
Abstract
Background
Ultrasound findings of shallow T2 gallbladder carcinoma (GBC) with a favorable prognosis are not known.
Purpose
To confirm the criteria for ultrasound diagnosis of shallow T2 GBC.
Material and Methods
A detailed analysis of ultrasound and pathological correlation was conducted in two patients with pT1 GBC and seven with shallow pT2 GBC (subserosal-invasion depth ≤ 2 mm) at our institution from January 1988 to December 2017.
Results
A polypoid gallbladder tumor with a deep hypoechoic area represented a papillary adenocarcinoma invading the subserosa accompanied by abundant fibrosis and lymphocytic infiltration. Two cases of pT1 GBC did not present a deep hypoechoic area, whereas all seven cases of shallow pT2 GBC did. One case of pT1b GBC and four cases of pT2 GBC showed conical thickening of the outermost hyperechoic layer, whereas one case of pT1a GBC and three cases of pT2 GBC presented no change of the layer thickness. All shallow T2 GBCs showing a conically thickened outermost hyperechoic layer provided good postoperative prognoses.
Conclusion
Ultrasound images of shallow T2 GBC show a deep hypoechoic area with conical thickening or unchanging of an outermost hyperechoic layer. The former demonstrates pulling up the top of the layer at first and then thinning later as carcinoma invades with enlargement of the hypoechoic area, whereas the latter thinning of the layer from the beginning. Polypoid gallbladder tumors with a deep hypoechoic area and a conically thickened outermost hyperechoic layer suggest shallow T2 GBC and may provide good postoperative prognoses.
Introduction
Patients with an early (pT1) gallbladder carcinoma (GBC), confined to mucosa or muscle layer, are provided good prognoses (1). Further, radical resection provides a favorable prognosis for patients with GBCs limited to shallow subserosal invasion (subserosal-invasion depth ≤2 mm: shallow pT2) (2) and ultrasound images of shallow T2 GBCs are currently gaining attention.
We presented two cases of shallow pT2 GBCs showing a papillary-infiltrating type and indicated the significance of a deep hypoechoic area (3,4). As far as we know, there has been no literature reporting similar cases. As we have experienced five similar cases and an interesting case of pT1b carcinoma thereafter, we intend to review the ultrasound images of shallow T2 carcinoma together with T1b carcinoma through a detailed comparative study between ultrasound and pathological findings to exhibit numeric values in depth of carcinoma invasion.
Material and Methods
A comparative analysis between ultrasound and pathology was conducted in nine cases: two with pT1 GBC (pT1a = 1; pT1b = 1) and seven with shallow pT2 GBC (papillary-infiltrating type = 5; flat-infiltrating type = 2) among the cases who received an ultrasound in our hospital and underwent radical surgical resection in our hospital or its affiliated hospital from January 1988 to December 2017. Mean age was 63 years (age range = 47–83 years) and five (55.6%) were men. Ultrasound depicted the gallbladder and the whole image of the lesion as much as possible, both in the short and the long axes. All resected specimens were opened on the opposite side of the lesion along the long axis and fixed in formalin. After fixation, eight specimens were sliced wholly stepwise along the long axis and one specimen along the short axis. This study remains confined to routine clinical practice with the patients’ consent.
Ultrasound was performed using a Toshiba SSA-260A unit with a 3.75-MHz convex transducer or a 7.5-MHz linear transducer, Toshiba SSA-340A unit with a 3.75-MHz or 3.7-MHz convex transducer, Toshiba SSA-770A unit with a T5.0-MHz convex transducer (Toshiba, Tokyo, Japan), and Olympus GF-UM240 with a 12-MHz radial transducer (Olympus, Tokyo, Japan). The number of ultrasound operators was five and only one operator was responsible for the final ultrasound diagnosis, namely, the first author.
Results
A polypoid gallbladder tumor with a deep hypoechoic area represented a papillary adenocarcinoma invading the subserosa accompanied by abundant fibrosis and lymphocytic infiltration. Two cases of pT1 GBC did not present a deep hypoechoic area, whereas all seven cases of shallow pT2 GBC did it. The limit of delineation with ultrasound of a deep hypoechoic area was 1–2 mm in thickness. A case of pT1b GBC and four of pT2 GBC showed conical thickening of the outermost hyperechoic layer, whereas a case of pT1a GBC and three of pT2 GBC presented no change in the layer thickness (Table 1).
