
Abstract
Background
The radiation dose for patients can be reduced with many methods and one way is to use abdominal compression. In this study, the radiation dose and image quality for a new patient-controlled compression device were compared with conventional compression and compression in the prone position.
Purpose
To compare radiation dose and image quality of patient-controlled compression compared with conventional and prone compression in general radiography.
Material and Methods
An experimental design with quantitative approach. After obtaining the approval of the ethics committee, a consecutive sample of 48 patients was examined with the standard clinical urography protocol. The radiation doses were measured as dose-area product and analyzed with a paired t-test. The image quality was evaluated by visual grading analysis. Four radiologists evaluated each image individually by scoring nine criteria modified from the European quality criteria for diagnostic radiographic images.
Results
There was no significant difference in radiation dose or image quality between conventional and patient-controlled compression. Prone position resulted in both higher dose and inferior image quality.
Conclusion
Patient-controlled compression gave similar dose levels as conventional compression and lower than prone compression. Image quality was similar with both patient-controlled and conventional compression and was judged to be better than in the prone position.
Introduction
All X-ray examinations shall be justified, optimized, and radiation doses be kept as low as reasonably achievable (ALARA) and image quality should be good enough to make an accurate diagnosis (1–4).The prime importance is to reduce the radiation dose to keep radiation morbidity from diagnostic imaging to a minimum (5).
Reduction of radiation doses and better image quality requires radiographers to use optimized methods such as compression (6,7). The image quality improves with compression because soft tissue is displaced sideways, a thinner body part requires less exposure, and scattered radiation is decreased (7).
Research has shown that compression of a few centimeters can reduce the radiation dose by half (7). Despite the benefits of compression, its use has been reduced in recent years in conventional X-ray examinations (3,7–10). A national Swedish report showed low use of compression of about 45% (10).
Traditionally, there are two methods to compress the patient’s abdomen in X-ray examinations. The one traditionally used is where the radiographer attaches a compression device on both sides of the examination table with a compression band across the abdomen of the patient. In this study, this is called “conventional compression.” The other method is the prone position with natural compression by the person’s weight. In the present study, a new method is evaluated. With this method, the patient presses a compression plate to the abdomen. This method will be referred to as “patient-controlled compression.”
A study has shown that in the supine position with compression, the pelvis region can compress 7–8 cm, independent of the thickness of the patient. In the prone position, self-compression in one study was 4 cm; however, for thin patients there was not the same effect (7). The most used compression method is the prone position because it is simple, but all examinations cannot be done with the patient in the prone position (11,12). However, studies have shown that the prone position reduces radiation dose in lumbar spine and abdominal examinations compared with the supine position without compression (9,11–14).
Because all X-ray examinations cannot be done in the prone position and because studies have indicated a low use of compression, a new patient-controlled compression device was evaluated in this study.
The purpose of this study was to compare radiation dose and image quality of patient-controlled compression compared with conventional and prone compression methods in general radiography.
Material and Methods
The regional Ethical Review Board has approved the study.
It was decided to test the device in urography, as no extra images would then be needed for the study.
Study device
The tested compression device is a prototype consisting of a 35 × 30 × 5 cm sheet of plastic with two handles.
Participants
A consecutive sample of urography patients were invited to participate in the study. The inclusion criteria were: outpatients who were referred for urography; and age 18–80 years. The exclusion criteria were: emergency patients; patients who could not participate actively; inability to understand the instructions or answer questions; and contraindication for compression or pregnancy.
Information about the study, invitation to participate, and a written consent form were sent together with the urography appointment. Verbal informed consent was obtained at the time of examination. The data were collected over a five-month period, between September 2015 and January 2016.
A power analysis based on a previous pilot study, of 20 urography examinations each containing two images, indicated that 43 patients would be required to achieve 90% power with 0.05 significance level at a standardized difference of 0.99 (15). To compensate for drop-outs, we aimed for 50 included patients in the study.
