (Fig. 1). US showed a hypoechoic mass developed on the anterior aspect of the proximal thigh (Fig. 2) with central fluid content and irregular peripheral wall (Fig. 2). Computed tomography (CT) scan of the pelvis and thighs confirmed the presence of a large mass, strengthening the hypothesis of a malignant lesion developed after degeneration of an OC (Fig. 3).
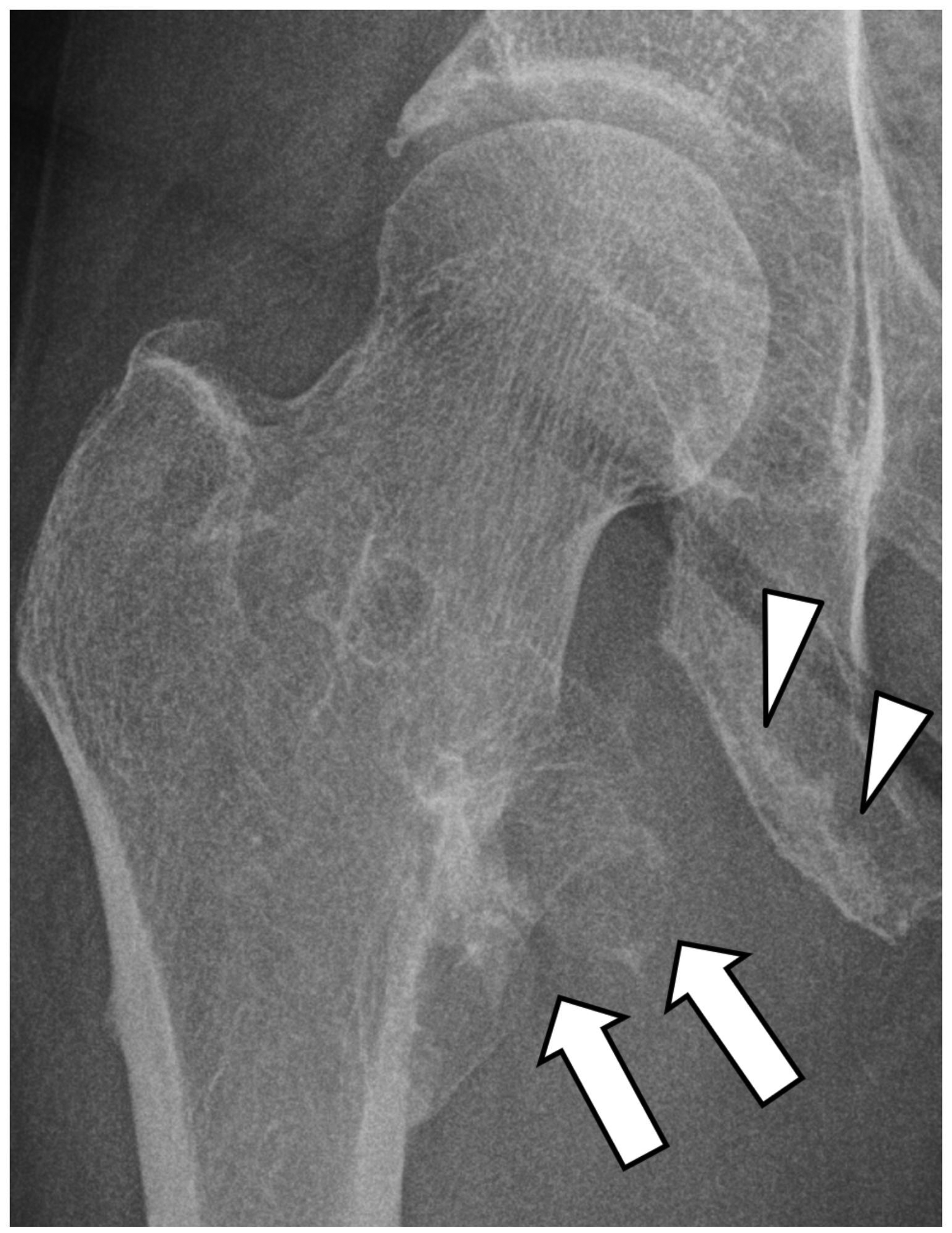
Radiograph of the right hip shows osteochondroma arising from the medial aspect of the femoral neck (arrows). Note subtle hyperostosis at the level of the ischial tuberosity (arrowheads).

