
Abstract
Granular cell tumor (GCT) is a rare neoplasm of the soft tissues and <1% of all GCTs are malignant. Initially, GCT was considered a myogenic lesion affecting the female breast (myoblastoma). We report the case of an 83-year-old woman with a palpable lump in the left breast; mammography and ultrasound showed an irregular lesion. It was difficult to differentiate it from a malignant lesion; therefore, we performed core needle biopsy and histopathologic examination and immunohistochemical studies revealed a GCT of the breast.
Introduction
Granular cell tumors (GCT) were first alluded to by Weber in 1854 and fully described by Abrikossoff in 1926 (1,2). They can occur in any body site and may be multifocal (3), with the head/neck, chest wall and arms being the most common sites (2,4). GCTs of the breast (GCTB) account for 5–15% of all GCTs (5). It was thought to be a myogenic lesion affecting the female breast (myoblastoma) and was actually assumed to be a tumor originating from perineural or putative Schwann cells of the peripheral nerves or their precursors that grows in the lobular breast tissue, due to the immunohistochemical features. About 8% of GCTs occur in the breast (6). They are more common in middle-aged premenopausal women and especially African American women (7). They occur more frequently in the upper inner quadrant of the breast, in contrast to breast carcinoma, which is more usually located in the upper outer quadrant (4). This reflects the course of the supraclavicular nerve, which innervates the breast skin (3). We describe a new case of soft-tissue GCT in an 83-year-old woman, with a brief review of the literature.
Case report
An 83-year-old woman with a history of resection of uterine myoma presented to the primary care center with a non-painful palpable lump in the left breast and no other accompanying symptoms. At physical examination, a palpable lump was found in the superior medial quadrant of the left breast. No skin abnormalities were noted. Right breast examination results were normal. There was no axillary or cervical lymphadenopathy. Cardiovascular and pulmonary examination findings were unremarkable. No previously obtained mammograms were available for comparison. The patient underwent mammography and breast ultrasonography (US) for evaluation.
Mediolateral LO and craniocaudal mammogram (Fig. 1) of the left breast shows an irregular with slightly lobulated mass and irregular margin in the superior medial quadrant. There is no calcification in the mass and in the surrounding mass. Radiologists evaluated the mass as Category 4A in the Breast Imaging Reporting and Data System (BI-RADS). Ultrasound (Fig. 2) shows an irregular hypoechoic nodule with dense posterior acoustic shadowing. There is no increase of the vascularity of the tumor. Radiologists evaluated the mass as Category 4A in BI-RADS. Core needle biopsy (CNB) was performed and diagnosed with GCT. Magnetic resonance imaging (MRI) was not performed because granular cell tumor was suspected by CNB.

(a) Mediolateral oblique and (b) craniocaudal mammograms obtained at initial presentation show a slightly lobulated mass and irregular margin in the superior medial quadrant.

(a) Ultrasound shows an irregular hypoechoic nodule with dense posterior acoustic shadowing. (b) There is no increase of the vascularity of the tumor.
Surgical excision revealed a 0.9 × 1.0 × 0.7 cm tumor, tan solid mass with a good plane for dissection from the surrounding parenchyma. Preoperative marking was performed by ultrasound. Skin incision was done just above the mass and a lumpectomy was performed. The surrounding breast and fat tissue were mobilized and skin flap formation was carried out. After the surgeon checked the hemostasis, the surgery was completed. The patient has had an uneventful course after hospital discharge without recurrence for >2 years.
