
Abstract
Background
Laterality errors in radiology reports can lead to serious errors in management.
Purpose
To reduce errors related to side discrepancies in radiology reports from thoracic imaging by 50% over a six-month period with education and voice recognition software tools.
Material and Methods
All radiology reports at the Thoracic Imaging Division from the fourth quarter of 2016 were reviewed manually for presence of side discrepancies (baseline data). Side discrepancies were defined as a lack of consistency in side labeling of any abnormality in the “Findings” to “Impression” sections of the reports. Process map and Ishikawa fishbone diagram (Microsoft Visio) were created. All thoracic radiologists were educated on side-related errors in radiology reports for plan–design–study–act cycle 1 (PDSA #1). Two weeks later, voice recognition software was configured to capitalize sides (RIGHT and LEFT) in the reports during dictated (PDSA# 2). Radiology reports were analyzed to determine side-discrepancy errors following each PDSA cycle (post-interventional data). Statistical run charts were created using QI Macros statistical software.
Results
Baseline data revealed 33 side-discrepancy errors in 47,876 reports with an average of 2.5 errors per week (range = 1–8 errors). Following PDSA #1, there were seven errors pertaining to side discrepancies over a two-week period. Errors declined following implementation of PDSA #2 to meet the target of 0.85 side-discrepancy error per week over seven weeks.
Conclusion
Automated processes (such as capitalization of sides) help reduce left/right errors substantially without affecting reporting turnaround time.
Introduction
Medical errors rank behind coronary artery diseases and cancer as the third leading cause of deaths in the United States (1). Medical error refers to: failure of a planned action to be completed as intended; use of a wrong plan to achieve an aim; an unintended act or one that does not achieve its intended outcome; and deviation from the process of care, which may or may not cause harm to the patient (2–4).
Prior studies have reported the prevalence of errors related to laterality or left and right discrepancies in radiology and non-radiology specialties (5–8). While surgical and procedural errors related to wrong side treatment are rare, side discrepancies in radiology reports can contribute to these errors leading to catastrophic consequences for both physicians and patients (5,7,9–12). We defined laterality errors related to side discrepancies as lack of consistent side labeling of an abnormality between the “Findings” and “Impression” sections of the radiology reports.
The clinical process improvement strategies stresses on the development of SMART objectives involving components that are Specific (confined to thoracic imaging), Measurable (50% reduction in frequency of side discrepancies in radiology reports), Achievable (with education and software-based changes), Relevant (in line with the hospital’s policy of error reduction and quality improvement), and Timebound (timeframe of the baseline and post-intervention data of six months) (13). Thus, the aim of our clinical process improvement study was to reduce errors related to side discrepancies in radiology reports from thoracic imaging by 50% over a six-month duration with education and voice recognition software changes.
Materials and Methods
This quality improvement study was exempted from the need of approval from the human research committee of the institutional review board. None of the authors have any pertinent financial disclosure in relation to this study.
Baseline data
Radiology information system (RIS) support staff were requested to export all consecutive radiology reports from 12 October 2016 to 11 January 2017 on imaging examinations dictated in the division of thoracic imaging. Exported data included information related to examination number, modality name (radiography, computed tomography [CT], or magnetic resonance [MR]), protocol name (where applicable for CT and MR), date and time of examination, study indication, radiologist’s name, and the entire “Findings” and “Impression” sections of radiology reports. Data were exported to Microsoft Excel for analysis. All radiology reports without mention of right and/or left side were excluded. Five study coinvestigators (RV, SN, AT, AO, RC) analyzed the remaining radiology for the presence of side discrepancies in the description of radiology findings between the “Findings” and the “Impression” sections of the reports.
Process and cause analysis
Clinical process improvement involves the creation of a series of illustrations to understand the clinical process, a source of limitation or errors in the process, and identify focused areas for improvement as targets (11). The baseline dataset on radiology reports with side discrepancies between the findings and impressions sections was reviewed to determine possible causes for these errors and plot a Pareto chart using QI Macros software (KnowWare International, Inc., Denver, CO, USA). We created a process map using Microsoft Visio (Microsoft Inc., Redmond, WA, USA) to illustrate various steps from online radiology order entry for requesting imaging exam to the final sign-off radiology report. The same program was used to illustrate possible sources and causes of side discrepancies with an Ishikawa fishbone diagram.
