
Abstract
Aortic subvalvular pseudoaneurysms (PSA) are particularly subjected to strain and shear stress forces from blood flow and therefore their size can vary along the heart cycle. Here we describe a case of an aortic subvalvular PSA that shows significant variation in size between systolic and diastolic phase during retrospective ECG-triggered cardiac computed tomography angiography.
Introduction
Aortic subvalvular pseudoaneurysm (PSA) is a relatively rare complication which may occur after aortic valve replacement (AVR). The underlying causes for this condition may be infective endocarditis, aortic dissection, connective tissue disorders, preoperative chronic hypertension, or aortic calcification. The development of aortic subvalvular PSA mostly occurs within a few weeks to months after surgery and often presents with non-specific symptoms. As aortic PSA may enlarge over time, the risk for fatal complications increases, e.g. rupture, thrombosis, compression of coronary vascularity. The non-invasive methods for diagnosing aortic PSA are computed tomography (CT), magnetic resonance imaging (MRI), and transesophageal echocardiography (TEE) (1–5).
Case report
A 49-year-old man with a Medtronic-Hall aortic valve prosthesis (Medtronic, Minneapolis, MN, USA) presented with fever, chills, and vomiting one year after aortic valve surgery. Physical examination revealed suspicious septic emboli in the palm of the right hand and in the left little toe; blood culture showed the presence of Staphylococcus aureus. MRI revealed a retrofaryngeal phlegmon and a 10-mm supratentorial cerebral lesion which was interpreted as septic embolism. Overall, these findings raised a suspicion of prosthesis endocarditis. Follow-up echocardiography showed two paravalvular leakages. The patient underwent surgery where vegetation of the aortic valve prosthesis was discovered. The aortic valve was replaced by a 25-mm St. Judes mechanic aortic valve prosthesis (Abbot, Saint Paul, MN, USA). During surgery, a minimal fistula was detected in the aortic root.
Retrospective ECG synchronized cardiac computed tomography angiography (CTA) was performed using the dual source multidetector (MDCT) Somatom Definition Flash® (Siemens Healthcare, Forchheim, Germany). Scan parameters included 128 × 0.6 mm detector collimation, 100 kVp, and 370 quality reference mAs. An individualized intravenous contrast media (CM) dosage of 300 mg iodine per kilo body weight of 80 mL iodixanol 320 mg per mL (Visipaque®, GE healthcare) was injected at 6.5 mL/s followed by a 35-mL physiological saline (NaCl) flush at the same injection rate. The optimal scanning window was defined by using a test bolus injection protocol containing 15 mL of CM and 35 mL of NaCl. Time to peak enhancement of ascending aorta was calculated by using a 10-mm circular region of interest (ROI).
