
Abstract
Background
Gastrointestinal symptoms and changes in colonic transit time (CTT) are common in the population.
Purpose
To evaluate consecutive patients who had been examined for CTT, along with completion of a diary about laxative and drug use, lifestyle factors, and gastrointestinal symptoms, to identify possible associations with longer or prolonged CTT.
Material and Methods
A total of 610 consecutive patients had undergone the radiopaque marker method with an abdominal X-ray for clinical purposes. The patients had completed a diary regarding medical treatment, lifestyle factors, stool habits, and their perceived constipation and abdominal pain during the examination period. The associations between CTT and laxative use, lifestyle factors, stool habits, and symptoms were calculated by logistic regression.
Results
Women had longer CTT (2.5 [1.6–3.9] vs. 1.7 [1.1–3.0] days, P < 0.001), lower weekly stool frequency (6 [3–10] vs. 8 [5–12], P = 0.001), and perceived more constipation (P = 0.025) and abdominal pain (P = 0.001) than men. High coffee consumption (P = 0.045), bulk-forming (P = 0.007) and osmotic (P = 0.001) laxatives, and lower stool frequency, shaped stool, and perceived constipation (P for trend < 0.001) were associated with longer CTT. In total, 382 patients (63%) were treated with drugs affecting motility. In the 228 patients without drug treatment, longer CTT was associated with female sex and smoking, and lower frequency of symptoms and prolonged CTT were observed compared to patients using drugs. Tea, alcohol, and abdominal pain did not associate with CTT.
Conclusions
Female sex, coffee, smoking, drug use, infrequent stools, shaped stool, and perception of constipation are associated with longer or prolonged CTT.
Keywords
Introduction
Functional gastrointestinal disorders (FGID)—e.g. irritable bowel syndrome (IBS)—are characterized by abdominal pain and dysmotility, without obvious structural changes (1). Inflammatory bowel disease (IBD) may exhibit abdominal pain and dysmotility in the absence of clinical overt inflammatory relapse of the disease (2). Apart from primary gastrointestinal (GI) diseases, patients with diabetes mellitus, multiple sclerosis, and Parkinson’s disease may also suffer from GI symptoms and dysmotility (3–5).
Colonic transit time (CTT), also called GI transit time, oroanal transit time (OATT), or whole gut transit time (
There is no “gold standard” of examining GI motility although a host of new promising methods are emerging, utilizing techniques such as magnetic resonance imaging (MRI), high-resolution manometry, and three-dimensional (3D) Transit system (8). A plain abdominal X-ray together with ingestion of radiopaque markers (ROM) is one method widely used in both clinical and research settings, to calculate the CTT, depending on how many markers that remain in the colon (6,7). No review is available to reflect or evaluate the results of the ROM method and its utilization in the clinical setting.
Our hypotheses were that lifestyle factors affect CTT and that longer CTT may affect or induce GI symptoms. To address these two hypotheses, we summarized the results from consecutive patients who had been examined by the ROM method to assess CTT and had completed a daily questionnaire during the study period about drug treatment; coffee, tea, smoking, and alcohol habits; and symptoms of constipation and abdominal pain. The primary aim of this study was to identify possible factors and symptoms which associated with longer or prolonged CTT. The secondary aim was to compile all ROM examinations to evaluate the information given.
Material and Methods
Patients
The participants consisted of 638 consecutive patients who had been examined by the ROM method over 17 years at the Department of Imaging and Function. All patients had received a clinical referral for examination of CTT and were handled according to the same clinical routines, independent of disease. Twenty-seven participants were excluded due to missing information of CTT and one was excluded due to being five years old, leaving 610 participants in the final study cohort.
This retrospective study was approved by the regional ethics committee of Lund/Malmö (2017/151, date of approval 20170314) and performed in accordance with the declaration of Helsinki. All participants were given the opportunity to withdraw inclusion via Lund University Population Research Platform webpage (9).
Measurement of colonic transit time
Ten radiopaque rings were ingested at the same time every morning for six days. On the sixth day, 20 radiopaque rods were ingested in addition. On the seventh day, a plain abdominal X-ray in anteroposterior or posteroanterior projection was obtained that covered the whole abdomen. To calculate CTT, the number of radiopaque rings remaining in the intestine were counted and divided by 10 (10). The definition of a pathologically prolonged CTT was set to > 2.2 days in men and > 4.2 days in women, according to established criteria (6,7). All participants were instructed to refrain from using any laxatives during the days under surveillance.