The entire division of thoracic radiology—including attending radiologists, clinical and research fellows, and radiology residents posted in the section—were invited for a brainstorming session to discuss strategies for reducing side discrepancies in radiology reports. A priority and payoff matrix was created to classify various solutions based on their ease of implementation and possible impact on reducing side discrepancies.
The outcome measure was defined as the number of radiology reports with side discrepancies, process measure as the rate of radiology reports with side discrepancies over two-week periods, and balance measure as any increase in reporting time because of any intervention(s) designed to reduce side discrepancies.
Plan–Design–Study–Act (PDSA) implementation
The first PDSA cycle was planned around awareness and education about the side discrepancies among the division of thoracic imaging staff. During this 15-min didactic session, a study co-investigator (SD) informed the division members about baseline data on side discrepancies in the division and its implications on patient care, reporting physicians and treating physicians. To emphasize the fact, radiologists were informed that errors resulting from wrong side procedures or surgeries (whether associated with “erroneous side” description in the radiology report or not) are regarded as “never” events and require mandatory reporting to the office of the state Board of Registration in Medicine.
After two weeks, a second PDSA cycle was initiated with manual modifications in the settings of the voice recognition software (Powerscribe 360, Nuance Communications, Burlington, MA, USA) for individual reporting radiologists in the division of thoracic imaging. This involved activating the existent software feature named “capitalize RIGHT and LEFT” in the radiology report text. Once this feature was activated, each time radiologists dictated the words right or left, they appeared in the report as RIGHT or LEFT. Informal feedback was obtained from each radiologist about this feature. The second PDSA cycle was initiated after obtaining permission from the director of the Thoracic Imaging Division and consent of each thoracic radiologist.
Post-implementation data
All thoracic imaging radiology reports (2976 reports) were reviewed over a two-week period following implementation of the first PDSA cycle. Seven weeks following implementation of the second PDSA cycle, all reports emanating from the Thoracic Imaging Division (10,657 reports) were assessed for the presence of side discrepancies in the radiology reports. In total, 13,633 radiology reports from the Thoracic Imaging Division over a period of nine weeks were assessed following implementation of the first PDSA cycle. For each radiology report with a side discrepancy, we recorded attributes identical to those described in the baseline data. We reviewed the medical records to assess if there were any consequences related to the errors of side discrepancy in the radiology reports.
Statistical process chart
Since side-discrepancy errors are rare and counted as discrete events over a constant period, c-chart was chosen as the template for statistical process chart for the study. The statistical process chart was created using QI macros statistical software. Fisher’s exact test was used for statistical analysis. A P value < 0.05 was considered statistically significant.
Results
Process and cause analysis
Fig. 1 illustrates the process map illustrating steps where a document with the wrong side might be created in the imaging chain from order to final interpretation and sign-off. The Ishikawa fishbone diagram summarizes potential causes for wrong side pertaining to the radiologists, environment, and imaging exam as well as PACS and voice recognition software (Fig. 2) (14). The Pareto chart summarizes causes of errors related to the wrong side of findings in the Thoracic Imaging Division (Fig. 3). Decisions regarding prioritization of interventional strategies for reducing side discrepancies in radiology reports were based on the priority/payoff matrix (Table 1).

Process map from order to final report sign-off with document generation at various steps which can show sites of laterality errors.