Imaging techniques
Patients were examined with the standard clinical urography protocol. The first study image was acquired in the supine position without contrast medium; the second image in the supine position 10 min after contrast injection (Fig. 1); directly after that, the third image was acquired in the prone position. All images were acquired within 15 min. All these images were acquired in the same way. The standard clinical settings for urography were tube potential = 70 kV (large patients = 75 kV) and automatic exposure control (AEC) for tube charge (mAs). These settings were identical for all three study images for the same patient. All images in the study were acquired using a source image receptor distance (SID) of 110 cm. The distance from the collimator to the front of the patient with and without compression was recorded with a measuring tape.
Example of a clinical image after contrast administration.
Three different types of compression were used, the first two in random order:
Conventional compression: patient supine with compression applied by the radiographer, anteroposterior (AP) projection. A compression band was attached to both sides of the examination table and strapped over the abdomen with an extra pillow under the band (Fig. 2a); Patient-controlled compression: patient supine, AP projection. Patient instructed to hold and press the plastic compression plate against the abdomen after inhalation. An extra pillow was used (Fig. 2b); Prone compression: patient lying prone without additional compression, posteroanterior projection.
Compression devices used in the study: (a) conventional compression and (b) patient-controlled compression.

The first two compressions were done in random order with a computer-generated block randomization with block size 10. The randomization information was placed in 50 sealed sequential envelopes. Prone position was always acquired as the last image.
Radiation dose measurements
All examinations were performed in the same examination room and with the same equipment (DRX-Evolution, Carestream Health, Rochester, NY, USA) with a flat panel detector (PaxScan Csl, Varian Medical Systems, Salt Lake City, UT, USA).
Parameters recorded for study purposes were: sex; age; height and weight; tube potential; tube charge; and field size. The staff involved had extra training to examine the study patients.
The radiation doses were measured as dose-area product (DAP) with a DAP-meter integrated in the equipment. The tube charge was also registered. All images were stored and reviewed in a PACS system (Sectra, Linköping, Sweden).
Image quality evaluation
The image quality of the three study images per patient (one with each of the two tested compression methods and one in prone position) was evaluated by visual grading analysis of the bony structures (16). The type of compression could not be deduced from the images; however, the image in the prone position could be recognized.
Four radiologists evaluated each image individually by scoring nine criteria modified from the European quality criteria for diagnostic radiographic images (17):
Visually sharp reproduction, as a single line, of the upper- and lower-plate surfaces in the centered beam area; Visually sharp reproduction of the pedicles; Reproduction of the intervertebral joints; Reproduction of the spinous and transverse processes; Visually sharp reproduction of the cortex and trabecular structures; Reproduction of the adjacent soft tissues, particularly the psoas shadows; Reproduction of the sacroiliac joints; This image has better image quality than the other two for the same patient; This image has worse image quality than the other two for the same patient.
Each criterion was given one of these scores: 0 = confident that the criterion is not fulfilled; 1 = somewhat confident that the criterion is not fulfilled; 2 = indecisive whether the criterion is fulfilled or not; 3 = somewhat confident that the criterion is fulfilled; or 4 = confident that the criterion is fulfilled.
Statistical analyses
The radiation dose data were reviewed for normal distribution with inspection of their distribution and by the Shapiro–Wilk test. If a skewed distribution was found, the analysis should be performed after logarithmic transformation. Radiation dose data were then analyzed with a paired t-test (15). Image quality data were analyzed with a generalized linear model with fixed factors (16,18). This results in an odds ratio (OR) for a pairwise comparison. Conventional compression was chosen as the reference method and the image quality for the other two methods were reported as compared to conventional compression. All analyses were performed with SPSS version 22 (IBM, Kista, Sweden).
Results
Sixty-four patients were invited to participate in the study. Two declined participation, seven did not fulfill the inclusion criteria, and five patients were excluded due to lack of time. One patient was excluded after randomization because of faulty examination parameters; for one patient the study protocol was lost.
Radiation dose data (average with SD) and geometric mean ratios with 95% CI between groups (n = 48 patients).