Study questionnaire
Each participant was instructed to complete a questionnaire each day regarding their daily consumption of coffee, tea, alcohol, cigarettes, laxatives, and other medications during the examination period. Type of alcoholic beverages was noted. The questionnaire included questions about number of stools, stool consistency, and perceived constipation and abdominal pain on a scale in the range of 0–3.
Data categorization
Continuous variables were not normally distributed, why all data were categorized. Values of CTT were divided into quartiles. Patient age was divided into five age groups: <30, 30–39, 40–49, 50–59 and ≥60 years. Coffee and tea intake was reported in number of cups each day; the total numbers of cups were then summarized for the six-day period. Likewise, alcohol intake was reported in number of standard drinks each day and was then summarized for the six-day period. Henceforth, the six-day period will be referred to as a week for simplicity. Coffee (cups/week), tea (cups/week), and alcohol (standard drinks/week) intakes were grouped into tertiles, because of uneven groups when using quartile grouping. Smoking was categorized as smoker or non-smoker.
Stool consistency was assigned to one of three groups: watery stool; shaped stool; or mixed stool, which means the appearance of both watery and shaped stool on the same day. Both abdominal pain and constipation were rated on a scale of 0–3 for each day; 0 being “no abdominal pain” or “no constipation,” respectively, and 3 being “severe pain” or “severe constipation,” respectively. The individual days were then summarized to a total number in the range of 0–18. Laxatives were divided into four categories based on their main mode of action: bulk-forming agents; osmotic agents; stool softener agents; and stimulant agents. If a patient used laxatives from more than one category, the patient was assigned to the laxative considered most potent, according to the following grading based on the standard therapy progression (11): stimulant agents > stool softener agents > osmotic agents > bulk-forming agents.
Data analysis
IBM SPSS statistics version 24.0 (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses.
Differences between men and women and between patients with or without medical treatment were assessed using Mann–Whitney U test for ordinal values and Fisher’s exact test for nominal values. CTT values were split by the median value to longer and shorter CTT. Factors intended to study for influence on CTT (independent variables), namely, gender, age, smoking, amount of coffee, tea and alcohol intake, type of alcohol intake, and type of laxatives were examined using an unconditional logistic regression to calculate crude odds ratio (OR) and 95% confidence interval (CI). Analyses were then performed adjusted for all variables. A second grouping was made based on pathological and normal CTT (>2.2 days for men and > 4.2 days for women) (6,7). After unconditional logistic regression to calculate crude OR and 95% CI, analyses were adjusted for all variables statistically significant in the unconditional calculation. To study the associations between CTT and GI symptoms (dependent variables), the number of stools and perception of constipation and abdominal pain were divided by the median value into two groups, and unconditional logistic regression to calculate crude OR and 95% CI were performed, followed by adjustment for gender, coffee intake, and laxative use, since these factors were associated with longer CTT and thus considered potential confounders. Stool consistency was divided into watery and shaped stool, excluding participants with mixed stool consistency, and calculated in the same way as stool frequency and GI symptoms. A subgroup analysis was performed according to the abovementioned description, with only inclusion of the 228 patients without any medication. The association between CTT and GI symptoms were adjusted for sex and smoking, since these factors associated with longer CTT in the subgroup. Furthermore, an interaction analysis was performed between sex and each factor in the adjusted models by including an interaction term. The adjusted analyses were performed as a complete case-analysis. A P value <0.05 was considered statistically significant.
Results
Patient characteristics
The final sample consisted of 610 patients, 129 (21%) men and 481 (79%) women. No statistically significant differences in age, smoking prevalence, or in the consumption of cigarettes, coffee, tea, alcohol, or laxatives were found between men and women. Men drank more beer and women drank more wine (Table 1). When comparing CTT, men showed a faster transit time of 1.7 days (interquartile range = 1.1–3.0 days) compared to women with 2.5 days (interquartile range = 1.6–3.9 days) (P<0.001). In accordance with this, the number of stools per week was found to be higher for men than for women (P = 0.001), but with no differences in stool form between sexes. Both abdominal pain (P = 0.001) and constipation (P = 0.025) were found to be rated lower in men than in women (Table 1).
Patient characteristics.

Values are presented as median (interquartile range [IQR]) or n (%). Statistical calculations were performed using the Mann–Whitney U test for ordinal values and Fisher’s exact test for nominal values.