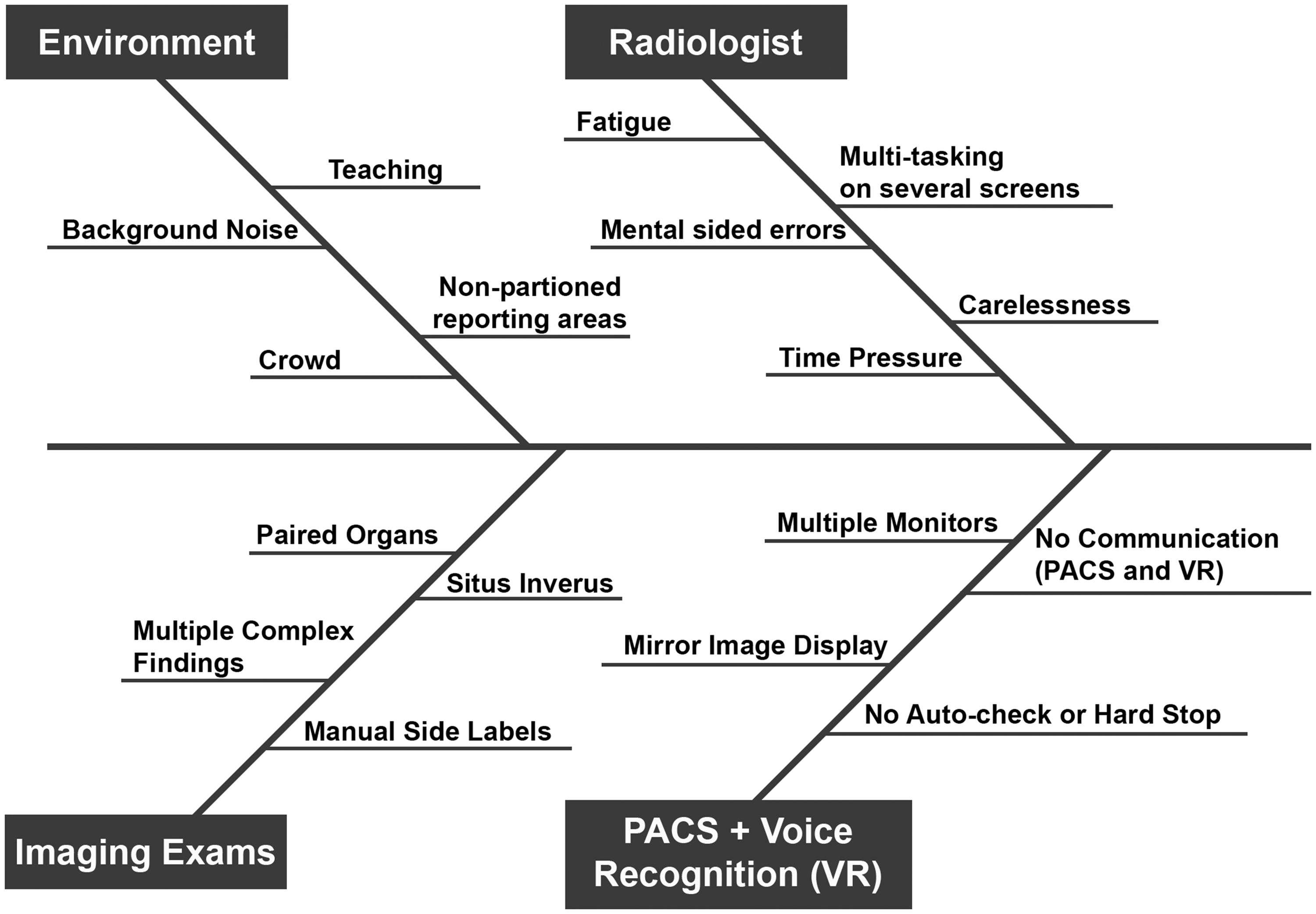
Ishikawa fishbone diagram to understand various contributory causes of side discrepancies in radiology reports.

Pareto chart depicts various causes of side errors in the radiology reports. Most errors (> 90%) were attributable to the radiologists in imaging exams with multiple bilateral findings. There were significant statistical differences between the frequency of side errors in radiology reports from the baseline data (average = 2.5 side errors/week) and following PDSA #1 (3.5 side errors/week) and #2 cycles (0.9 side errors/week) (P < 0.0001).
Priority/payoff matrix on impact of change (High/Low) and ease of implementation (Easy/Hard) to achieve desired outcome (reduce side discrepancies).

Baseline data
Of the 47,876 baseline radiology reports dictated in the division of thoracic imaging, 25,293 reports had descriptions regarding the side of the radiologic findings in the “Impression” section. In the baseline data, there were 33 reports (33/47,876, 0.0007%) with side discrepancies between the “Findings” and “Impression” sections with an average of 2.5 errors (range = 1–8) per week. The overall volume in the department was about 3683 radiology reports per week.