A cross-sectioned gross specimen and loupe image (Fig. 3) showed a lobulated margin with focal spiculated mass. The tumor consists of groups of cells with abundant granular, pale pink cytoplasm, and inconspicuous cytoplasmic borders. Histologically, the spiculated margin revealed collagen fiber that results in atrophy of the mammary gland. High-power photomicrograph (original magnification, ×100; hematoxylin and eosin [H&E] stain; Fig. 4a) shows infiltrating nests and cords of large polygonal cells, separated by prominent fibrous septa. High-power photomicrograph (original magnification, ×400; H&E stain; Fig. 4b) depicts abundant granular eosinophilic cytoplasm and small nuclei within the cells, features indicative of GCT. Immunohistochemical examination (Fig. 4c) showed the typical receptors of this tumor. In our case, GCT showed positive immunoreaction to PAS, PAS diastase and S-100, and calretinin and negative immunoreactivity against cytokeratin, estrogen, progesterone receptors, and also to HER2/Neu receptors. In addition, negative receptors for cytokeratin confirmed the diagnosis of GCT.

Photographs of the cross-sectioned gross specimen show irregular margin with a focal spiculated and heterogenous white mass. Loupe image also shows a spiculated mass. The spiculated margin revealed collagen fiber that results in atrophy of the mammary gland (arrow). Scale is in cm.
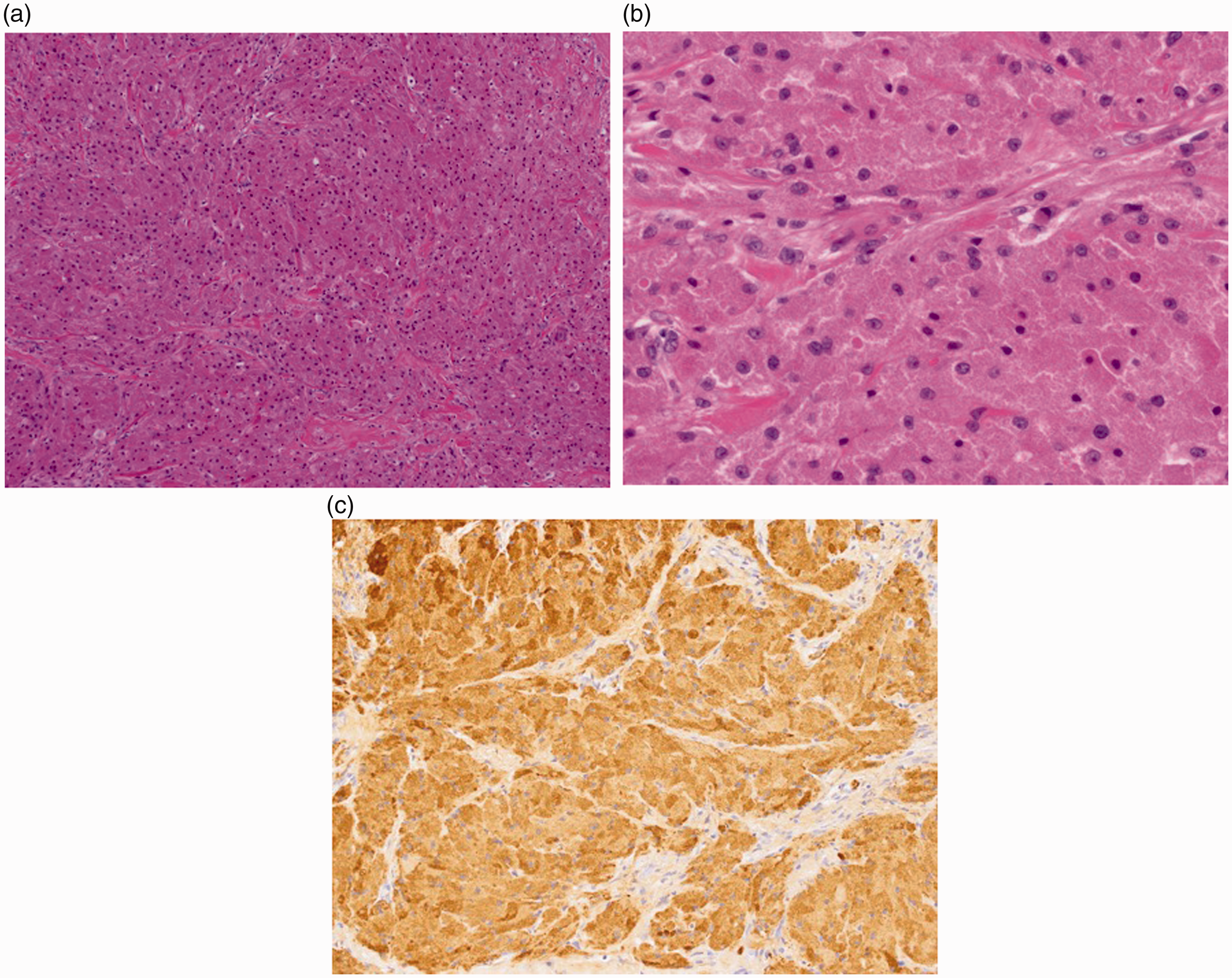
(a) High-power photomicrograph (original magnification, ×100; H&E stain) shows infiltrating nests and cords of large polygonal cells, separated by prominent fibrous septa. (b) High-power photomicrograph (original magnification, ×400; H&E stain) depicts abundant granular eosinophilic cytoplasm and small nuclei within the cells, features indicative of GCT. (c) Immunohistochemistry shows diffuse reactivity for S100 protein. Nuclei are small and bland.