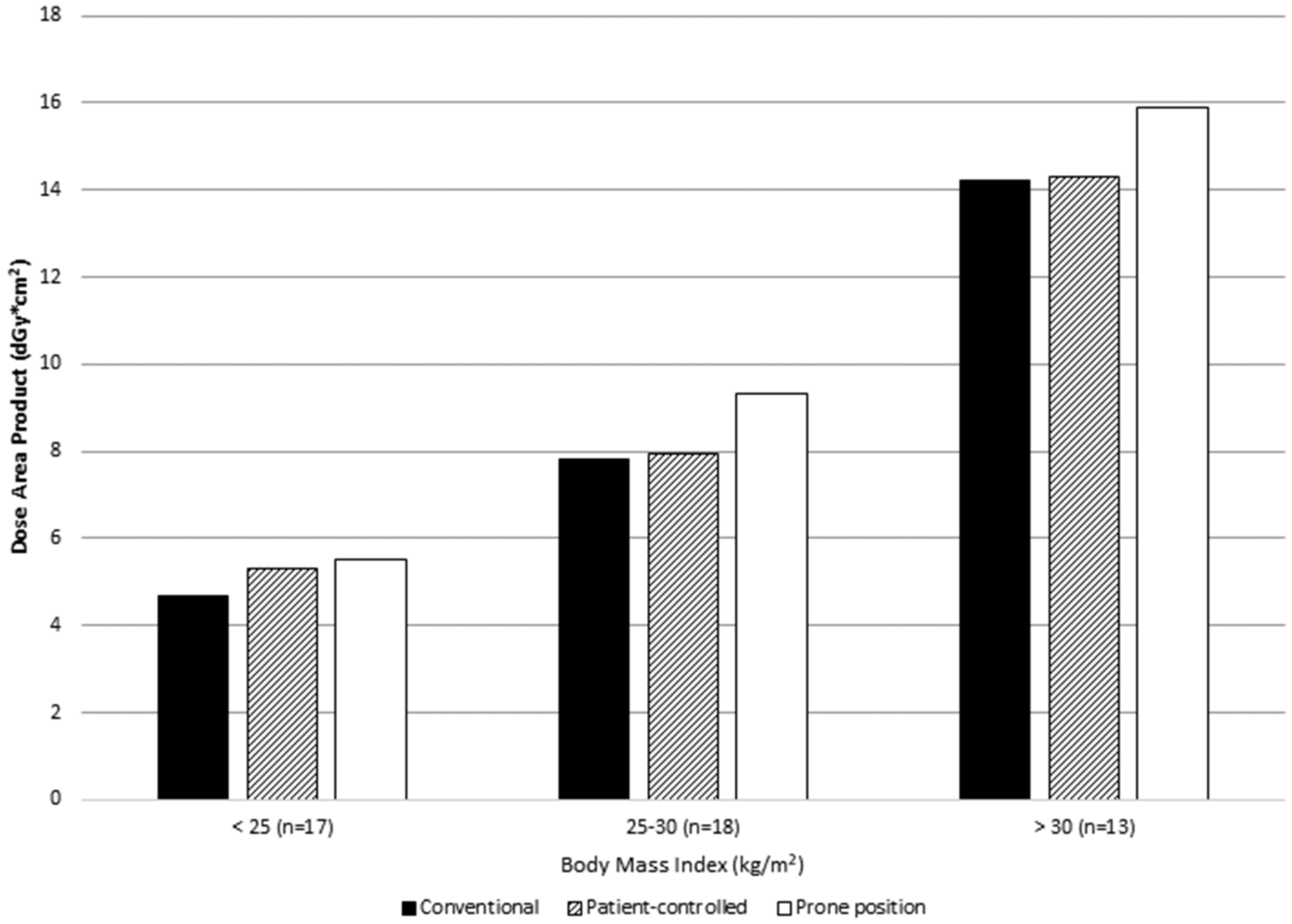
Dose-area product for three compression methods stratified by BMI.
Image quality
ORs (with 95% CIs) for image quality evaluation.

Conventional compression is reference and all ORs are for the comparison with this. An OR > 1 indicates higher scores for this criterion than reference.