Summary of nine patients with pT1 and shallow pT2 GBC.

*The thickness of subserosal invasion and that of subserosal fibrosis are measured in the specimen with the largest and/or deepest carcinoma invasion. The latter is estimated as the whole thickness of subserosal fibrosis including non-cancerous fibrosis.
†The case was positive for lymph node metastasis, dying of lung and lymph node metastasis.
pap, papillary type; pap-inf, papillary-infiltrating type; flat-inf, flat-infiltrating type; Gn, neck; Gb, body; Gf, fundus of the gallbladder.
Ultrasound and pathological correlation of the four cases were demonstrated in Figs. 1–4 (cases 1, 2, 6, and 9). Five cases (case 3–5, 7, and 8) have been previously published (5). Histopathological findings were described according to the Japanese classification of biliary tract cancers (6).

Case 1. (a) Transabdominal conventional ultrasound: a broad-based elevated lesion (arrowhead), 13 mm in diameter, adjacent to a nodule (adenomyoma, arrow) at the fundus. A deep hypoechoic area is not noted on the thickness-unchanged outermost hyperechoic layer. (b) Fixed specimen: an elevated lesion in the fundus adjacent to an adenomyoma. A white line shows the cross-section line, responsible to the loupe view (c). (c) Loupe view (H&E): a carcinoma (pap-tub1 >> tub2) confined to the mucosa adjacent to an adenomyoma (red circle), which is shown upside down to compare with ultrasound images (a).

Case 2. (a) Transabdominal ultrasound: a papillary protruded lesion, 30 mm in diameter, at the fundus (white arrow), which is inhomogeneously hyperechoic. In addition, there exists an outermost hyperechoic layer conically thickened but without a deep hypoechoic area on it. (b) Fresh specimen: a protruded lesion in the fundus. pT1a and pT1b denote invasion depths. A white line shows the cross-section line for the loupe view (c). (c) Loupe view (H&E): a carcinoma (tub1-tub2) at the fundus invading the muscle coat (pT1b). Note that the subserosal adipose layer beneath the lesion is conically thickened and free from carcinoma, fibrosis or lymph follicles. (d) Low power view (H&E): small nests of adenocarcinoma (white circle) invading the muscle layer.
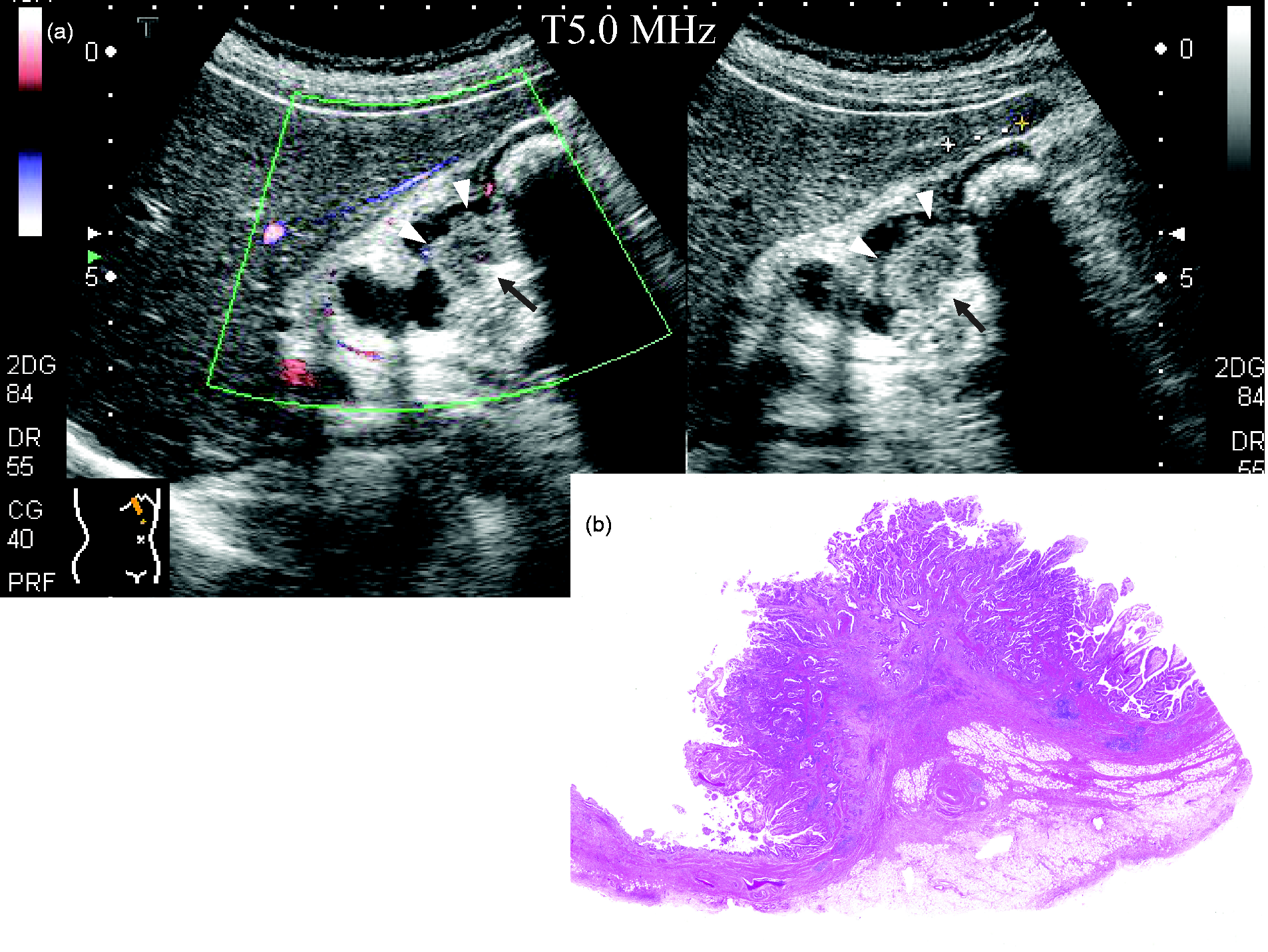