Discussion
GCTB are usually asymptomatic and present as smooth, slow-growing, solitary nodules in subcutaneous, intradermal, or submucosal regions. While the majority of GCTB behave in a benign manner, malignant cases have been described (8). Malignant GCTs are rare; however, they must be suspected when pathologically enlarged lymph nodes are detected, the tumor is >5 cm, there is heterogenous signal intensity or rim enhancement on MRI, or there is infiltration of the adjacent tissues (9). Although rare they are of particular significance as they mimic scirrhous breast malignancies and are hard to distinguish from them via clinical, radiological, or observational techniques. Misdiagnosis of malignancy can lead to inappropriate radical treatment resulting in unnecessary physical and psychological hardship. A GCT usually presents as a firm and painless mass and the mass is usually well circumscribed, but several cases with poly-circumscribed masses have been reported in the literature (10). The prognosis for benign GCTB is excellent. Recurrence occurs in 2–8% of individuals after excision with wide margins (11). Further recurrence is likely to be related to non-radical excision in the first instance.
Sonographically, the common features of GCTs are solid, heterogenous, poorly defined masses with high depth/width ratio. They may show a hypervascular echotexture particularly peripherally although this is not consistent. They are generally hypoechoic and display posterior shadowing with a course internal echo and high boundary echo. Mammographically, GCTs include irregularity, spiculation, stellation, isodensity sometimes associated with hypodense rims, heterogenicity, variable circumscription, and association with tendril like extention/desmoplasia. It is important to differentiate between GCTs and breast carcinoma because although they have similarities in the diagnosis, the treatment approach and prognosis are very different. Although MRI was not performed in this case, on T2-weighted sequences GCTs show a signal intensity either equal to or slightly higher than adjacent glandular tissue. On T1-weighted sequences, they show a low signal intensity compared with adjacent glandular tissue. On contrast-enhanced MRI, this tumor enhanced significantly and fast, especially at the margins. MRI features are not specific for this tumor and suggested the possibility of malignancy. Furthermore, GCTB does not show increased glucose metabolism on FDG-PET; therefore, FDG-PET can correctly differentiate GCTB from a malignant tumor (12).
In this case, the findings of mammography and sonography were indicative of a malignant tumor; therefore, the tumor had to be excised to establish an accurate diagnosis and determine surgical excision. In our histopathologic study, the tumor showed a focal spiculated margin because of collagen fiber. Accordingly, ultrasound and mammography showed an irregular margin, and it is difficult to distinguish it from a malignant lesion. GCTB was suspected by CNB, thus surgical local excision was performed. This patient received a benign final diagnosis and obtained a successful outcome.
In conclusion, although GCTs are usually benign and slow-growing, it is difficult to distinguish them from malignant lesions. Therefore, it is very important that radiologists should be aware of their clinical, radiological, and histopathological features.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.