Ultrasonography of the anterior aspect of the proximal thigh shows large fluid-containing collection, with thick wall (arrows) and heterogeneous hyperechoic proliferations on its deep aspect (arrowheads).

Initial transverse CT images (a, b) show a mass at the medial aspect of the proximal right femur, surrounding the base and tip of the osteochondroma (asterisk in (a)). Note the peripheral irregular wall of the mass with nodular components (arrowheads in (b)).
MRI of the pelvis and right thigh performed at our institution confirmed the presence of an OC arising from the posteromedial aspect of the right proximal femur (Fig. 4). This examination ruled out signs of a malignant transformation: there was no thickened cartilage cap covering the OC and no enhancing tumoral tissue close to the OC. This examination suggested a mechanical conflict between the femoral OC and the ischium, with a “pincer effect” on interposed soft tissue. This chronic impingement between the OC and the ischium explained the development of a chronic bursitis, with accumulation of abundant fluid on each aspect of the narrowed IFS. The observation of fatty villous proliferations within this fluid collection suggested the presence of an LA component within the bursitis. This IFI explained the walking limitation reported by the patient.

Coronal STIR MR image (a) and transverse T1 (b), T1–post-injection of contrast (c), and STIR (d) MRI of the pelvis and right hip shows fluid-filled collection between the femoral osteochondroma (arrows in (a)) and the ischial tuberosity (arrowheads). The fluid-filled collection presents irregular walls with fat signal peripheral nodular thickenings (arrowheads in (b, c)).
In the absence of suspicion of malignant transformation, the surgical resection of the OC and secondary bursitis was proposed to the patient. However, she preferred delaying the operation for personal reasons.
Three months later, the patient was transferred to our institution after a fall at home. X-rays and CT demonstrated a femoral neck fracture, partly involving the femoral OC. This was not considered a pathological fracture related to the OC or to the previously described mass that was still present and showed no change compared to prior examinations (Fig. 5). She was operated by a posterior approach to allow the complete removal of the OC and associated soft-tissue mass arising from the IFS. A total hip replacement was performed, as treatment for the femoral neck fracture and to restore mobility of the hip.

CT performed after a fall at home. Coronal (a) and transverse (b) reformatted images show a fracture of the femoral neck (arrows). Note that the fracture involves the base of the osteochondroma (arrowheads in (b)).
Pathological examination confirmed the radiological findings with the absence of malignant transformation of the OC (Fig. 6a) and exuberant subsynovial fatty proliferation resembling LA within the chronic bursitis (Fig. 6b). The macroscopic analysis revealed the concurrent observation of an OC measuring 6 × 4 × 2 cm, a bursitis consisting in a cavity surrounded by a thickened wall, containing fluid and multiple polypoid fatty components arising from the wall (Fig. 7a). This wall was described as a hyperplastic synovial membrane and the underlying tissue was composed of mature adipocytes embedded within a fibrous and vascular network (Fig. 7b). There were no signs of malignancy, neither within in the OC and its cartilaginous cap, or within adjacent soft-tissue abnormalities.

Pathologic correlation: macroscopy. (a) Global view of the resected specimen shows the wall of the bursitis removed at surgery, with heterogeneous parietal villous proliferations; note the yellow fatty appearance of this proliferation. The osteochondroma is visible at the left part of the picture. (b) Macroscopic view of fatty proliferations arising from the wall of the fluid-filled collection shows polypoid fat containing formations.