Case 6. (a) Transabdominal color Doppler ultrasound and conventional ultrasound: a broad-based elevated lesion (white arrowheads), 2 cm in diameter, on the peritoneal side of the body, accompanied by gallstones. Its shallow part is hyperechoic and its deep part hypoechoic with an outermost hyperechoic layer conically thickened beneath the lesion (black arrow). (b) Loupe view (H&E): a carcinoma (pap, tub1 > tub2 >> por), pT2, of the body; well-differentiated papillary elements occupying the luminal side of the tumor and a moderately differentiated tubular region involving the shallow subserosa accompanied by abundant fibrosis. The subserosal adipose layer beneath the lesion is conically thickened.

Case 9. (a) Transabdominal ultrasound: two broad-based elevated lesions, 15 mm and 8 mm in diameter, on the gallbladder fossa side and the peritoneal side of the fundus, respectively. The former is accompanied by an unchanged outermost hyperechoic layer beneath the lesion without a deep hypoechoic area (white arrowheads) and the latter by an unchanged outermost hyperechoic layer and a deep hypoechoic area (red circle). (b) Loupe view (H&E): a carcinoma (pap), pT1a, at the fundus. (c, d) Loupe view and low power view (H&E), respectively: a carcinoma (por) at the fundus involving the shallow subserosa, accompanied by fibrosis.
As for the postoperative outcomes, four cases with the conically thickened outermost hyperechoic layer were live and one of three cases with the unchanged outermost hyperechoic layer was dead, among seven shallow pT2 cases in which more than five years had passed since the radical operation . In another respect, while the dead case tested positive for lymph node metastasis, all the live cases tested negative (Table 1).
Discussion
Ultrasound studies have demonstrated the gallbladder wall in fasting to be up to 3 mm thick and to be composed of usually two layers—an innermost hypoechoic layer and an outermost hyperechoic layer—or sometimes three layers—an innermost hyperechoic layer, a middle hypoechoic layer, and an outermost hyperechoic layer (7,8). There has been much discussion regarding the interpretation of the middle hypoechoic layer. However, the interpretation that the middle hypoechoic layer consists of not only the muscularis propria but also the subserosal fibrous layer (8) is widely accepted today. The outermost hyperechoic layer represents the subserosal adipose layer plus serosa (Table 2).