Bold typeface indicates significant differences.
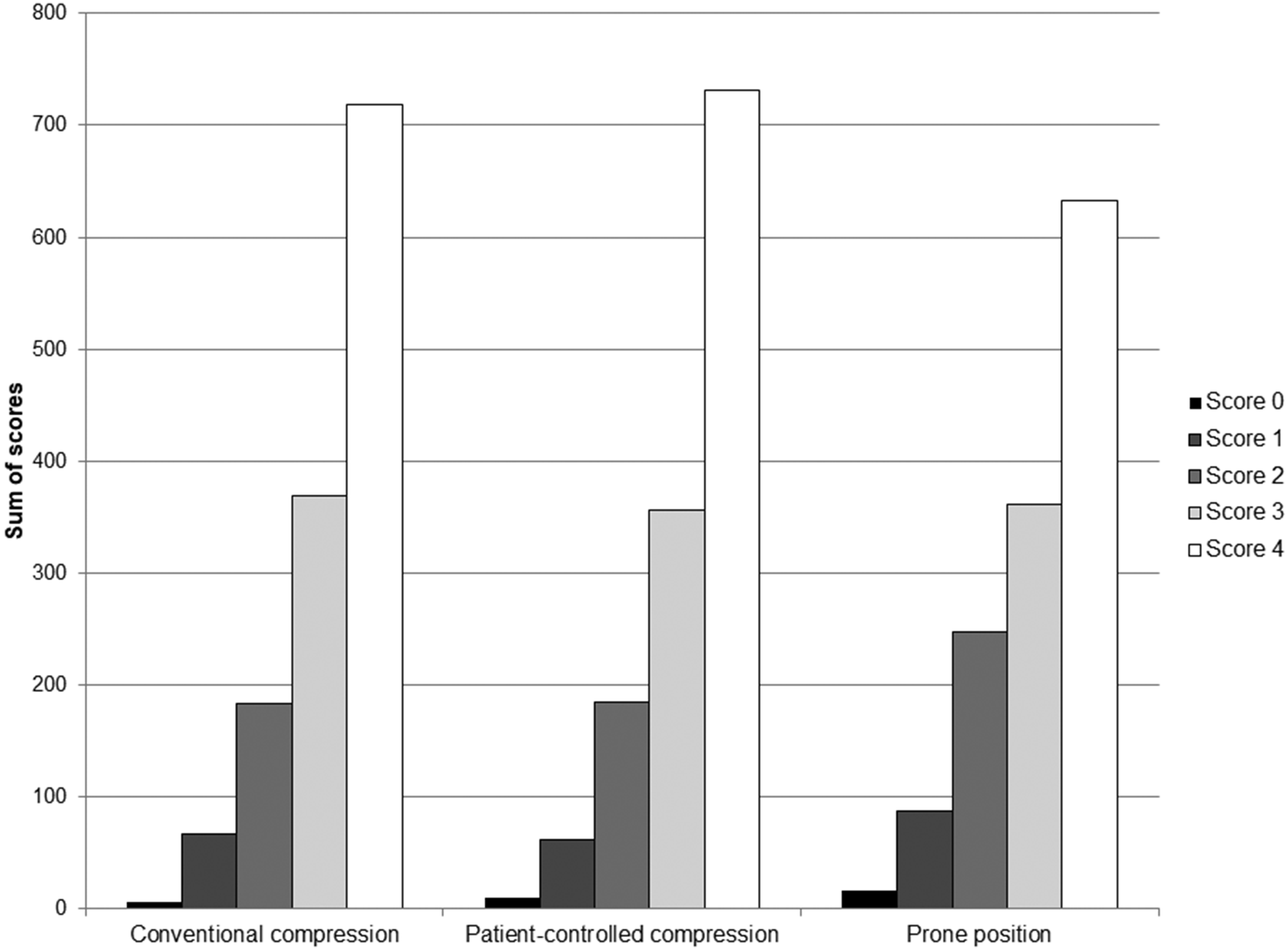
Distribution of image quality scores for three compression methods, criteria 1–7, and four observers combined (0 = lowest, 4 = highest).