P<0.05 is considered statistically significant.
*Rated on a scale of 0–3 for each day and summarized to a total number ranging from 0–18.
CTT, colonic transit time.
Except laxative use, the most common self-reported medications were analgesic drugs in the form of paracetamol or non-steroidal anti-inflammatory drugs (NSAIDs) (n = 61, 10%), proton pump inhibitors or histamine antagonists (n = 60, 10%), antidepressant drugs (n = 41, 7%), sedatives and/or sleeping pills (n = 37, 6%), beta blockers (n = 27, 4%), other hypertensive drugs (n = 20, 3%), motility-stimulating drugs (n = 20, 3%), opioid or opioid-like drugs (n = 22, 3%), and antispasmodic drugs (n = 17, 3%). Altogether, 317 patients (52%) used any of these drugs during the week. Only 228 out of 610 patients (37%) were without treatment of both laxatives and other motility-modulating medications during the examination period.
Laxatives and lifestyle factors in association with colonic transit time
Longer CTT was associated with female sex, higher coffee consumption and intake of bulk-forming and osmotic laxatives, and tended to be associated with smoking (Table 2). No sex interactions were found in laxative use or lifestyle factors (data not shown). In men, prolonged CTT was associated with high coffee consumption (P = 0.01) and use of bulk-forming laxatives (P = 0.007), with a tendency of association in the age range of 30–49 years compared to age <30 years (Table 3). In women, prolonged CTT did not associate with any lifestyle factor, but was associated with use of osmotic (P = 0.005) and stimulant laxatives (P = 0.019) (Table 3).
Associations of shorter and longer colonic transit time.

Colonic transit time was divided into shorter and longer transit time by the median values. Values are presented as crude odds ratio (OR) and 95% confidence interval (CI). Adjusted ORs are adjusted for all variables.
P < 0.05 is considered statistically significant.
Std, standard drinks.
Associations with pathologic colonic transit time in men and women.
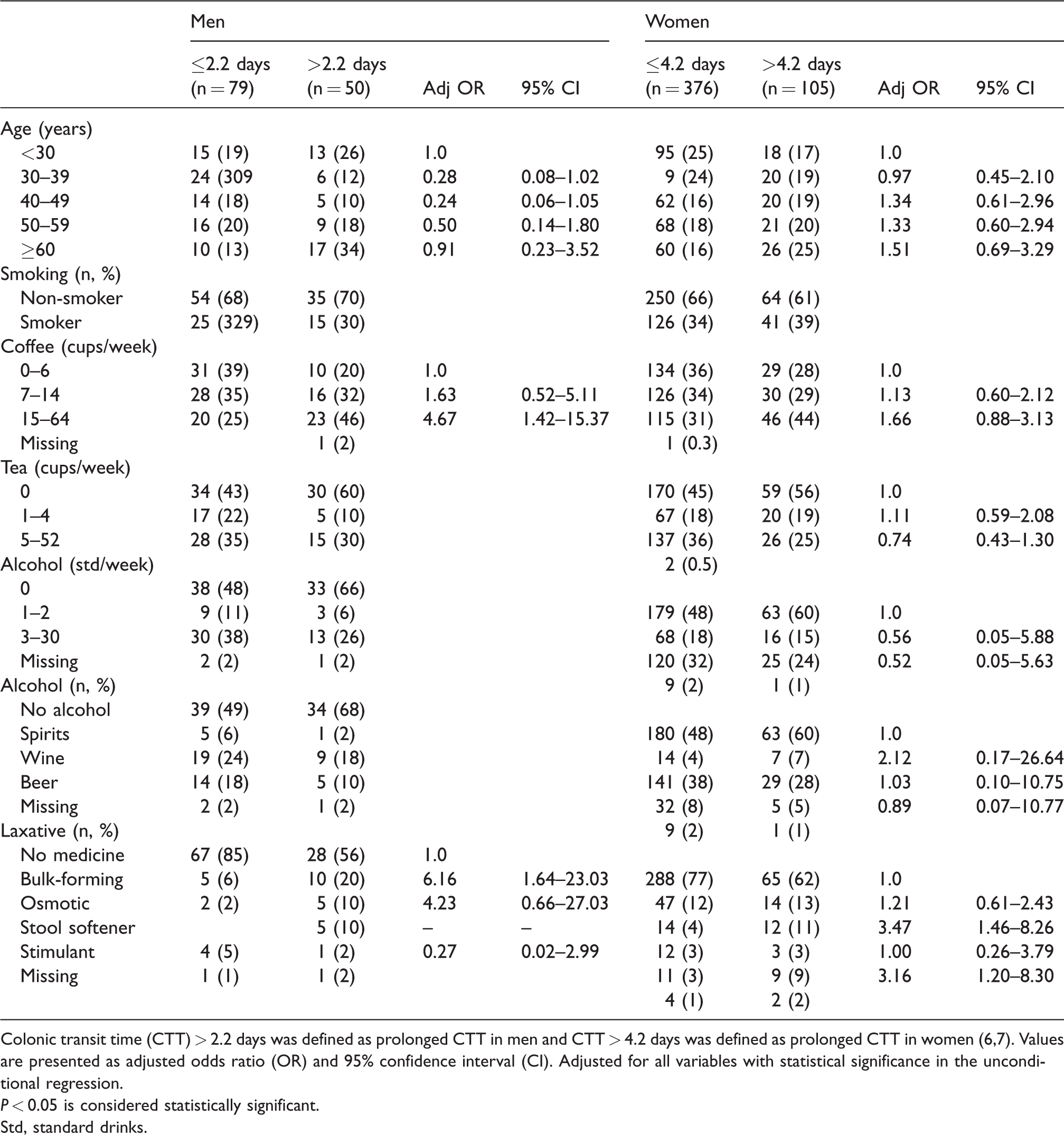