The layer structure of the gallbladder wall on ultrasound or endoscopic ultrasound (adapted from Aibe et al. (4) with modification).

Ultrasound or endoscopic ultrasound shows the gallbladder wall to be composed of two or three layers. A three-layered structure is disclosed as shown here. In case of a two-layered structure, the inner layer is hypoechoic, composed of border echo, mucosa, muscularis propria, and shallow fibrous subserosa without the innermost hyperechoic layer.
As for ultrasound diagnosis of the invasion depth of a GBC, the following consensus in interpretation has been accepted recently that gallbladder tumors with a thinned or a split outermost hyperechoic layer invade the subserosa or serosa, respectively (7) . In other words, the outermost hyperechoic layer is thinned or split by a hypoechoic mass. Today, GBCs with deep (i.e. obvious) subserosal invasion (subserosal-invasion depth > 2 mm) (2) are easily diagnosed by ultrasound or endoscopic ultrasound and many have been reported. Hence, they are not diseases that are being studied in the field of ultrasound diagnosis.
In contrast, those with neither a thinned nor a split outermost hyperechoic layer were confined to the mucosa or muscle layer (pT1 GBC) or invaded only the shallow subserosal fibrous layer adjacent to the muscle coat (subserosal fibrous layer). Thus, differentiation of these latter two types posed difficulties (9) and a gallbladder tumor with a thickness-unchanged outermost hyperechoic layer could not exclude a subserosal carcinoma confined to subserosal fibrous layer. In addition, GBCs with shallow subserosal invasion are rare and their ultrasound findings have been scarcely reported. Further, a small deep hypoechoic area has been overlooked as mentioned below. Thus, GBCs with shallow subserosal invasion are diseases that are being studied in the field of ultrasound diagnosis.
Ultrasound and pathological correlation show that a superficial hyperechoic part coincides with a papillary adenocarcinoma and a deep hypoechoic area represents an adenocarcinoma invading subserosa accompanied by abundant fibrosis and lymphocytic infiltration: the thickness of the hypoechoic area almost reflects that of subserosal fibrosis measured histologically. We consider that the limit of delineation with ultrasound of a deep hypoechoic area is 1–2mm thick (Table 1). In addition, a deep hypoechoic area also may represent a medullary lesion, hyperplastic lymph follicles, or non-cancerous fibrosis (5). For this reason, ultrasound may depict such lesions as a deep hypoechoic area in a hyperechoic benign lesion; however, such examples have not actually been reported until now. Similarly, while a polypoid GBC confined to the mucosa or muscle layer with lymphocytic infiltration or fibrosis beneath the carcinoma might be overestimated on ultrasound as invading the subserosa, this does not appear as a practical problem since the finding usually takes place simultaneously inside the area of carcinoma invasion. It is essential that a deep hypoechoic area demonstrates the subserosal invasion of a GBC even in a case without thinning of an outermost hyperechoic layer.
Although a similar expression—“a hypoechoic area in the center of the lesion”—was reported (10), the expression “a deep hypoechoic area” is more proper for the ultrasound image than the former one, because the hypoechoic area is depicted on an outermost hyperechoic layer, namely non-cancerous subserosal adipose tissue, not in the center of the lesion in three dimensions.
Kijima has reported that 87% of advanced GBCs are adenocarcinoma: well-differentiated types in the mucosa and moderately to poorly differentiated types with fibrosis in the invasive components (11). We consider, thus, that a deep hypoechoic area represents the latter components. Hence, the ultrasound finding of a deep hypoechoic area is never rare but quite ubiquitous, when GBC invades the subserosa. However, for the cases in an early phase, the significance of a small spot of the deep hypoechoic area has been overlooked until now.
In fact, we have noted that a tiny deep hypoechoic area is depicted not infrequently on the top of a conically thickened outermost hyperechoic layer as in Figure 2 of Fujita et al.’s paper (9). They did not, however, focus on this finding and overlooked it. Although Kim et al. recently reported sonography definitions of T categories, they also did not pay attention to “a deep hypoechoic area” (12). We suppose many researchers have probably not encountered an opportunity to experience case 9 (Fig. 4).