Pathologic correlation: microscopy. (a) Microscopic examination (hematoxylin and eosin [H&E]) of the osteochondroma shows well-differentiated thin cartilaginous cap. No sign of degeneration was present at the level of this cartilage cap (arrowheads). (b) Microscopic examination (H&E) shows a polypoidal proliferation of synovium (asterisk) and subsynovial generous quantities of fat with some loose fibrous tissue (arrows) and scattered congested vessels (arrowheads).
Discussion
Hereditary multiple exostosis (HME) disease is a rare skeletal disease predominantly inherited and linked to the mutation of tumor suppression genes EXT1 and EXT2 (11–13). It is usually diagnosed at the age of 3–12 years due to the presence of multiple OCs arising from the metaphysis of bones. The expression of the disease is variable: some patients may be asymptomatic while others may be heavily affected and present with short stature and growth deformities due to the presence of exostoses in shoulders, forearms, knees, ankles, pelvis, or spine (14). The disease may impact on the quality of life, global health, and be responsible for pain resulting from conflicts with adjacent muscles, vessels, nerves, or from reciprocal mechanical conflict between adjacent bony structures (15–17). In the present case, the conflict between the femoral OC and the ischium was responsible for the IFI and subsequent painful limp.
Bursitis may be associated with the lesion due to chronic impingement or friction, and may be detected as a newly appeared mass, in the present case observed between the femoral OC and the ischium and extending to the proximal portion of the thigh (18).
HME is associated with a significant risk of malignant transformation of OCs in exostotic chondrosarcomas during adulthood, with a lifetime risk of malignant transformation estimated to approximately 5% (12,16). Regular follow-up of the OCs, especially when located on the axial skeleton, is strongly recommended. A change in size or appearance of symptoms warrants immediate investigation. In this indication, US and MRI may be used (4). MRI is especially useful to analyze suspicious lesions and is the modality of choice to analyze the cartilaginous cap of the OC, which is thickened in case of malignant transformation (2,19). However, the distinction between a benign lesion and a low-grade secondary chondrosarcoma may be difficult (20).
Since its description by Johnson et al. (5), IFI has been recognized as a quite frequent but potentially overlooked cause of hip pain. MRI is the imaging modality of choice for a positive diagnosis (21). Several authors suggested the use of measurements to define the narrowing of the IFS and quadratus femoris space (QFS) with the association of quadratus femoris muscle edema upon MRI analysis. Threshold values of 15 and 10 mm have been suggested to define IFS and QFS, respectively. However, a high variability in these measurements does exist, mainly due to patient positioning (22). Moreover, imaging abnormalities are not always correlated with clinical IFI (23). Based on a meta-analysis, Singer et al. (24) proposed the following criteria to diagnose IFI: QF edema, narrowing of the IFS and/or QFS associated with ipsilateral hip pain.
HME disease represents a well-known cause of IFI, beside other conditions and morphological predispositions (6,25–30). In a case control study, Yoong et al. (6) demonstrated that IFI features were found on 62% of MRI studies performed in multiple exostosis patients with an IFS in the range of 0–21 mm. MRI is thus the imaging modality of choice to analyze the IFI in HME patients, as demonstrated by Duque Orozco et al. (31) in a pediatric population.
LA results from lipomatous and villous proliferation of the synovial membrane. It is characterized by fatty infiltration of the subsynovial connective tissue. It is usually described in the knee (32,33) but may be observed in the hip (34), shoulder (35), wrist (36), or elbow (37). The disease is monoarticular in most cases but involvement of several joints in the same patient has been described (36,38,39). Extra-/peri-articular location of LA, especially in bursae, such as in the sub acromial space or prepatellar bursa, has been more exceptionally reported (8,9,36,37,40). In some cases, LA may be associated with osteochondral loose bodies (41).
The etiology of LA is considered unknown. Several authors hypothesized that LA arises in osteoarthritic joints secondary to chronic inflammation inducing proliferation and hypertrophy of the synovial membrane with subsequent adipose differentiation (10). However, a few authors (42) reported cases of primary LA in younger patients without underlying osteoarthritic pathology. Recently, Chander et al. (36) highlighted a specific predisposition of the adipose tissue of the sub-synovial space of patients presenting with LA.
MRI findings of LA were described by Vilanova et al. (43) showing that MRI allowed a definite diagnosis of LA with characteristic hypertrophic adipose proliferation of the sub-synovial tissue especially when using fat-supressed or STIR sequences.
In conclusion, this case presented an unusual association. The different observations and their pathogenesis may be summarized as follows. The IFS was extremely narrowed and mechanical conflict was present between the femoral OC and the ischium. This chronic impingement led to the development of a secondary chronic bursitis and an internal LA. The resulting heterogenous mass raised the possibility of malignant transformation of an OC. MRI allowed the correct identification of the complex association of benign complications of this HME disease and ruled out malignant transformation of the OC, which was histopathologically proven.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.