Colonic transit time (CTT) > 2.2 days was defined as prolonged CTT in men and CTT > 4.2 days was defined as prolonged CTT in women (6,7). Values are presented as adjusted odds ratio (OR) and 95% confidence interval (CI). Adjusted for all variables with statistical significance in the unconditional regression.
P < 0.05 is considered statistically significant.
Std, standard drinks.
Gastrointestinal symptoms in association with colonic transit time
A more frequent stool passing (median value ≤6) was inversely associated with CTT [OR] = 0.08; 95% [CI] = 0.04–0.14, highest vs. lowest quartile, P for trend <0.001). In analogy, shaped stool (OR = 6.75; 95% CI= 2.42–18.84, highest vs. lowest quartile, P for trend <0.001) and aggravated perception (median value ≤2) of constipation (OR = 5.44; 95% CI = 3.15–9.39, highest vs. lowest quartile, P for trend <0.001) were associated with longer CTT. The abdominal pain did not associate with CTT (data not shown). No sex interactions were found in the associations between CTT and GI symptoms (data not shown).
Associations in patients with or without any drug treatment
When excluding all patients with any ongoing medication that could affect gut motility, female sex (OR = 3.90; 95% CI = 1.96–7.75; P<0.001) and smoking (OR = 1.98; 95% CI = 1.02–3.84; P = 0.04) were associated with longer CTT, whereas coffee intake did not associate with CTT (OR = 1.75; 95% CI = 0.78–3.94; highest vs. lowest tertiles, P = 0.18). More infrequent stool passing, shaped stool form, and perceived constipation were associated with longer CTT, whereas abdominal pain did not associate with CTT (Table 4). Patients without ongoing medication had less perception of constipation (0 [0–7] vs. (4 [0–10], P <0.001), abdominal pain (4 [0–9] vs. 6 [2–10], P = 0.001), and shorter CTT (2.1 [1.4–3.0] days vs. 2.5 [1.5–4.1] days, P <0.001), with a tendency to higher stool frequency (6.5 [5–10] vs. 6 [3–10], P = 0.08), compared to patients with any ongoing medication. Furthermore, prolonged CTT was less common in both men (29% vs. 49%, P = 0.04) and women (14% vs. 26%, P = 0.01) without any medication, compared to patients with motility-affecting medication.
Associations between symptoms and colonic transit time.