There was a large variation between the four observers, with observers 1 and 2 giving scores mostly in the middle of the spectrum for criteria 1–7, average scores of 2.5 and 2.8 on the scale of 0–4. Observers 3 and 4 gave higher scores with average scores of 3.8 and 3.9. However, this difference was consistent throughout all seven criteria. All observers graded prone position as giving inferior image quality (Table 2).
Discussion
This study showed that radiation dose and image quality were similar for conventional compression and patient-controlled compression, and they were significantly better than prone compression.
There are only a few studies on abdominal compression and on different types of compression equipment in particular. A phantom study by Olsson et al. showed that by applying compression in the supine position, it was possible to compress the pelvis 7–8 cm, and by 4 cm in the prone position. There was no such effect for thin patients in the prone position. Radiation doses were estimated to be reduced by 50% or more by compression in the supine position (7). Our study shows that supine compression methods reduce radiation doses more than the prone position.
The prone position method is easy and quick to use but not all patients can lie prone nor can all examinations be done prone. Which compression method to use as standard depends on factors such as radiation dose, examination time, image quality, ergonomic considerations for the staff, comfort for the patient, and cost issues. Many studies have shown that the prone position reduced radiation dose more than the supine position in lumbar spine and abdominal examinations but these studies used the supine position without compression (9,11–14).
Radiographers have theoretical and practical knowledge about radiation safety principles and how to perform X-ray examinations with minimal radiation dose and high image quality. The application of compression is still not applied in practice to a satisfactory extent, which causes unnecessary high radiation doses (10). One reason why the use of compression is reduced could be requirements for higher productivity (7). Thus, it seems important to have an abdominal compression device that is easy to use and still effective. The minimization of radiation dose and high image quality for safer diagnosis is an important patient safety task.
We tested the three different compression methods at urography, as we did not want to expose the patient to any additional radiation just for the purpose of the study. Compression methods that reduce the radiation dose can be used in most radiographic examinations in the abdominal area. Patient-controlled compression can also be used with the patient standing or sitting when conventional compression is inconvenient. However, further studies are needed in this area as well as studies on time requirements for the various methods.
There was variation between observers in the image quality assessment. This might be due to different internal references for what is required to fulfil a criterion. However, the difference was consistent through the study. In the prone position, image quality was judged better for the sacroiliac joints. This might be due to the divergent X-ray beam giving better reproduction of this part.
Limitations with patient-controlled compression are that it is more sensitive for a limited ability to participate actively in an examination. For example, the ability to understand the given information or the ability to compress could have affected the degree of compression in the present study. In clinical use, there is a need for good information for radiographers to get optimal images when the patient-controlled compression plate is used.
Patient cooperation is very important when using patient-controlled compression, since it is the patient who decides how much compression to apply. Conventional compression is thus preferred when patients are judged unable to use the patient-controlled compression device. An advantage with patient-controlled compression is that it decreases the risk of too-high pressure, which might cause inconvenience for the patient.
Limitations to the study are that half of the compression images were acquired with and half without contrast media. Since only the bony structures were evaluated, this was not judged to be of great concern. It would also be interesting to compare “compression” with “no compression,” since the amount of total dose reduction is not clarified by the present study.
In conclusion, we found no significant difference in radiation dose or image quality between conventional compression and a new patient-controlled compression device. Both were superior to the prone position regarding lower dose and better image quality. Patient-controlled compression could thus be an alternative to conventional compression in general radiography.
Footnotes
Acknowledgements
The authors thank Stina Augustsson, Wolfgang Krauss, and Caroline Hagbohm for image quality evaluations. They also thank Anders Magnuson for his statistical assistance and the radiographers in their department who examined the study patients.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: OPH invented and designed the patient-controlled compression device. The radiographic procedures were therefore performed by radiographers in the radiology department as part of their daily work. Analysis of the data was done in close collaboration between the first author and the co-authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Research Committee of Region Örebro County and Örebro University, Sweden. The study is registered in ClinicalTrials.gov (NCT02622269).