As far as the literature search with keywords of “gallbladder carcinoma,” “invasion depth,” “ultrasound,” or “endoscopic ultrasound” in PubMed since 1990, there have been no results reporting ultrasound findings on shallow pT2 GBC in detail to exhibit numeric values in subserosal invasion depth except for our papers (4,5). Further, no paper has highlighted the significance of a conically thickened outermost hyperechoic layer in terms of invasion depth of a GBC except for ours (4,5) and another one with the expression “tightened outermost hyperechoic layer” (13).
Based on the results of the ultrasound and pathological correlation of our nine cases and Kijima’s report, a hypothesis on the vertical extension of a polypoid GBC is conducted as follows: vertical extension of a protruded GBC will proceed from A through F without skipping stages (Fig. 5). As for a flat-elevated lesion, a different pathway will be considered as mentioned below.

A schema showing vertical growth of polypoid carcinoma of the gallbladder: changes in the ultrasound image and pathology. Numbers indicate the case numbers of Table 1. Light purple and rose berry areas represent shallow hyperechoic and deep hypoechoic parts, respectively. Dotted lines show the assumed deepest lines of muscle coat. In case of a protruded lesion, while a well-differentiated adenocarcinoma in the mucosa changes into moderately to poorly differentiated adenocarcinoma in the muscle coat, the lesion is drawn into the lumen. Thus, the outermost hyperechoic layer (yellow areas) is pulled up at first (B, C) as in cases 2-6. Thereafter, the layer becomes thinned as carcinoma invasion progresses with enlargement of the deep hypoechoic area (D, case 7). In contrast, in case of a flat-elevated lesion, the vertical growth is expected to go directly from A to D without going through the B and C stages. Cases 8 and 9 are considered to match this process.
The key point of the hypothesis is disclosed in “B and C”. B shows a GBC with the pulled-up outermost hyperechoic layer, and C shows a GBC with the pulled-up outermost hyperechoic layer plus a small deep hypoechoic area. Case 2 without a deep hypoechoic area corresponds to B. Then, case 6 with a deep hypoechoic area is suitable for C.
“B and C” of our hypothetical process may correspond to a state between classification groups B and C by Iri et al. (10) and between classification types B and C by Horaguchi et al. (14), if contextualized along past literature. As for the vertical extension of polypoid GBC, it is quite natural that “B and C” should come before “D” as shown in our schematic process of the tumor.
In contrast, many researchers reported that the vertical extension of a polypoid GBC went from A to F without going through stages B and C: namely A→D→E→F (Fig. 5). However, we consider that it corresponds only to an extension manner for a flat-elevated lesion.
In addition, Katayama et al. reported from a histological viewpoint that the pulled-up muscle coat was demonstrated in all five protruded pT1b GBC cases and in five of six protruded minute-pT2 GBC cases (15). The finding of “pulled-up muscle coat” is accompanied by “pulled-up subserosal adipose tissue layer,” namely, the pulled-up outermost hyperechoic layer. Hence, this finding is shown in both pT1b GBC and minute-pT2 GBC, which supports our hypothesis. Although Katayama et al. defined the subserosal invasion ≤ 0.5 cm2 as minute-pT2 GBC in two dimensions, they did not show numeric values in depth of carcinoma invasion. Therefore, it is difficult to compare their values directly with our values and catch it on ultrasound.
Although it is premature to describe a relationship between ultrasound findings and postoperative prognosis because of a small number of cases, four cases with the pulled-up outermost hyperechoic layer were negative for lymph node metastasis and alive for more than five years after the radical operation (Table 1). Therefore, we consider that gallbladder tumors with a pulled-up outermost hyperechoic layer are more likely to be negative for lymph node metastasis and provide good prognoses. However, further studies will be necessary to obtain a definitive proof through the accumulation of the additional similar cases.
In conclusion, ultrasound images of shallow T2 GBC show a deep hypoechoic area with conical thickening or unchanging of an outermost hyperechoic layer. The former demonstrates pulling up the top of the layer at first and then thinning later as the carcinoma invades with enlargement of the hypoechoic area, whereas the latter demonstrates thinning of the layer from the beginning. Polypoid gallbladder tumors with a deep hypoechoic area and a conically thickened outermost hyperechoic layer suggest shallow T2 GBC and may provide good postoperative prognoses.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.