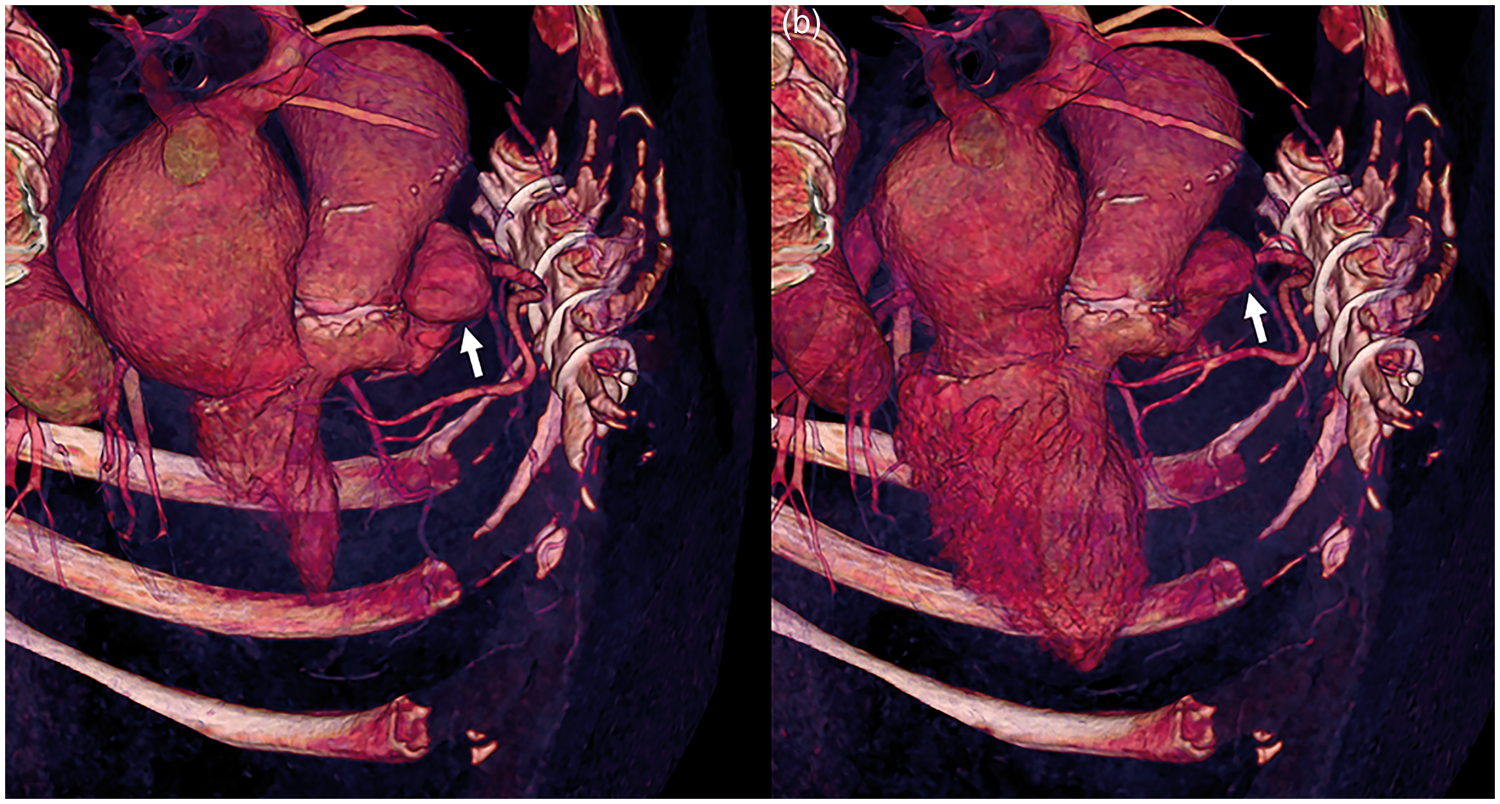
Cardiac CTA demonstrated a mechanic aortic valve prosthesis with normal opening angle and three subvalvular PSA. The largest PSA was located below the right coronary cusp and could be seen to vary in size between systole 41 × 42 × 34 mm and diastole 39 × 34 × 27 mm (Figs. 1 and 2, video).
A-D. ECG synchronized cardiac CTA of the aortic subvalvular pseudoaneurysm located below the right coronary cusp which varies in size between systole (arrow in Fig. 1A and C) and diastole (arrow in Fig. 1B and D).
Discussion
CTA imaging of PSA associated with the aortic root can be challenging especially in combination with the patient having a high heart rate which often involves the presence of movement artifacts. Therefore, in order to minimize the risk of misinterpretations of PSA size, CTA examination should be performed ECG-synchronized. This is illustrated in Fig. 3, where the first CTA examination of the patient was carried out non-ECG-synchronized (Fig. 3a) compared with ECG-synchronized cardiac CTA (Fig. 3b).
A-B. None ECG synchronized CTA (A) compared to ECG synchronized cardiac CTA (B).
When performing cardiac CTA, a stable and low heart rate is of great importance to ensure optimal image quality. Therefore, in order to reduce the heart rate, beta-blockers are often used at cardiac CTA, allowing scanning during the mid-diastolic phase which reduces the risk of deterioration of image quality due to motion artifacts (6,7). However, our case illustrates how the size of PSA varies with cardiac phase. To avoid misinterpretation of their severity, PSA originating from the aortic subvalvular region or from the aortic root should be imaged in both diastolic and systolic phases by performing an ECG-synchronized cardiac CTA.
Supplemental Material
sj-vid-1-arr-10.1177 2058460118778068 -Supplemental material for Variable size of aortic subvalvular pseudoaneurysm
Supplemental material, sj-vid-1-arr-10.1177 2058460118778068 for Variable size of aortic subvalvular pseudoaneurysm by Anders Svensson, Kerstin Cederlund, Torkel B Brismar and Raquel Themudo in Acta Radiologica Open
Supplemental Material
sj-vid-2-arr-10.1177 2058460118778068 -Supplemental material for Variable size of aortic subvalvular pseudoaneurysm
Supplemental material, sj-vid-2-arr-10.1177 2058460118778068 for Variable size of aortic subvalvular pseudoaneurysm by Anders Svensson, Kerstin Cederlund, Torkel B Brismar and Raquel Themudo in Acta Radiologica Open
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
Supplement videos are available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.