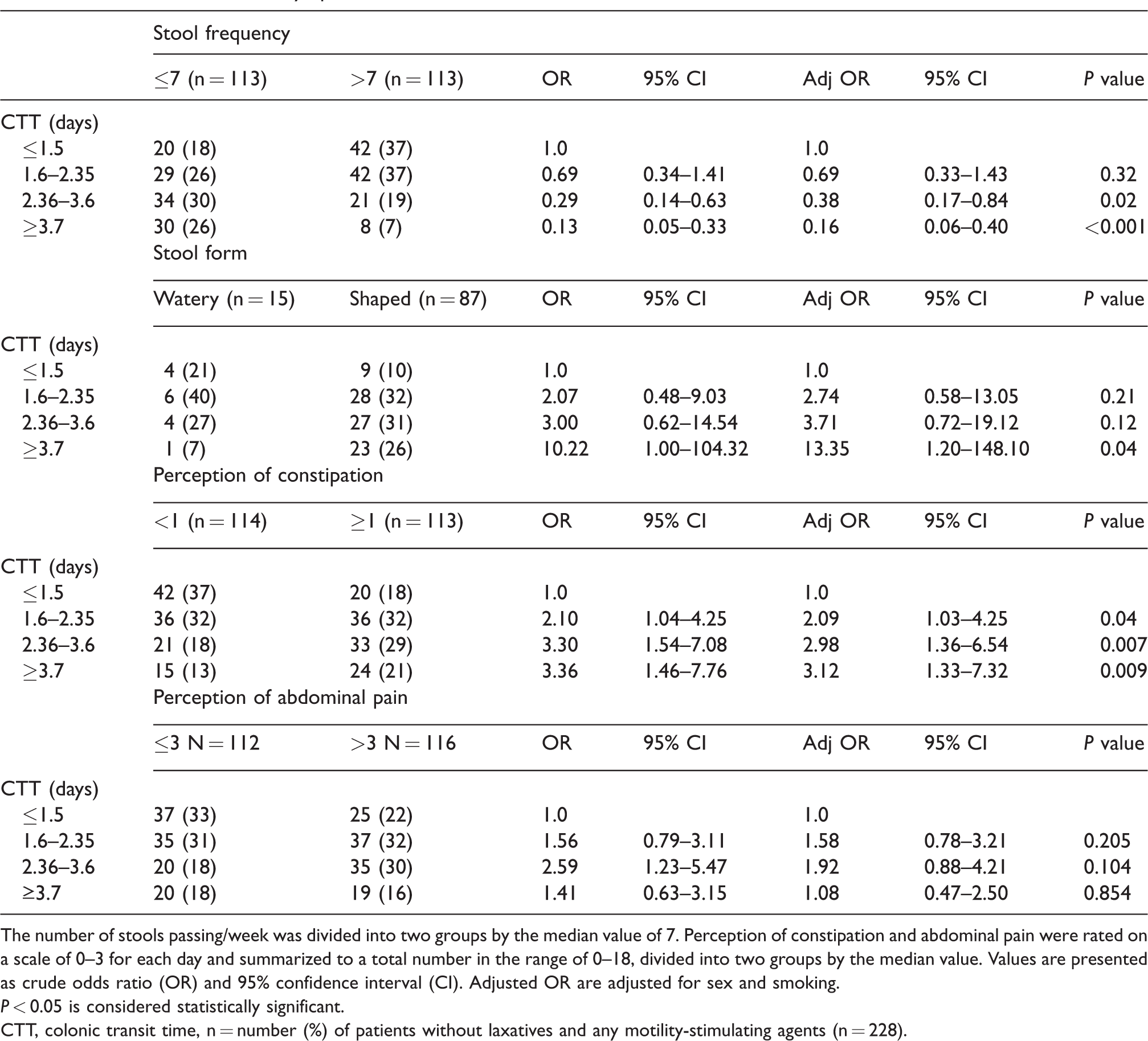
The number of stools passing/week was divided into two groups by the median value of 7. Perception of constipation and abdominal pain were rated on a scale of 0–3 for each day and summarized to a total number in the range of 0–18, divided into two groups by the median value. Values are presented as crude odds ratio (OR) and 95% confidence interval (CI). Adjusted OR are adjusted for sex and smoking.
P < 0.05 is considered statistically significant.
CTT, colonic transit time, n = number (%) of patients without laxatives and any motility-stimulating agents (n = 228).
Discussion
The main findings in the present study were that female sex, high coffee consumption, use of bulk-forming and osmotic laxatives, low stool frequency, shaped stool, and perception of constipation were associated with longer CTT. High coffee consumption and use of bulk-forming laxatives were associated with prolonged CTT in men; use of osmotic and stimulant laxatives were associated with prolonged CTT in women. Patients who did not use motility-affecting drugs had shorter CTT, lower prevalence of prolonged CTT, and fewer GI symptoms than patients without such drugs.