In the 33 radiology reports with side discrepancies, sides were described 252 times (252/33; 7.6 sides per report) with 151 mentions for the right side (151/33; 5.4 side labels per report) and 101 for the left side (101/33, 3.1 side labels per report) (P < 0.0001). Among the modalities, CT reports (25/33, 76%) had the most errors followed sequentially by plain radiography (7/33, 21%) and MR (1/33, 3%) (P < 0.0001). Most side discrepancies pertained to lung findings (24/33, 73%) with remaining from the chest wall (bony thorax, axilla, and chest wall muscles) (4/33, 12%) (P < 0.0001). Right-sided findings were mislabeled as left in 18/33 discrepancies and 15/33 left-sided findings were misquoted as right (P = 0.467). Radiologists corrected the side discrepancies with an addendum in only 5/33 reports (15%) with these errors compared to 28/33 reports with uncorrected labels (85%) (P < 0.0001). Although 21 radiologists (11 men, 10 women) read thoracic imaging studies, 20/33 side discrepancies (61%) belonged to reports from male radiologists versus 13/33 (39%) from female radiologists (P = 0.13).
PDSA cycles 1 and 2
Following the awareness and educational session (PDSA #1), a spike in the number of reports with side discrepancies was noted leading to seven reports with side discrepancies over the two-week period or 3.5 errors per week (seven discrepancies/2976 radiology reports; 0.002%).
Once PDSA #2 was implemented, the side discrepancies dropped considerably to 0.9 errors per week (six errors over the seven-week duration, 6/10,657; 0.0005%). The baseline and post-PDSA data are summarized in the statistical processing chart (c-chart) (Fig. 4). Most radiologists supported the capitalization of RIGHT and LEFT side in the radiology reports, stating that the change made them more attentive to the side and to check for the correct side before signing off their final reports. Fortunately, a review of medical records did not reveal any ill-effects of side discrepancies on patient management.

Statistical process chart illustrating baseline and post-PDSA implementation data following each cycle.
Discussion
Our study establishes the infrequent but quantifiable prevalence of wrong side errors in the radiology reports and applies systemic clinical improvement process strategies to implement mitigating interventions and to assess their impact.
The infrequent occurrence of side errors in radiology procedures and reports have been reported in prior publications (5,8,12). Likewise, CT as the dominant contributory modality towards these errors has also been observed (5). Though not unexpected, most side discrepancies occurred in complex radiology reports with multiple bilateral lesions with numerous citations of right and left sides to describe lesion distribution and location.
The success of active interventions such as software-based alterations in voice recognition programs assessed as part of the PDSA #2 cycle has also been reported previously in a study on automatic highlighting and correction of errors for radiography pertaining to discrepancies between imaged and reported sides (6). Another publication documented effectiveness of color highlighting of words right and left in the reports to help radiologist identify the sides and correct any wrong side errors (5).
Chief among implications of our study are the presence of a finite range of side discrepancies in radiology reports and success of active intervention such as upper-case right and left in radiology reports. The latter draws the attention of the radiologist to match the lesion side in both findings and impression sections of the report and makes it easier to cross check for side errors. Furthermore, based on feedback received from the radiologists, upper-case side descriptions also emphasized the need to reconcile the lesion side in the images and their reports.
The fact that sides of the lesions were mentioned at least five times in all radiology reports with side discrepancies with an average side mention rate of 7.6 per report implies that reports with discrepancies likely belonged to challenging or complex cases.
There are some limitations in our study. We did not assess actual incidence of errors related to discordance between actual lesion side in radiology images and its description in the corresponding report. Given the rarity of these errors, this would have required review of several thousand cases making it impractical and inefficient. However, this limitation implies that our study underestimated the actual incidence of side-related errors in radiology. Although we assessed the frequency of laterality errors in area of our subspecialty (thoracic imaging), such errors can affect radiology exams and reports in the extremities as well. Another limitation pertains to shorter duration of follow-up after the introduction of PDSA cycles compared to the baseline data and doesn't consider the washout effect (P = <0.0001). While helpful, given the workload in our hospital and consequent multiplication of radiology report warranting evaluation, we did not extend the PDSA cycles throughout the department. It is difficult to extrapolate if the success of our PDSA #2 would have been possible in other divisions of radiology. We also did not assess if other strategies like changing the font type or color for “right” and “left” would have been equally or more successful than their capitalization.
In conclusion, side discrepancies between the “Findings” and “Impression” sections of the radiology reports are uncommon but quantifiable. Active intervention with software automation (capitalization of sides) can help reduce side discrepancies whereas error awareness and education may be inadequate. Clinical process improvement strategies help reduce side discrepancies in a systematic and measurable manner without hampering the workflow or negatively affecting the report turnaround times.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MKK has received a research grant from Siemens Healthcare and Toshiba America Medical Systems unrelated to the work being presented in this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.