The unexpected absence of association between CTT and age in the present study may depend on few included older individuals (>60 years) (12). In accordance with previous studies (6,7), women were found to have almost 50% longer CTT with 2.5 days versus 1.7 days for men; shaped stool form was positively associated with higher CTT and stool frequency was negatively associated with CTT. Furthermore, women´s weekly summarized abdominal pain was rated twice as high and their summarized perception of constipation was rated six times higher, compared to men. Abdominal pain may be explained by side effects from medical treatment or presence of organic diseases, not identified with the ROM method, as it was unrelated to CTT. Peripheral or visceral hypersensitivity may be another explanation for abdominal pain (1,13–16). Differences in GI symptoms between sexes have been hypothesized to depend on involvement of ovarian hormones (17).
The current results suggest that constipation should be treated with laxatives and abdominal pain with pain-modulating agents, provided there was an absence of any organic GI disease demanding specific treatment. In addition, slow transit constipation and outlet obstruction are successfully treated with laxatives in many cases (12). From a clinical point of view, a transit time examination may be of limited importance for the treatment strategy. From a scientific point of view, it may be important to classify normal or delayed transit time and explore molecular mechanisms, to identify subgroups of patients with or without organic signs of gut dysmotility. However, an examination during influence of laxatives and other motility-affecting drugs may give unreliable information.
All patients were instructed to refrain from laxatives during the study period. Still, around 25% of the patients used different types of laxatives. Bulk-forming, osmotic, and stimulant laxatives were associated with prolonged transit time, although an improvement of transit time has been documented by these agents (18,19). The explanation to the associations may probably be that patients with longest transit times were in greatest need to be relieved of their symptoms.
The effect of coffee on GI transit time is insufficiently described. A recent study could not find any effect of coffee on gastric or small intestinal transit time (20), but older studies have shown that coffee stimulates colonic motility in healthy volunteers (21,22). Albeit no scientific evidence, there is a widespread conception in the general population that coffee induces defecation. In line with the higher consumption of certain laxatives among patients with the longer transit times, it is possible that the same patients tried to relieve their symptoms by extensive coffee consumption. In patients without any drug treatment, no association between coffee consumption and transit time was observed.
Alcohol intake did not show any overt effect on CTT, as described previously (23–25). The literature shows the minor importance of smoking and alcohol on functional bowel symptoms (26). In contrast, increased physical activity and dietary modification, which were not considered in the present study questionnaire, have been shown to be useful therapeutic tools in improvement of GI symptoms and colonic motility (27–30). The present results support the assumption that a pathologically prolonged CTT is caused by myopathic and/or neurologic abnormalities, refractory to several lifestyle interventions (12).
Many of the patients used drugs which may exert motility-reducing properties, such as opioids, beta blockers, antihypertensive drugs, and antidepressant medication, that could hypothetically explain the higher prevalence of prolonged CTT in the medication group. The need of this medical treatment should be re-evaluated considering their impact on GI transit time and symptoms, and the classification of normal or prolonged transit time may be misleading during this type of drug treatment.
The strength of the present study is the large cohort of consecutively examined individuals, along with completion of questionnaires concerning medication, lifestyle habits, and GI symptoms. However, there are several limitations in the study. The self-reporting questionnaire allows the participant to under- or overestimate their consumption or symptoms. Diet and fluid intake as well as the grade of physical activity were not considered. The phase of the menstrual cycle was unknown. Moreover, we did not know the diagnoses of the patients referred for CTT. Since the majority of patients who seek help for constipation and abdominal pain are diagnosed as FGID, one can speculate that the majority of the examined participants suffered from this disorder, but the possibility exists that patients with diseases such as diabetes mellitus and neurologic disorders were included (12). Since the answer from the examinations were given in number of markers, without any description of the markers situated, regional transit time could not be estimated. Thus, from the reply given to the clinician, it was impossible to differ between colonic inertia and outlet obstruction in the cases of prolonged CTT. A shorter examination period could be preferred to make it easier for the patients to refrain from drug treatments during the procedure (31). We could not assess short CTT, since the number of remaining rods were not given in several replies from the X-ray examination, and no questions about diarrhea were present in the diary.
In conclusion, the link between CTT and the aforementioned lifestyle factors is complex. Infrequent stool passing and perception of constipation may indicate prolonged transit time. Transit time examination may be redundant to handle patients with mainly symptoms of abdominal pain. GI symptoms may be secondary side effects to several drugs, which should be considered when actual, and drugs should be withdrawn before examination of CTT.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed by grants from the Development Foundation of Region Skane.